GLP-1 Plus Amylin: Why Combination Therapy Is the Next Frontier

Introduction#
Among the many receptor combinations being explored for obesity treatment, the pairing of GLP-1 and amylin signaling has emerged as one of the most promising. Two drugs targeting this combination -- CagriSema and amycretin -- have produced weight loss exceeding 20%, rivaling or surpassing the dual GIP/GLP-1 agonist tirzepatide.
This article examines why amylin complements GLP-1 so effectively, the clinical evidence for each GLP-1/amylin approach, and how this combination may reshape obesity treatment.
Important: Only semaglutide and tirzepatide are FDA-approved for obesity. CagriSema has an NDA filed but is not yet approved. All other agents discussed are investigational.
What Is Amylin?#
Amylin (islet amyloid polypeptide, IAPP) is a 37-amino acid peptide hormone co-secreted with insulin by pancreatic beta cells after meals. It serves as a complementary satiety signal:
Amylin's Physiological Roles#
- Appetite suppression: Acts on the area postrema and nucleus tractus solitarius in the brainstem, distinct from GLP-1's hypothalamic targets
- Gastric emptying delay: Slows nutrient absorption (similar to but independent from GLP-1)
- Glucagon suppression: Reduces postprandial glucagon secretion
- Satiation signaling: Promotes meal termination ("I'm full" signals)
Why Amylin Complements GLP-1#
GLP-1 and amylin suppress appetite through different brain circuits:
| Feature | GLP-1 | Amylin |
|---|---|---|
| Primary brain target | Hypothalamus | Area postrema / brainstem |
| Appetite effect | Reduces hunger (tonic) | Promotes meal termination |
| Gastric emptying | Delays (via vagal) | Delays (via brainstem) |
| Glucagon suppression | Yes (via insulin) | Yes (direct) |
| Insulin secretion | Stimulates | Does not stimulate |
| Co-secreted with | Released from gut | Released from beta cells |
The key insight is that GLP-1 and amylin target different nodes in the appetite regulation network. Combining them produces additive or synergistic appetite suppression because the brain receives satiety signals from two independent pathways simultaneously.
The History: Pramlintide#
The First Amylin Analog#
Pramlintide (Symlin), approved by the FDA in 2005, was the first synthetic amylin analog. It validated the amylin pathway for metabolic control but had significant limitations:
- Indication: Adjunct to insulin in type 1 and type 2 diabetes (not approved for obesity)
- Dosing: Two to three injections daily (before each meal)
- Weight loss: Modest (~2-3% in trials)
- Hypoglycemia risk: When combined with insulin
- Formulation: Required separate injection from insulin
Pramlintide's inconvenient dosing schedule (multiple daily injections) and modest weight loss limited its clinical impact. However, it proved that amylin analogs could reduce appetite and body weight in humans.
Lessons from Pramlintide#
The pramlintide experience taught the field three key lessons:
- Amylin analogs work for appetite suppression but need longer half-lives
- Combining amylin with a GLP-1 agonist (rather than insulin) targets complementary pathways
- Weekly or less frequent dosing is essential for patient adherence
CagriSema: The Two-Drug Combination#
Components#
CagriSema is a fixed-dose combination of two separate molecules in a single weekly injection:
