Amycretin vs Tirzepatide: Emerging GLP-1/Amylin vs Approved GIP/GLP-1
Evidence-based comparison of amycretin (unimolecular GLP-1/amylin) and tirzepatide (dual GIP/GLP-1) for obesity, including early-phase vs Phase 3 data.
Verdict at a Glance
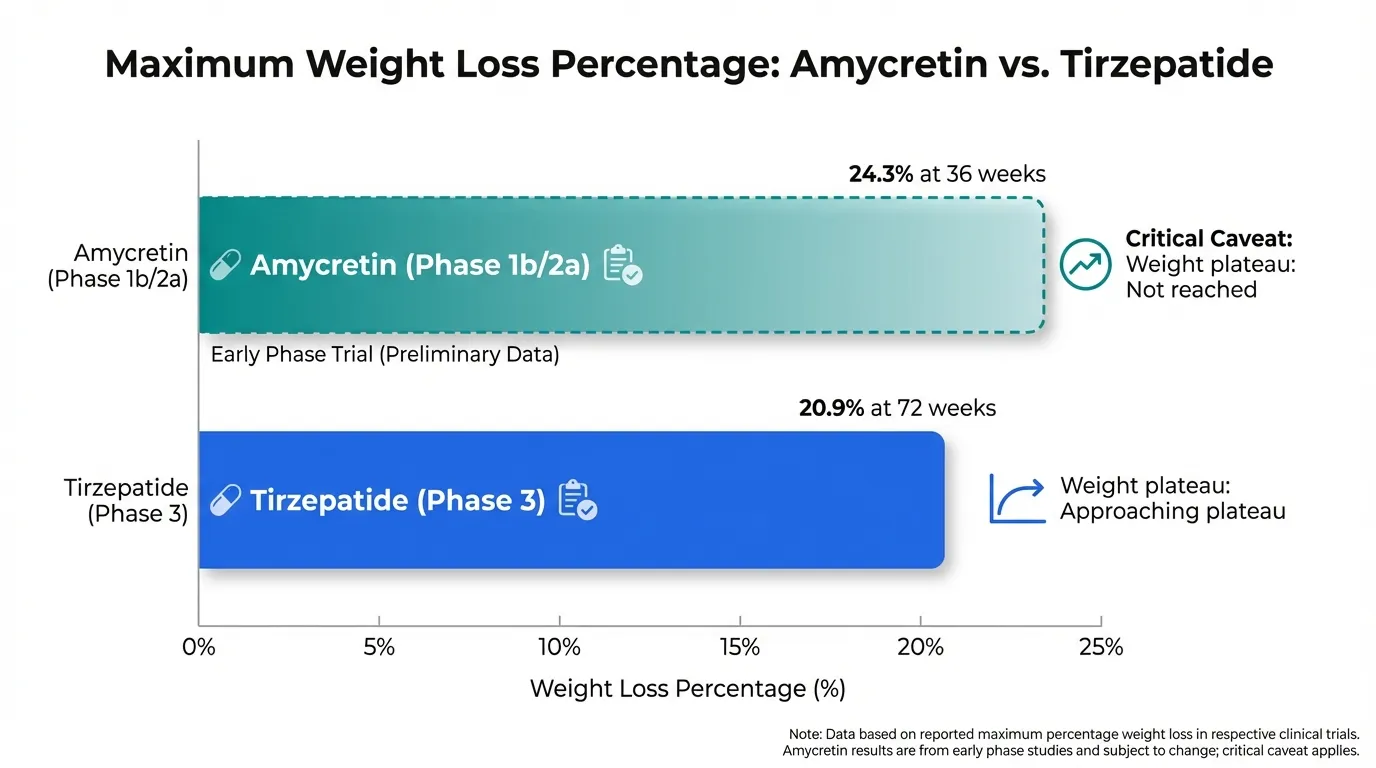
Amycretin's early-phase data (24.3% weight loss at 36 weeks, no plateau) suggest it could substantially exceed tirzepatide's 20.9%, potentially becoming the most effective anti-obesity agent ever tested. However, this comparison is fundamentally unequal: amycretin's results come from 125 patients over 36 weeks, while tirzepatide's come from thousands of patients over 72 weeks in rigorous Phase 3 trials. Early-phase weight loss often diminishes in larger trials. Tirzepatide is FDA-approved and available today. Amycretin's promise must be confirmed in Phase 3 before definitive conclusions can be drawn.
