Survodutide vs Tirzepatide: Comprehensive Comparison
A detailed comparison of Survodutide and Tirzepatide, two dual-agonist metabolic peptides with different receptor pairings -- glucagon/GLP-1 versus GIP/GLP-1 -- and their implications for weight loss, liver fat reduction, and metabolic disease.
Verdict at a Glance
Tirzepatide is the proven, FDA-approved option with superior weight loss data and established clinical use; Survodutide offers a differentiated mechanism via glucagon agonism with potential advantages for liver fat and MASH that await Phase 3 confirmation
| Best for | Pick | Why |
|---|---|---|
| Currently Available Obesity Treatment | Tirzepatide | FDA-approved as Zepbound with established dosing, safety monitoring, and commercial availability through standard prescribing channels |
| Non-Alcoholic Steatohepatitis (MASH) | Survodutide | Glucagon receptor agonism directly promotes hepatic fat oxidation and has shown significant liver fat reduction and histological improvement in Phase 2 MASH trials |
| Type 2 Diabetes with Obesity | Tirzepatide | Dual incretin mechanism provides potent glucose lowering alongside weight loss; FDA-approved for T2D with proven HbA1c reduction in SURPASS trials |
| Maximizing Energy Expenditure | Survodutide | Glucagon receptor activation increases resting energy expenditure and thermogenesis, providing a catabolic component absent from GIP/GLP-1 dual agonists |
| Patients with Hepatic Steatosis | Survodutide | The glucagon component uniquely drives hepatic lipid oxidation, potentially offering greater liver fat reduction than GIP/GLP-1 approaches |
| Category | Survodutide | Tirzepatide | Advantage |
|---|---|---|---|
| Receptor Pharmacology | Dual glucagon and GLP-1 receptor agonist; glucagon component drives hepatic fat oxidation and thermogenesis alongside GLP-1-mediated appetite suppression | Dual GIP and GLP-1 receptor agonist with approximately 5-fold GIP selectivity; GIP enhances insulin secretion and adipose tissue signaling | Comparable |
| Weight Loss Efficacy | Phase 2 data showed up to 18.7% body weight reduction at 46 weeks; Phase 3 trials ongoing | Up to 20.9% body weight reduction in SURMOUNT Phase 3 trials; FDA-approved for chronic weight management | Tirzepatide |
| Liver Fat Reduction | Strong hepatic fat reduction via glucagon receptor agonism; Phase 2 MASH trial showed significant liver fat decrease and histological improvement | Moderate hepatic fat reduction observed as secondary benefit; not specifically developed for liver indications | Survodutide |
| Regulatory Status | Phase 3 clinical trials by Boehringer Ingelheim for obesity and MASH; not yet approved | FDA-approved as Mounjaro (2022) for type 2 diabetes and Zepbound (2023) for obesity; widely available commercially | Tirzepatide |
| Side Effect Profile | GI side effects common; glucagon component may cause transient hyperglycemia and heart rate increase; dose-dependent tolerability | GI side effects well-characterized; extensive post-market safety data from millions of prescriptions; manageable with dose titration | Tirzepatide |
| Metabolic Mechanism Breadth | Glucagon promotes hepatic glycogenolysis, fat oxidation, thermogenesis, and energy expenditure; GLP-1 provides glucose-lowering counterbalance and satiety | GIP and GLP-1 provide complementary incretin effects on insulin secretion, appetite regulation, and glucose homeostasis | Comparable |

Introduction#
Survodutide and tirzepatide represent two distinct pharmacological strategies within the emerging class of multi-receptor metabolic peptide agonists. Both are dual agonists that include GLP-1 receptor activation, but they differ fundamentally in their second receptor target: survodutide pairs GLP-1 with glucagon receptor agonism, while tirzepatide pairs GLP-1 with GIP (glucose-dependent insulinotropic polypeptide) receptor agonism. This difference in receptor pairing creates meaningfully different metabolic profiles, particularly regarding hepatic fat metabolism, energy expenditure, and glycemic control.