- Cagrilintide: A long-acting amylin analog (acylated for weekly dosing)
- Semaglutide: The established GLP-1 receptor agonist
Why Two Molecules?#
Using two separate peptides in combination allows each component to be independently optimized:
- Cagrilintide was developed specifically as a weekly amylin analog (unlike pramlintide's TID dosing)
- Semaglutide brings proven GLP-1 efficacy with extensive safety data
- The fixed-ratio combination simplifies dosing to a single injection
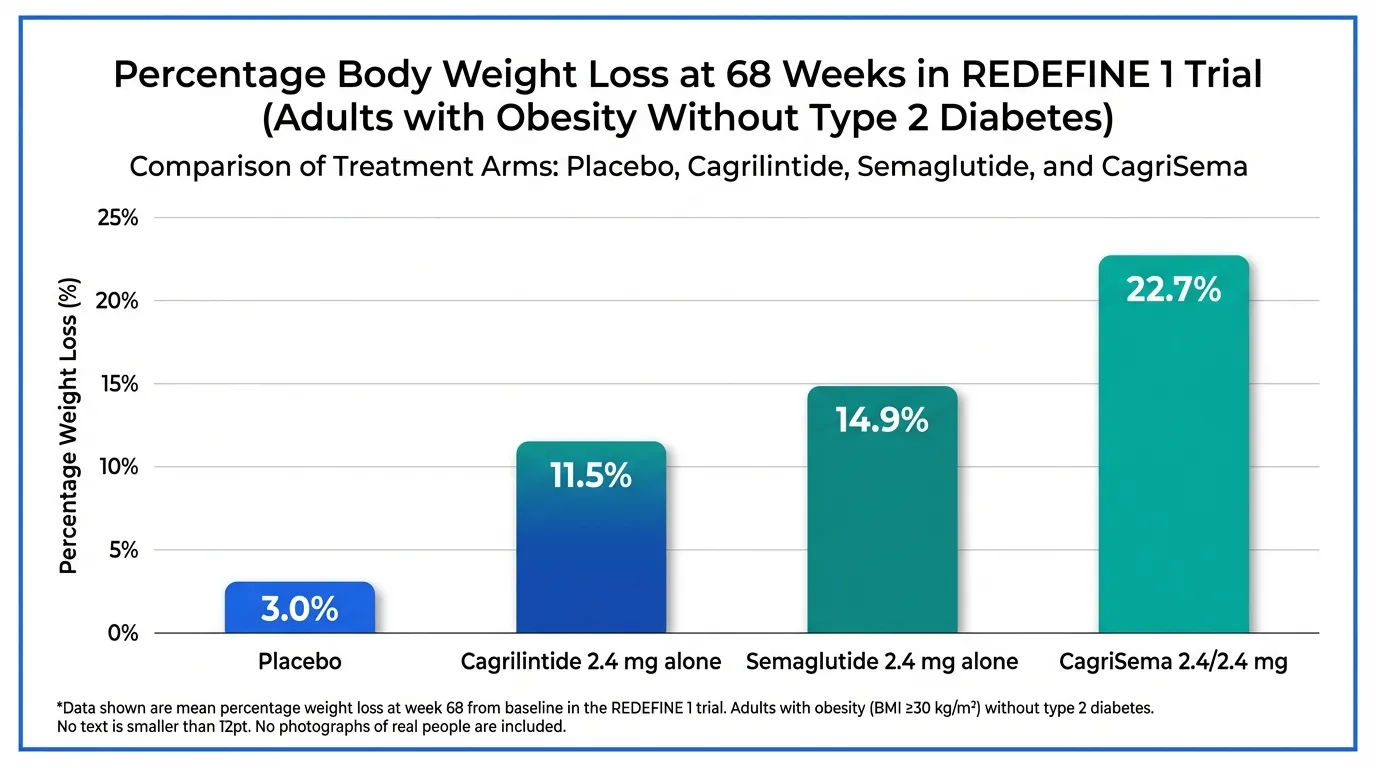
Phase 3 REDEFINE Results#
REDEFINE 1 (Adults without T2D, n=3,400):
| Arm | Weight Loss (68 wk) |
|---|---|
| CagriSema 2.4/2.4 mg | 22.7% (trial product) / 20.4% (treatment policy) |
| Cagrilintide 2.4 mg alone | 11.5% |
| Semaglutide 2.4 mg alone | 14.9% |
| Placebo | 3.0% |
The combination outperformed both components individually, confirming synergistic effects. Notably, cagrilintide alone (11.5%) produced meaningful weight loss as an amylin monotherapy, demonstrating the pathway's independent therapeutic value.
REDEFINE 2 (Adults with T2D, n=1,200):
- CagriSema: 15.7% weight loss at 68 weeks (trial product estimand)
- Placebo: 3.1%
- Also showed significant HbA1c reduction
Regulatory Status#
Novo Nordisk has filed an NDA with the FDA. If approved, CagriSema would be the first amylin-containing therapy approved for obesity and the first fixed-dose GLP-1/amylin combination.
Amycretin: The Unimolecular Approach#
A Single Molecule, Two Activities#
Amycretin takes a fundamentally different approach: instead of combining two separate peptides, it is a single 68-amino acid peptide engineered to activate both GLP-1 and amylin receptors simultaneously.
Design#
- Structure: 68-amino acid peptide with C18 diacid sidechain for albumin binding
- Half-life: Suitable for weekly SC dosing
- Molecular weight: ~8,000 Da
- Key modifications: Aib (aminoisobutyric acid) substitutions for DPP-4 resistance
- Oral formulation: Also in development with SNAC absorption enhancer
Clinical Data#
SC Phase 1b/2a (Lancet, 2025):
- 24.3% weight loss at 36 weeks (60 mg dose)
- Weight loss curve still declining at study end (no plateau)
- GI side effects: nausea 82%, vomiting 53%
- Overall discontinuation: 33% (but 59% of discontinuations were unrelated to AEs)
Oral Phase 1 (Lancet, 2025):
- 13.1% weight loss at 12 weeks
- Demonstrates oral amylin/GLP-1 co-agonism is feasible
Phase 2 in T2D:
- 448-patient study underway
- HbA1c reduction up to 14.5% weight loss at 36 weeks reported in November 2025
Amycretin vs CagriSema#
| Feature | Amycretin | CagriSema |
|---|---|---|
| Approach | Unimolecular | Two-drug combination |
| Components | Single peptide | Cagrilintide + semaglutide |
| Weight loss | 24.3% (36 wk) | 22.7% (68 wk) |
| Phase | Phase 2 | NDA filed |
| Oral option | Yes (Phase 1) | No |
| Company | Novo Nordisk | Novo Nordisk |
| Dosing | Weekly SC | Weekly SC |
| Manufacturing | Single molecule | Two molecules |
The weight loss trajectory of amycretin (24.3% at 36 weeks vs CagriSema's 22.7% at 68 weeks) suggests it may be significantly more potent, though direct comparison across different trial populations and durations is unreliable. Phase 2 and Phase 3 data will be needed to establish relative efficacy.
