Bimagrumab vs Follistatin: Myostatin Pathway Inhibitors for Muscle Growth
Comparison of bimagrumab and follistatin, two approaches to inhibiting the myostatin/activin pathway for muscle growth, body composition, and metabolic benefits.
Verdict at a Glance
Bimagrumab has substantially stronger clinical evidence, with multiple phase 2 trials demonstrating simultaneous fat loss and lean mass gain in humans. Its antibody format provides standardized dosing and a well- characterized safety profile. Follistatin is biologically compelling as a natural myostatin antagonist, but human evidence is limited to early gene therapy trials for muscular dystrophies. For anyone interested in myostatin pathway inhibition, bimagrumab represents the more clinically validated approach, while follistatin remains primarily a research tool.
| Best for | Pick | Why |
|---|---|---|
| Clinical Evidence for Body Composition | Bimagrumab | Phase 2b data in obesity/T2D demonstrated significant fat mass loss with simultaneous lean mass gain -- a combination rarely achieved by any single intervention. Human RCT data available. |
| Muscle Wasting Conditions | Bimagrumab | Studied in multiple muscle wasting indications including sarcopenia and inclusion body myositis with standardized dosing and safety monitoring. |
| Gene Therapy Approach | Follistatin | AAV1-follistatin gene therapy offers a one-time treatment approach for severe muscular dystrophies, providing sustained local follistatin expression without repeated dosing. |
| Natural Myostatin Regulation | Follistatin | Follistatin is the endogenous myostatin antagonist, offering a physiologically native approach to pathway modulation. It binds and sequesters myostatin directly rather than blocking receptor signaling. |
| Reproducible, Standardized Treatment | Bimagrumab | As a monoclonal antibody with established pharmaceutical manufacturing, bimagrumab offers consistent potency, well-defined pharmacokinetics, and regulatory-grade quality control. |
| Category | Bimagrumab | Follistatin | Advantage |
|---|---|---|---|
| Mechanism of Action | Fully human monoclonal antibody that blocks activin type II receptors (ActRII), preventing myostatin, activin A, and GDF-11 from signaling. Targets the receptor rather than individual ligands, providing broad inhibition of the TGF-beta muscle-wasting pathway. | Endogenous glycoprotein that acts as a natural antagonist of multiple TGF-beta superfamily ligands including myostatin, activin A, and GDF-11 by directly binding and sequestering them. Gene therapy (AAV- follistatin) and recombinant protein approaches both studied. | Comparable |
| Research Evidence | Multiple phase 2 clinical trials in humans including obesity/T2D (significant fat loss and lean mass gains), sarcopenia, and sporadic inclusion body myositis (sIBM). Phase 2b obesity trial showed simultaneous fat loss and muscle gain. | Primarily preclinical data and early-stage gene therapy trials. AAV1- follistatin gene therapy studied in Becker muscular dystrophy and inclusion body myositis (Mendell et al.). Limited human pharmacological data for recombinant follistatin. | Bimagrumab |
| Side Effect Profile | Involuntary muscle contractions and spasms are the most notable adverse effect. Mild diarrhea, acne, and injection-site reactions reported. Transient increases in FSH observed due to activin pathway inhibition. Generally well tolerated in clinical trials. | Limited human safety data. Gene therapy approaches carry standard AAV risks (immune response, durability concerns). Theoretical reproductive effects due to activin/FSH pathway involvement. Recombinant follistatin safety profile poorly characterized. | Bimagrumab |
| Dosing and Administration | Intravenous infusion or subcutaneous injection. Phase 2 trials used monthly IV infusions (10 mg/kg). Long half-life of antibody enables infrequent dosing. Standardized pharmaceutical production. | Gene therapy (AAV injection, one-time intramuscular) or recombinant protein (subcutaneous injection, research-only). No standardized dosing protocols. Gene therapy is irreversible; recombinant protein requires frequent dosing due to short half-life. | Bimagrumab |

Introduction#
Bimagrumab and follistatin represent two strategies for inhibiting the myostatin/activin signaling pathway to promote muscle growth and improve body composition. Both interfere with TGF-beta superfamily signaling that normally restrains muscle mass, but they operate through fundamentally different mechanisms and have vastly different levels of clinical evidence.