Tirzepatide, developed by Eli Lilly, has already achieved FDA approval and commercial success as Mounjaro (type 2 diabetes) and Zepbound (obesity). Survodutide, developed by Boehringer Ingelheim, is in Phase 3 development with a particular focus on metabolic-associated steatohepatitis (MASH) in addition to obesity. This comparison examines how these different receptor strategies translate into clinical differences and which approach may be better suited for specific patient populations.
Mechanism of Action Comparison#
Survodutide#
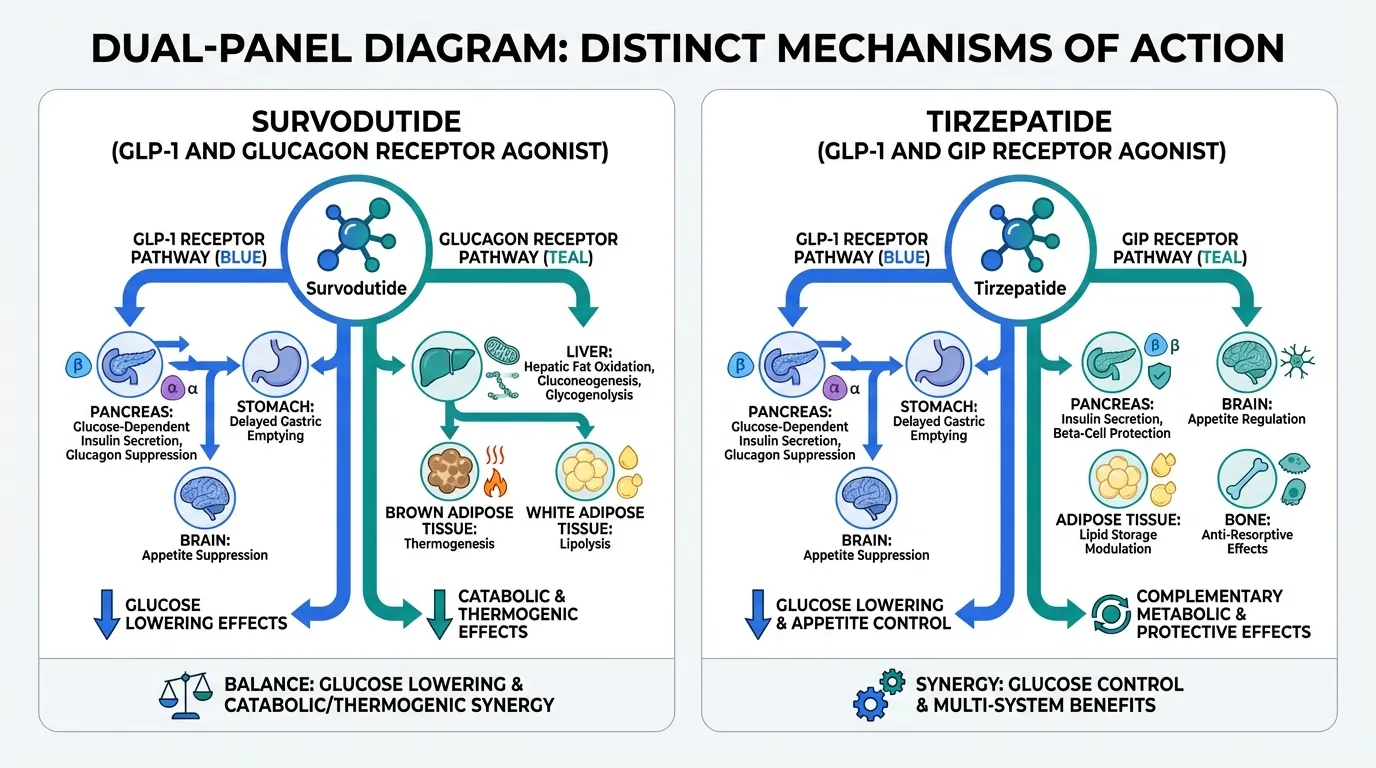
Survodutide (BI 456906) is a dual glucagon/GLP-1 receptor agonist with a molecular weight of 4170.6 Da. Its mechanism integrates two metabolically opposing yet complementary pathways:
GLP-1 receptor agonism provides the established incretin effects: glucose-dependent insulin secretion enhancement, suppression of inappropriate glucagon release from alpha cells, delayed gastric emptying, and central appetite suppression through hypothalamic and brainstem satiety circuits.