Petrelintide: The Amylin Monotherapy Foundation#
Development#
Petrelintide is a long-acting amylin analog being developed by Zealand Pharma in collaboration with Roche. It represents the next generation of amylin monotherapy:
- Dosing: Once weekly SC injection
- Phase: Phase 2b (ZUPREME-1 and ZUPREME-2)
- Partnership: Roche collaboration for co-development and co-commercialization
Phase 1b Data#
| Dose | Duration | Weight Loss |
|---|---|---|
| 0.6 mg weekly | 6 weeks | 5.3% |
| 1.2 mg weekly | 6 weeks | 5.1% |
| 2.4 mg weekly | 16 weeks | 4.8% |
| 4.8 mg weekly | 16 weeks | 8.6% |
| 9.0 mg weekly | 16 weeks | 8.3% |
| Pooled placebo | -- | 1.7% |
Why Amylin Monotherapy Matters#
Petrelintide is being developed as both a standalone therapy and a potential foundation for future combinations. The rationale for amylin monotherapy includes:
- Complementary mechanism: For patients who cannot tolerate GLP-1 agonists
- Combination potential: Could be paired with any GLP-1 agonist, including tirzepatide
- Tolerability: Amylin analogs may have different GI side effect profiles than GLP-1 agonists
- Lean mass preservation: Preclinical data suggest amylin analogs may preserve lean mass better than GLP-1 alone
ZUPREME Phase 2b Trials#
- ZUPREME-1: Adults with obesity without T2D, 42-week treatment, enrollment completed March 2025, results expected H1 2026
- ZUPREME-2: Adults with obesity with T2D, 28-week treatment, enrolled starting April 2025, results expected H2 2026
Cagrilintide: Amylin Alone#
Monotherapy Data#
Cagrilintide, the amylin component of CagriSema, has been studied as a monotherapy:
- REDEFINE 1: 11.5% weight loss at 68 weeks (2.4 mg weekly)
- This is notable because it demonstrates that amylin pathway activation alone produces clinically meaningful weight loss
Comparison to GLP-1 Monoagonism#
Cagrilintide's 11.5% weight loss as an amylin monotherapy is competitive with early GLP-1 agonists (liraglutide 3.0 mg achieved ~8% in SCALE), though below semaglutide 2.4 mg (14.9%). This establishes amylin as a legitimate independent pathway for obesity treatment.
The Science of Synergy#
Why GLP-1 + Amylin Exceeds the Sum of Parts#
The REDEFINE 1 data provide a clear demonstration of synergy:
- Cagrilintide alone: 11.5% weight loss
- Semaglutide alone: 14.9% weight loss
- Arithmetic sum: 26.4%
- CagriSema actual: 20.4% (treatment policy) / 22.7% (trial product)
While the combination does not fully achieve the arithmetic sum (likely due to overlapping mechanisms such as gastric emptying delay), it exceeds either component by a substantial margin. The ~6-8 percentage point increment over semaglutide alone confirms meaningful synergy.
Brainstem vs Hypothalamus#
The neuroanatomical basis for synergy lies in the separate brain regions targeted:
- GLP-1: Primarily activates neurons in the arcuate nucleus and paraventricular nucleus of the hypothalamus
- Amylin: Primarily activates neurons in the area postrema and nucleus of the solitary tract in the brainstem
By engaging both circuits simultaneously, the combination produces a more comprehensive suppression of appetite that is difficult to achieve by simply increasing the dose of either component alone.
Comparing Amylin-Based Approaches#
| Drug | Type | Weight Loss | Duration | Phase | Key Feature |
|---|---|---|---|---|---|
| Amycretin SC | Unimolecular GLP-1/amylin | 24.3% | 36 wk | Phase 2 | Highest single-molecule WL |
| CagriSema | Combo GLP-1 + amylin | 22.7% | 68 wk | NDA filed | Most advanced, proven synergy |
| Cagrilintide | Amylin monotherapy | 11.5% | 68 wk | Phase 3 | Validates amylin alone |
| Petrelintide | Amylin monotherapy | 8.6% | 16 wk | Phase 2 | Roche partnership, combo potential |
| Pramlintide | Amylin monotherapy | ~2-3% | varies | Approved (T1D/T2D) | Historical proof-of-concept |
Challenges and Open Questions#
Tolerability#
GI side effects are significant with dual GLP-1/amylin therapy. Amycretin SC showed 82% nausea and 53% vomiting in Phase 1b/2a. CagriSema's Phase 3 safety profile was described as consistent with the GLP-1 class, suggesting that the two-drug approach may have a tolerability advantage over the unimolecular approach by allowing independent dose titration.