Bimagrumab (BYM338) is a fully human monoclonal antibody developed by Novartis that blocks activin type II receptors (ActRIIA and ActRIIB), preventing myostatin, activin A, and other TGF-beta ligands from signaling. It has been studied in multiple phase 2 clinical trials and generated significant interest for its ability to produce simultaneous fat loss and lean mass gain. Follistatin is an endogenous glycoprotein that naturally antagonizes myostatin by directly binding and sequestering it, and has been investigated primarily through gene therapy approaches for muscular dystrophies.
Mechanism of Action Comparison#
Bimagrumab#
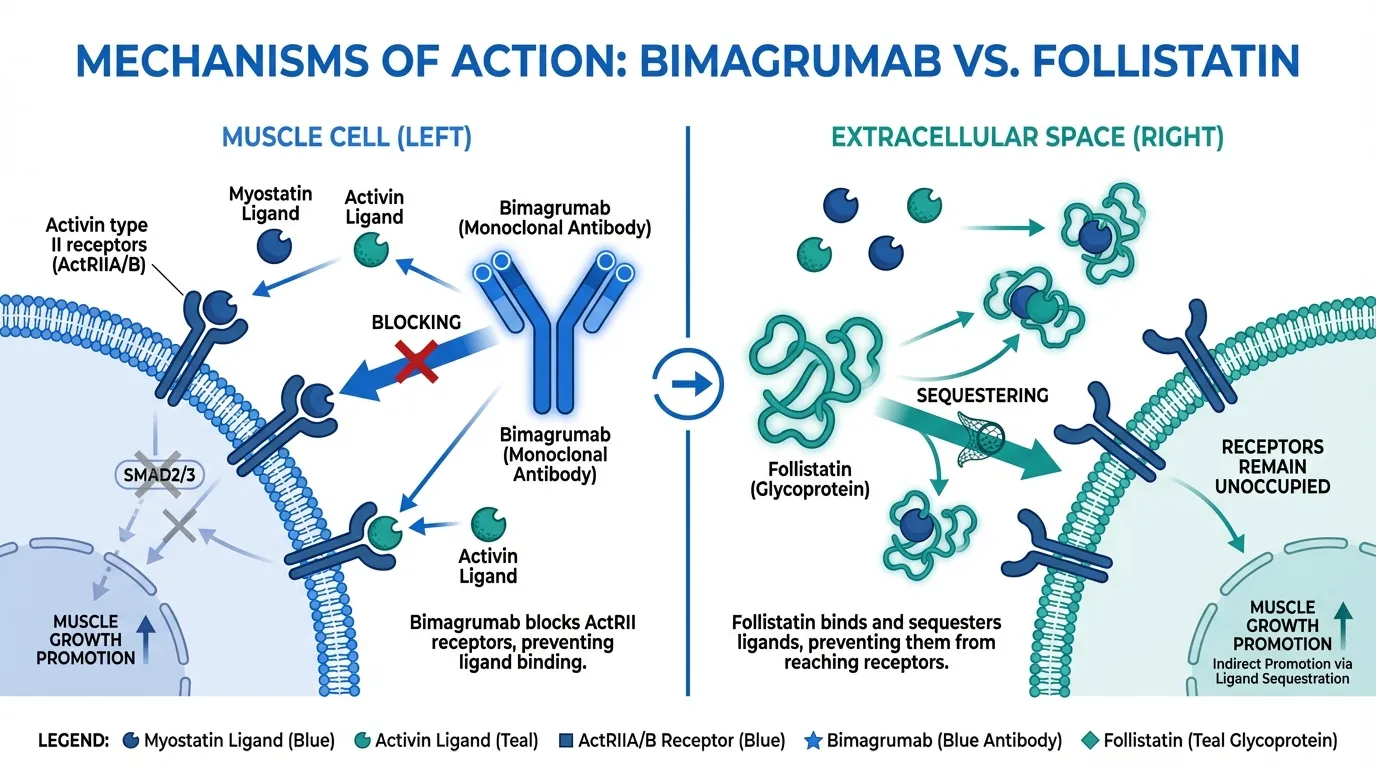
Bimagrumab blocks activin type II receptors (ActRIIA and ActRIIB) on the cell surface, preventing all ligands that signal through these receptors from activating downstream SMAD2/3 signaling. This provides broad inhibition because multiple TGF-beta superfamily members (myostatin/GDF-8, activin A, activin B, GDF-11) signal through these same receptors.