Glucagon receptor agonism introduces a catabolic metabolic component that is unique among current obesity therapeutics. Glucagon activates hepatic glycogenolysis and gluconeogenesis acutely, but its chronic effects are distinctly catabolic:
- Hepatic fat oxidation: Glucagon promotes beta-oxidation of fatty acids in the liver, directly reducing hepatic steatosis
- Thermogenesis: Glucagon increases resting energy expenditure through activation of brown adipose tissue and futile metabolic cycling
- Amino acid catabolism: Glucagon promotes hepatic amino acid uptake and ureagenesis
- Lipolysis: Glucagon stimulates adipose tissue lipolysis, mobilizing stored fat for oxidation
The critical pharmacological challenge with survodutide is balancing glucagon's hyperglycemic potential against GLP-1's glucose-lowering effects. The peptide's design achieves this through careful ratio optimization of glucagon-to-GLP-1 receptor activity, ensuring that the glucose-lowering effect of GLP-1 agonism predominates over glucagon's glycogenolytic action while preserving glucagon's catabolic benefits on fat metabolism and energy expenditure.
Tirzepatide#
Tirzepatide is a 39-amino acid peptide with a C20 fatty diacid moiety and a molecular weight of 4813.45 Da. It activates two incretin receptors:
GIP receptor agonism is the distinguishing feature of tirzepatide. GIP (glucose-dependent insulinotropic polypeptide) was historically considered primarily a glucose-dependent insulin secretagogue, but tirzepatide's development revealed additional metabolic roles:
- Central appetite regulation: GIP receptors in the hypothalamus and brainstem contribute to satiety signaling through pathways distinct from GLP-1
- Adipose tissue effects: GIP receptors on adipocytes modulate lipid storage and adipokine secretion
- Beta-cell protection: GIP signaling supports pancreatic beta-cell survival and proliferation