Optimal Ratio#
For unimolecular co-agonists like amycretin, the ratio of GLP-1 to amylin activity is fixed. For combinations like CagriSema, the ratio is determined by the fixed-dose formulation. The optimal balance between the two pathways remains an active area of research.
Long-Term Durability#
Weight maintenance after discontinuation of GLP-1/amylin therapy is unknown. If amylin signaling provides additional appetite suppression through different neural circuits, it may improve weight maintenance compared to GLP-1 alone, but this hypothesis requires long-term studies.
Body Composition#
Whether amylin-based approaches preserve lean mass better than GLP-1 alone is a critical unanswered question. Preclinical data suggest potential advantages, but definitive clinical body composition data for CagriSema and amycretin are pending.
Conclusion#
The GLP-1/amylin combination represents one of the most promising directions in obesity pharmacotherapy. CagriSema's Phase 3 success and NDA filing validate the approach, while amycretin's extraordinary Phase 1b/2a results suggest even greater potential from a unimolecular design. The addition of amylin to GLP-1 signaling engages complementary brain circuits to produce appetite suppression that exceeds either pathway alone.
With CagriSema potentially reaching the market in 2026-2027 and amycretin advancing through Phase 2, the GLP-1/amylin axis is positioned to become a cornerstone of next-generation obesity treatment.
This article is for educational and informational purposes only. It does not constitute medical advice.
References#
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- CagriSema Overview and Research Guide
- CagriSema Dosing Protocols
- CagriSema Side Effects and Safety
- Amycretin Overview and Research Guide
- Amycretin Dosing Protocols
- Amycretin Side Effects and Safety
- Petrelintide Overview and Research Guide
- Petrelintide Dosing Protocols
- Petrelintide Side Effects and Safety
- Pramlintide Overview and Research Guide
- Pramlintide Dosing Protocols
- Pramlintide Side Effects and Safety
- Cagrilintide Overview and Research Guide
- Cagrilintide Dosing Protocols
- Cagrilintide Side Effects and Safety
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety

{kind=link}
Frequently Asked Questions About GLP-1 Plus Amylin: Why Combination Therapy Is the Next Frontier
What does this article cover?
A research review of GLP-1 and amylin combination therapy for obesity, covering CagriSema, amycretin, petrelintide, pramlintide, and the science behind dual appetite hormone targeting. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers CagriSema, Amycretin, Petrelintide, Pramlintide, Cagrilintide, Semaglutide. Key context: CagriSema (Phase 3 cagrilintide + semaglutide combination achieving 22.7% weight loss, NDA filed); Amycretin (Unimolecular GLP-1/amylin co-agonist with 24.3% weight loss at 36 weeks in Phase 1b/2a); Petrelintide (Long-acting amylin analog in Phase 2 as monotherapy and potential combination foundation). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: Phase 3 cagrilintide + semaglutide combination achieving 22.7% weight loss, NDA filed. Unimolecular GLP-1/amylin co-agonist with 24.3% weight loss at 36 weeks in Phase 1b/2a. Long-acting amylin analog in Phase 2 as monotherapy and potential combination foundation. These takeaways are based on the research data available at the time of publication.
What is CagriSema and why is it significant?
CagriSema is a peptide discussed in this article because: Phase 3 cagrilintide + semaglutide combination achieving 22.7% weight loss, NDA filed. For a complete profile of CagriSema, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Non-GLP-1 Approaches to Weight Loss: Amylin, Melanocortin, and Myostatin Pathways
A research review of non-GLP-1 peptide approaches to weight loss — amylin analogs (cagrilintide, petrelintide, pramlintide), melanocortin agonists (setmelanotide, bivamelagon), and anti-myostatin antibodies (bimagrumab).

The Evolution of GLP-1 Receptor Agonists: From Single-Target to Multi-Receptor Metabolic Therapeutics
A research review tracing the evolution of GLP-1 receptor agonists from semaglutide through tirzepatide, retatrutide, and survodutide, examining how multi-receptor approaches have progressively expanded efficacy in obesity and metabolic disease.

Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained
A comprehensive guide to every GLP-1 receptor agonist drug, from FDA-approved semaglutide and tirzepatide to pipeline therapies like retatrutide, amycretin, MariTide, and oral orforglipron.
You Might Also Like
Related content you may find interesting