The downstream effect is removal of the brake on muscle protein synthesis, allowing muscle fibers to hypertrophy without the need for increased mechanical loading. Additionally, bimagrumab affects adipose tissue, promoting fat loss through mechanisms that may involve brown/beige adipocyte activation and improved metabolic signaling.
Follistatin#
Follistatin (FST) is a naturally occurring glycoprotein that acts as a ligand trap, directly binding myostatin, activin A, activin B, and other TGF-beta superfamily members in the extracellular space. By sequestering these ligands, follistatin prevents them from reaching and activating their receptors. Multiple follistatin isoforms exist (FST288, FST303, FST315), with different tissue distribution and binding properties.
Follistatin has been investigated through two approaches: AAV-mediated gene therapy (AAV1-FS344) for sustained local expression, and recombinant protein administration for systemic effects. The gene therapy approach provides sustained follistatin production from transduced muscle cells.
Mechanistic Comparison#
| Feature | Bimagrumab | Follistatin |
|---|---|---|
| Mechanism | Receptor blockade (ActRII) | Ligand sequestration (binds myostatin/activin) |
| Target specificity | Blocks all ActRII ligands | Binds multiple TGF-beta ligands |
| Drug format | Monoclonal antibody | Endogenous glycoprotein / gene therapy |
| Half-life | ~21 days (antibody) | Hours (recombinant) / sustained (gene therapy) |
| Reversibility | Reversible (drug washout) | Reversible (recombinant) / irreversible (gene therapy) |
| Effect on fat mass | Significant fat loss demonstrated | Not well characterized |
Dosing Comparison#
Bimagrumab Dosing#
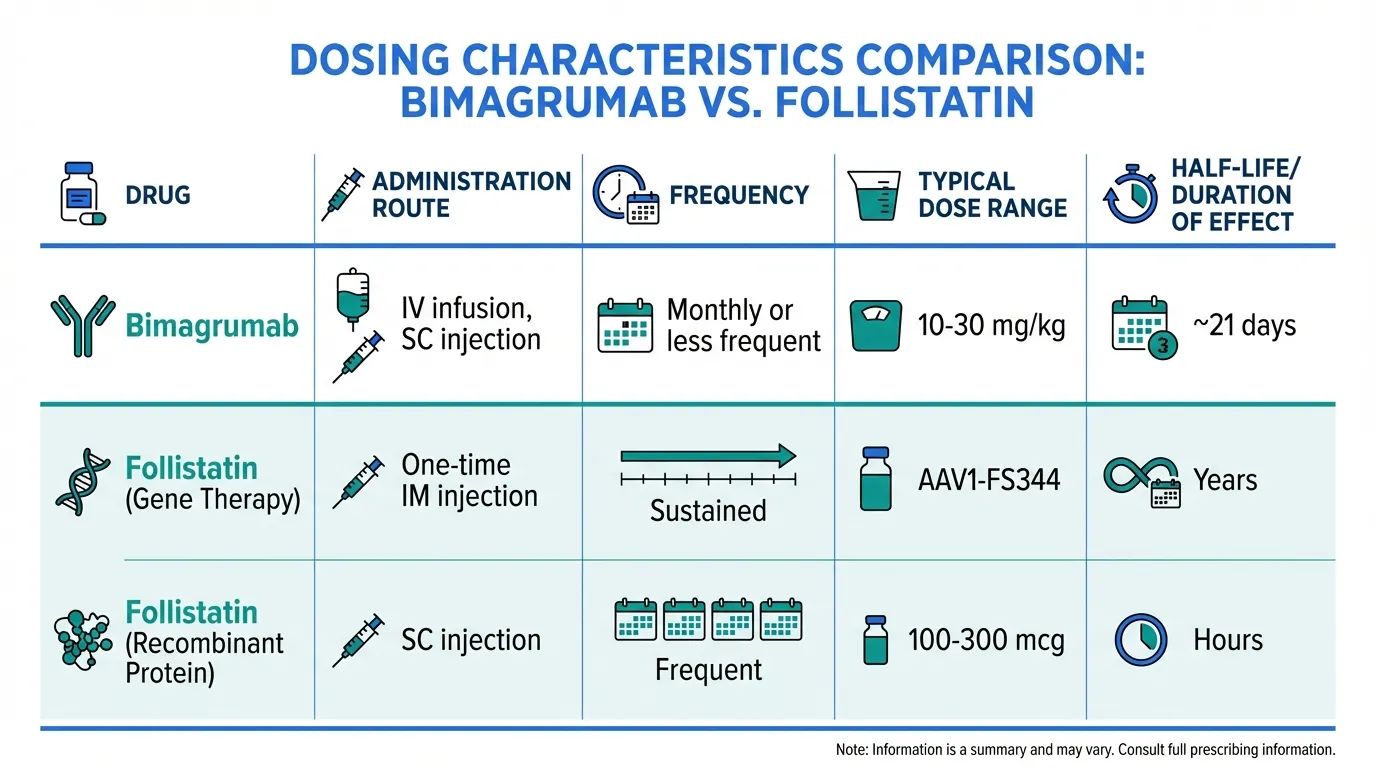
Bimagrumab has been administered as:
- IV infusion: 10 mg/kg monthly (phase 2 obesity trial, 48 weeks)
- IV infusion: 30 mg/kg single dose or monthly (phase 2 sarcopenia)
- Subcutaneous injection: Being explored for improved convenience
The antibody's ~21-day half-life enables monthly or less frequent dosing.