- Bone metabolism: GIP has anti-resorptive effects on bone, potentially mitigating osteoporosis risk during weight loss
GLP-1 receptor agonism provides complementary glucose-lowering and appetite-suppressing effects, as described above.
Tirzepatide demonstrates approximately 5-fold selectivity for GIP over GLP-1 receptors, making it a GIP-dominant dual agonist. This GIP predominance may partially explain its superior weight loss compared to pure GLP-1 agonists like semaglutide, as the two incretin pathways activate partially non-overlapping satiety mechanisms.
Dosing Comparison#
Survodutide Dosing#
Based on Phase 2 trial data and ongoing Phase 3 protocols:
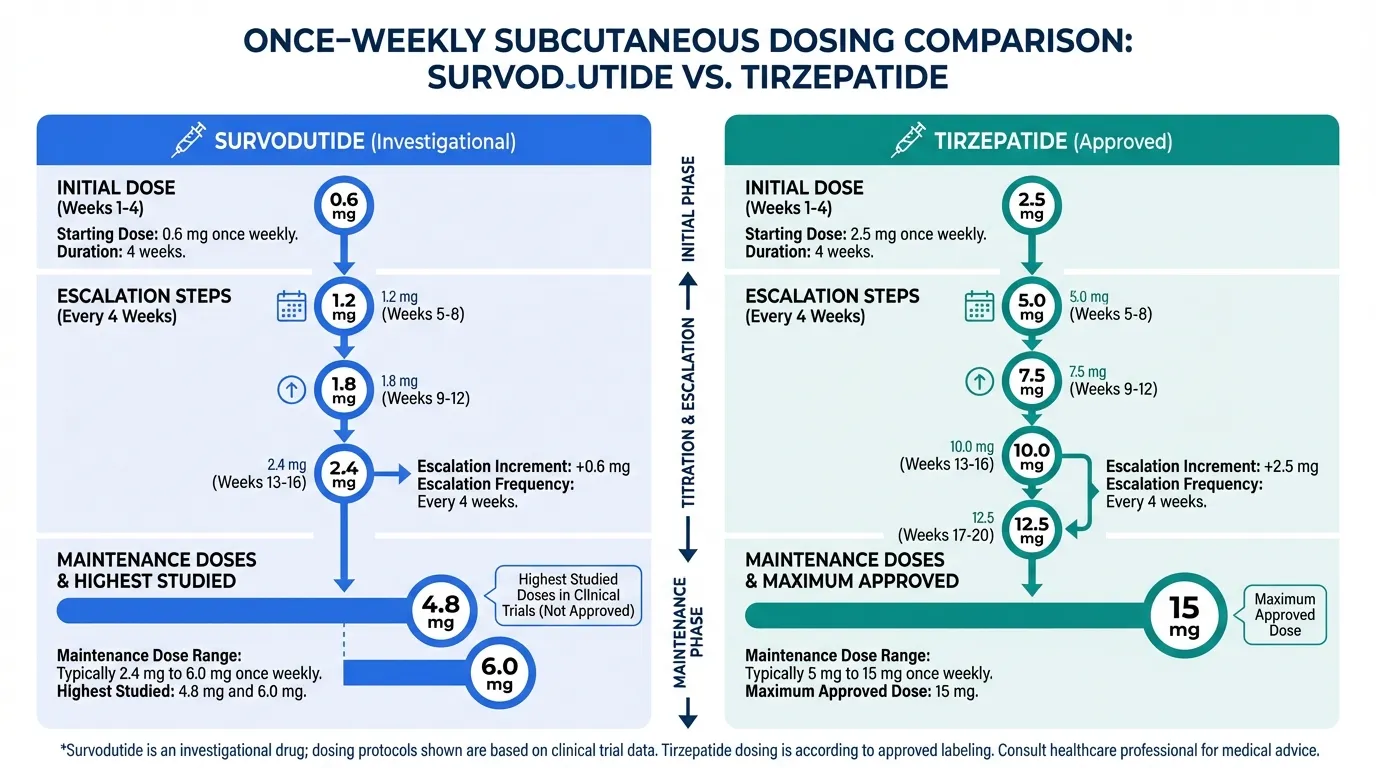
- Route: Once-weekly subcutaneous injection
- Dose escalation: Starting dose of 0.25 mg with gradual titration
- Maintenance doses studied: 2.4 mg, 4.8 mg, and 6.0 mg weekly in Phase 2
- Optimal dose: 4.8 mg and 6.0 mg showed greatest efficacy in Phase 2 weight loss trials
- MASH dosing: Similar dose range evaluated in hepatic endpoints trials
- Titration rationale: Gradual escalation minimizes GI side effects and allows metabolic adaptation to glucagon receptor activation
Tirzepatide Dosing#
FDA-approved dosing protocols:
- Route: Once-weekly subcutaneous injection
- Starting dose: 2.5 mg weekly for 4 weeks
- Dose escalation: Increase by 2.5 mg every 4 weeks as tolerated
- Maintenance doses: 5 mg, 10 mg, or 15 mg weekly
- Maximum dose: 15 mg weekly
- Formulation: Prefilled single-dose pens (Mounjaro/Zepbound) and prefilled syringes
- Storage: Refrigerated; room temperature stable for up to 21 days
Tirzepatide's well-established titration schedule, convenient delivery devices, and commercial manufacturing represent significant practical advantages over survodutide's investigational status.