| Best for | Pick | Why |
|---|---|---|
| Treatment Available Now | Tirzepatide | Tirzepatide is FDA-approved and available as Mounjaro/Zepbound. Amycretin is years from potential approval. For patients who need treatment today, tirzepatide is the only option. |
| Maximum Weight Loss (Proven) | Tirzepatide | With 20.9% weight loss at 15 mg in SURMOUNT-1, tirzepatide is the most effective approved anti-obesity medication, supported by thousands of patients across multiple Phase 3 trials. |
| Maximum Weight Loss Potential (Future) | Amycretin | If Phase 3 confirms the 24.3% weight loss seen in Phase 1b/2a (with no plateau at 36 weeks), amycretin could become the most effective obesity treatment ever developed. |
| Oral Treatment Option (Future) | Amycretin | Amycretin has an oral formulation in development without fasting restrictions. Tirzepatide has no oral formulation, making amycretin the only dual-agonist option with oral potential. |
| Type 2 Diabetes | Tirzepatide | Five SURPASS trials with 9,000+ patients, FDA approval, and demonstrated superiority over semaglutide. Amycretin's T2D data is limited to Phase 2. |
| Category | Amycretin | Tirzepatide | Advantage |
|---|---|---|---|
| Mechanism of Action | Unimolecular dual GLP-1 and amylin receptor agonist. Single molecule combining two satiety pathways. Amylin component provides brainstem appetite suppression and leptin resensitization. | Dual GIP and GLP-1 receptor agonist. Single 39-amino acid molecule with ~5-fold potency at GIPR relative to native GIP. Synergistic incretin activation for insulin secretion and appetite suppression. | Comparable |
| Weight Loss Efficacy | Phase 1b/2a showed up to 24.3% weight loss at highest SC dose at 36 weeks, with no plateau observed. If the weight loss trajectory continues, final efficacy could be substantially higher. | SURMOUNT-1 demonstrated 20.9% mean weight loss at 15 mg at 72 weeks. Up to 36% achieved 25% or more weight loss. Largest FDA-approved weight loss of any medication. | Amycretin |
| Development Stage and Evidence | Phase 1b/2a completed (125 patients, 36 weeks, Lancet). Phase 2 in T2D completed (448 patients). Phase 3 entering for obesity and T2D. Earliest approval years away. | FDA-approved 2022. SURPASS (5 T2D trials, 9,000+ patients) and SURMOUNT (obesity trials). Head-to-head superiority over semaglutide (SURPASS-2). Growing real-world safety experience. | Tirzepatide |
| Formulation Options | Both subcutaneous weekly and oral daily formulations in development. Oral formulation does not require fasting restrictions. Both showed efficacy in Phase 2 T2D trial. | Once-weekly subcutaneous injection only. No oral formulation available or in advanced development. Six dose strengths (2.5-15 mg) with hidden-needle pens. | Amycretin |
| Safety Profile | GI adverse events most common, consistent with GLP-1/amylin class. High frequency of GI events in early trials. Limited to <600 total participants. No long-term or cardiovascular data. | Well-characterized GI profile (nausea 12-33%, diarrhea 12-21%). FDA-approved with growing post-marketing experience. CVOT underway. Lower GI rates than semaglutide at equivalent efficacy. | Tirzepatide |

Introduction#
Amycretin (Novo Nordisk) and tirzepatide (Eli Lilly) represent the cutting edge of dual-mechanism obesity treatment, but from vastly different stages of development. Tirzepatide is the established leader, FDA-approved and producing the highest weight loss of any approved medication (20.9%). Amycretin is the most promising pipeline candidate, with early-phase data suggesting 24.3% weight loss at 36 weeks -- with no plateau in sight.