Follistatin Dosing#
Follistatin dosing varies by approach:
- Gene therapy (AAV1-FS344): One-time intramuscular injection into target muscles. Mendell et al. administered bilateral quadriceps injections in Becker muscular dystrophy patients
- Recombinant protein: No standardized dosing. Research protocols typically use 100-300 mcg subcutaneous injection. Short half-life requires frequent dosing
Side Effects Comparison#
Bimagrumab Side Effects#
The most notable adverse effect is involuntary muscle contractions and fasciculations, likely related to the change in muscle fiber properties from myostatin pathway inhibition. Mild diarrhea, acne, and injection-site reactions have been reported. Transient increases in FSH levels occur due to activin pathway involvement in reproductive hormone regulation, though this has not been associated with clinically significant reproductive effects in trial durations studied.
Follistatin Side Effects#
Human safety data for follistatin is limited. Gene therapy approaches carry standard AAV-vector risks including immune responses to the viral capsid, potential for insertional mutagenesis (though very low with AAV), and durability questions. Since follistatin inhibits activin signaling, theoretical concerns include effects on reproductive function (activin regulates FSH) and iron metabolism. These theoretical risks are poorly characterized because of the limited human data.
Research Evidence Comparison#
Bimagrumab Research#
- Obesity/T2D phase 2b: Heymsfield et al. demonstrated significant fat mass loss (-20.5%) with simultaneous lean mass gain (+3.6%) at 48 weeks in patients with obesity and T2D, despite no caloric restriction. This simultaneous recomposition effect is rare among single agents
- Sarcopenia: Phase 2 trial showed increases in lean mass in older adults with sarcopenia
- sIBM: Studied in sporadic inclusion body myositis, though primary endpoints were not met
- Body composition: Consistent increases in lean mass and decreases in fat mass across multiple indications
Evidence level: Moderate -- multiple phase 2 RCTs in humans with consistent body composition effects.
Follistatin Research#
- AAV1-FS344 gene therapy: Mendell et al. (PMID 28279643) studied intramuscular injection of AAV1-follistatin in Becker muscular dystrophy patients, demonstrating improvements in the 6-minute walk test
- sIBM gene therapy: AAV1-follistatin studied in inclusion body myositis with some evidence of stabilization
- Preclinical: Extensive animal data showing dramatic muscle hypertrophy with follistatin overexpression (the "mighty mouse" model)
- Recombinant protein: Minimal human clinical data
Evidence level: Low -- primarily preclinical and early gene therapy trials. No phase 2/3 RCTs for recombinant follistatin.
Key Differences Summary#
- Evidence maturity: Bimagrumab has multiple human RCTs. Follistatin has primarily preclinical data and early gene therapy trials.
- Drug format: Bimagrumab is a standardized pharmaceutical antibody. Follistatin is investigated as gene therapy or research-grade recombinant protein.
- Body composition: Bimagrumab has demonstrated simultaneous fat loss and lean mass gain in RCTs. Follistatin's effects on body composition in humans are poorly characterized.