Side Effects Comparison#
Survodutide Side Effects#
Phase 2 trial data revealed a side effect profile reflecting both GLP-1 and glucagon receptor activation:
- Gastrointestinal: Nausea (up to 41%), diarrhea (up to 21%), vomiting (up to 18%), decreased appetite -- consistent with GLP-1 agonist class effects
- Heart rate: Small transient increases observed, potentially related to glucagon-mediated sympathetic activation
- Hepatic: Transient aminotransferase elevations in some patients, though paradoxically liver fat was reduced
- Glucose: Glucagon's hyperglycemic potential appears adequately counterbalanced by GLP-1 in non-diabetic subjects, but careful monitoring is needed in diabetic patients
- Discontinuation rates: Dose-dependent, with higher discontinuation at the 6.0 mg dose
- Body composition: Some concern about lean mass loss at higher doses, a shared challenge with all potent weight loss therapies
Tirzepatide Side Effects#
Extensively characterized from Phase 3 clinical programs and post-market surveillance:
- Gastrointestinal: Nausea (12-33%), diarrhea (12-21%), vomiting (5-12%), constipation (6-11%) -- generally dose-dependent and improving with continued use
- Injection site reactions: Mild, reported in 2-5% of patients
- Pancreatitis: Rare (<0.2%); standard incretin class monitoring recommended
- Gallbladder events: Slightly elevated risk, consistent with rapid weight loss across all modalities
- Thyroid: C-cell tumor warning (class effect from preclinical GLP-1 agonist data); contraindicated in patients with personal/family history of medullary thyroid carcinoma
- Hypoglycemia: Low risk as monotherapy; increased when combined with insulin or sulfonylureas
Tirzepatide benefits from millions of patient-treatment-years of real-world safety data, providing confidence in its long-term safety profile that survodutide cannot yet match.
Research Evidence Comparison#
Survodutide Research#
Survodutide's clinical evidence is growing but remains primarily Phase 2:
- Phase 2 obesity trial: Randomized, dose-ranging study demonstrated up to 18.7% body weight loss at 46 weeks with the 4.8 mg dose, with dose-dependent efficacy across all arms
- Phase 2 MASH trial: Demonstrated significant reductions in liver fat content measured by MRI-PDFF, with histological improvement in MASH activity scores including inflammation and ballooning. A notable proportion of patients achieved MASH resolution without worsening fibrosis
- Phase 3 program: Multiple ongoing trials evaluating survodutide in obesity (SYNCHRONIZE program) and MASH, with topline results expected 2025-2026
- Mechanism studies: Preclinical data confirming glucagon-mediated hepatic fat oxidation, increased energy expenditure, and weight-independent improvements in liver histology
- Developer: Boehringer Ingelheim, which has positioned survodutide as a potential first-in-class treatment for MASH, a disease with limited approved therapies
Tirzepatide Research#
Tirzepatide has one of the most extensive clinical evidence bases of any metabolic peptide:
- SURPASS program (Type 2 diabetes): Five Phase 3 trials demonstrating superior HbA1c reduction versus insulin glargine (SURPASS-1), semaglutide 1 mg (SURPASS-2), insulin degludec (SURPASS-3), and insulin glargine + lispro (SURPASS-4). HbA1c reductions of 1.87-2.59% observed
- SURMOUNT program (Obesity): SURMOUNT-1 showed 20.9% weight loss at 72 weeks; SURMOUNT-2 confirmed efficacy in obese patients with T2D; SURMOUNT-3 and SURMOUNT-4 evaluated maintenance and sequential therapy
- SURPASS-CVOT: Cardiovascular outcomes trial evaluating major adverse cardiovascular events
- FDA approvals: Mounjaro (May 2022) for T2D; Zepbound (November 2023) for chronic weight management
- Real-world evidence: Growing body of post-market data confirming clinical trial efficacy translates to routine clinical practice
- Liver effects: Secondary analyses show moderate hepatic fat reduction, though tirzepatide was not specifically developed for liver disease
Key Differences Summary#
- Receptor pairing: Survodutide = glucagon + GLP-1; Tirzepatide = GIP + GLP-1
- Metabolic strategy: Survodutide adds catabolic/thermogenic mechanisms (glucagon); Tirzepatide adds incretin/anabolic mechanisms (GIP)
- Liver fat: Survodutide shows pronounced hepatic fat reduction through glucagon-driven oxidation; Tirzepatide shows moderate liver fat reduction
- Weight loss: Tirzepatide has demonstrated greater peak weight loss (20.9% Phase 3) vs survodutide (18.7% Phase 2), though direct comparison is limited by trial design differences
- Regulatory status: Tirzepatide is FDA-approved and commercially available; survodutide is in Phase 3 trials
- Developer: Survodutide by Boehringer Ingelheim; Tirzepatide by Eli Lilly
- Molecular weight: Survodutide 4170.6 Da; Tirzepatide 4813.45 Da
- Glycemic balance: Survodutide must counterbalance glucagon's hyperglycemic effect; Tirzepatide's dual incretin action is synergistically glucose-lowering
- MASH potential: Survodutide has specific MASH trial data; Tirzepatide's liver benefits are secondary observations
Conclusion#
Survodutide and tirzepatide embody two philosophically different approaches to multi-receptor metabolic therapy. Tirzepatide's GIP/GLP-1 dual agonism harnesses two complementary incretin pathways for potent glucose lowering and appetite suppression, and its FDA approval, extensive Phase 3 evidence, and growing real-world experience make it the established standard for obesity and type 2 diabetes treatment. For clinicians seeking a proven therapeutic option available today, tirzepatide is the clear choice.