- Reversibility: Bimagrumab effects are reversible with drug washout. AAV-follistatin gene therapy is irreversible.
- Mechanism level: Bimagrumab blocks at the receptor level (broad). Follistatin sequesters ligands in the extracellular space (also broad, but naturally regulated).
- Availability: Neither is FDA-approved. Bimagrumab is in clinical development. Recombinant follistatin is available through research suppliers but without standardized pharmaceutical quality.
Conclusion#
Bimagrumab is the clear leader in clinical evidence for myostatin pathway inhibition. Its phase 2b data showing simultaneous fat loss and muscle gain in obesity represents one of the most compelling body recomposition results from any single pharmacological agent. The monoclonal antibody format provides standardized manufacturing, reproducible pharmacokinetics, and a well-characterized safety profile.
Follistatin has a compelling biological rationale as the body's natural myostatin antagonist, and the gene therapy approach has shown promise in severe muscular dystrophies. However, for most applications related to muscle growth and body composition, the clinical data for follistatin is far less mature than bimagrumab.
Both approaches validate the fundamental concept that inhibiting myostatin/activin signaling promotes muscle growth and improves body composition. The choice between them depends on context: bimagrumab for clinical/pharmaceutical approaches with reversible dosing, and follistatin gene therapy for severe, irreversible muscular dystrophy interventions where sustained local expression is desired.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Clinical Evidence for Body Composition
Bimagrumab
Phase 2b data in obesity/T2D demonstrated significant fat mass loss with simultaneous lean mass gain -- a combination rarely achieved by any single intervention. Human RCT data available.
Muscle Wasting Conditions
Bimagrumab
Studied in multiple muscle wasting indications including sarcopenia and inclusion body myositis with standardized dosing and safety monitoring.
Gene Therapy Approach
Follistatin
AAV1-follistatin gene therapy offers a one-time treatment approach for severe muscular dystrophies, providing sustained local follistatin expression without repeated dosing.
Natural Myostatin Regulation
Follistatin
Follistatin is the endogenous myostatin antagonist, offering a physiologically native approach to pathway modulation. It binds and sequesters myostatin directly rather than blocking receptor signaling.
Reproducible, Standardized Treatment
Bimagrumab
As a monoclonal antibody with established pharmaceutical manufacturing, bimagrumab offers consistent potency, well-defined pharmacokinetics, and regulatory-grade quality control.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Bimagrumab vs Follistatin: Myostatin Pathway Inhibitors for Muscle Growth
Which is better, Bimagrumab or Follistatin?
Bimagrumab has substantially stronger clinical evidence, with multiple phase 2 trials demonstrating simultaneous fat loss and lean mass gain in humans. Its antibody format provides standardized dosing and a well- characterized safety profile. Follistatin is biologically compelling as a natural myostatin antagonist, but human evidence is limited to early gene therapy trials for muscular dystrophies. For anyone interested in myostatin pathway inhibition, bimagrumab represents the more clinicall... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Bimagrumab and Follistatin?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to Bimagrumab; Side Effect Profile: advantage goes to Bimagrumab. 1 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Bimagrumab over Follistatin?
For the scenario of "Clinical Evidence for Body Composition," research data suggests Bimagrumab may be more relevant. Phase 2b data in obesity/T2D demonstrated significant fat mass loss with simultaneous lean mass gain -- a combination rarely achieved by any single intervention. Human RCT data available.. This is based on currently available evidence and individual circumstances may differ.
How do Bimagrumab and Follistatin differ in their mechanisms of action?
Bimagrumab: Fully human monoclonal antibody that blocks activin type II receptors (ActRII), preventing myostatin, activin A, and GDF-11 from signaling. Targets the receptor rather than individual ligands, prov.... Follistatin: Endogenous glycoprotein that acts as a natural antagonist of multiple TGF-beta superfamily ligands including myostatin, activin A, and GDF-11 by directly binding and sequestering them. Gene therapy....
Which has fewer side effects, Bimagrumab or Follistatin?
In terms of side effects and tolerability, the advantage goes to Bimagrumab. Bimagrumab: Involuntary muscle contractions and spasms are the most notable adverse effect. Mild diarrhea, acne, and injection-site reactions reported. Transie.... Follistatin: Limited human safety data. Gene therapy approaches carry standard AAV risks (immune response, durability concerns). Theoretical reproductive effect....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.