Survodutide's glucagon/GLP-1 dual agonism offers a mechanistically distinct value proposition. The glucagon component provides hepatic fat oxidation, thermogenesis, and increased energy expenditure -- metabolic effects absent from GIP/GLP-1 approaches. This makes survodutide particularly compelling for patients with metabolic-associated steatohepatitis (MASH), where direct hepatic fat catabolism may provide benefits beyond weight loss alone. The Phase 2 MASH data showing histological improvement is especially notable given the limited therapeutic options for this condition.
The key question for survodutide's future is whether its Phase 3 trials will confirm the Phase 2 efficacy signals while demonstrating an acceptable safety profile, particularly regarding the glucagon component's effects on glucose homeostasis and heart rate. If successful, survodutide could carve out a distinct clinical niche as the preferred metabolic peptide for patients with concurrent obesity and liver disease, complementing tirzepatide's established role in broader metabolic disease management.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Currently Available Obesity Treatment
Tirzepatide
FDA-approved as Zepbound with established dosing, safety monitoring, and commercial availability through standard prescribing channels
Non-Alcoholic Steatohepatitis (MASH)
Survodutide
Glucagon receptor agonism directly promotes hepatic fat oxidation and has shown significant liver fat reduction and histological improvement in Phase 2 MASH trials
Type 2 Diabetes with Obesity
Tirzepatide
Dual incretin mechanism provides potent glucose lowering alongside weight loss; FDA-approved for T2D with proven HbA1c reduction in SURPASS trials
Maximizing Energy Expenditure
Survodutide
Glucagon receptor activation increases resting energy expenditure and thermogenesis, providing a catabolic component absent from GIP/GLP-1 dual agonists
Patients with Hepatic Steatosis
Survodutide
The glucagon component uniquely drives hepatic lipid oxidation, potentially offering greater liver fat reduction than GIP/GLP-1 approaches
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Survodutide vs Tirzepatide: Comprehensive Comparison
What are the key differences between Survodutide and Tirzepatide?
The main differences across comparison categories are: Receptor Pharmacology: advantage goes to neither (tie); Weight Loss Efficacy: advantage goes to Tirzepatide; Liver Fat Reduction: advantage goes to Survodutide. 3 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Tirzepatide over Survodutide?
For the scenario of "Currently Available Obesity Treatment," research data suggests Tirzepatide may be more relevant. FDA-approved as Zepbound with established dosing, safety monitoring, and commercial availability through standard prescribing channels. This is based on currently available evidence and individual circumstances may differ.
How do Survodutide and Tirzepatide differ in their mechanisms of action?
Survodutide: Glucagon promotes hepatic glycogenolysis, fat oxidation, thermogenesis, and energy expenditure; GLP-1 provides glucose-lowering counterbalance and satiety. Tirzepatide: GIP and GLP-1 provide complementary incretin effects on insulin secretion, appetite regulation, and glucose homeostasis.
Which has fewer side effects, Survodutide or Tirzepatide?
In terms of side effects and tolerability, the advantage goes to Tirzepatide. Survodutide: GI side effects common; glucagon component may cause transient hyperglycemia and heart rate increase; dose-dependent tolerability. Tirzepatide: GI side effects well-characterized; extensive post-market safety data from millions of prescriptions; manageable with dose titration.
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.