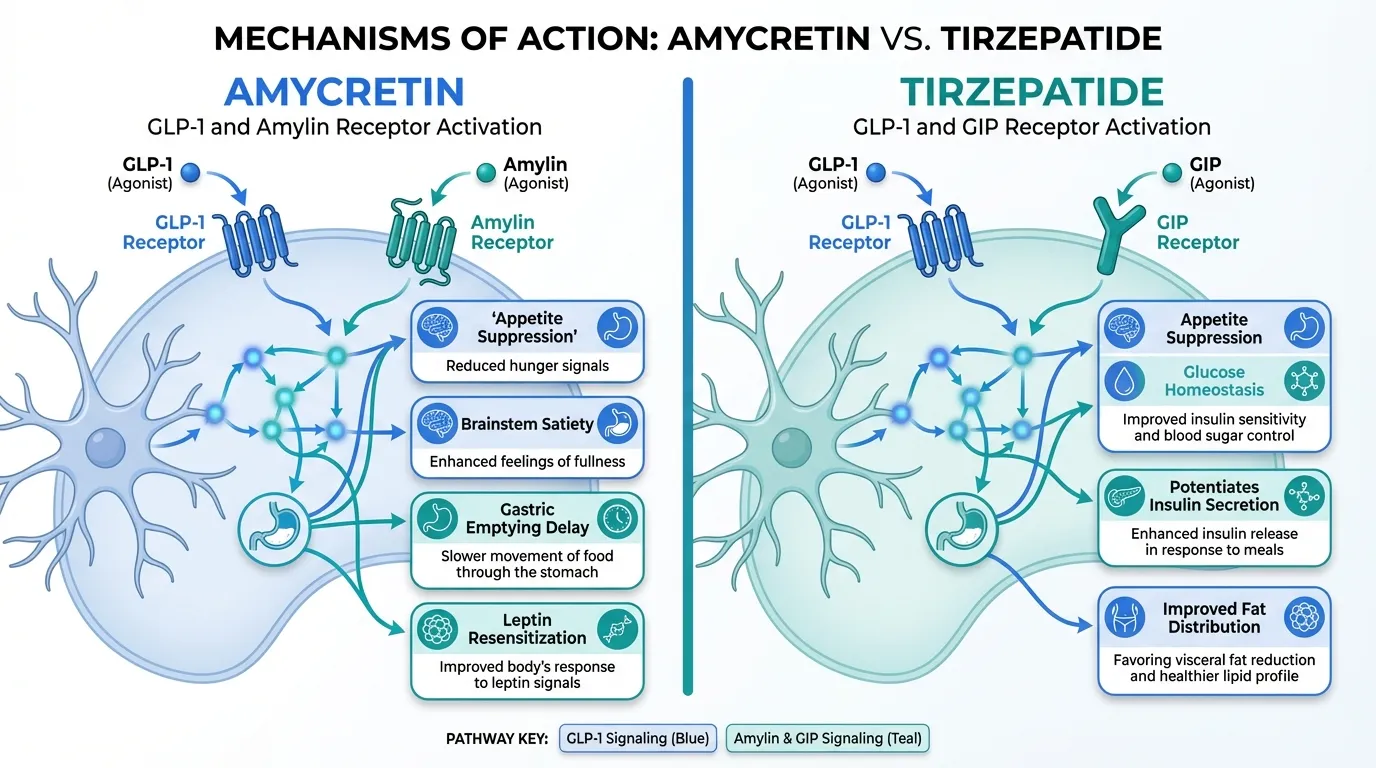
Both combine GLP-1 agonism with a second pathway, but the complementary mechanisms differ fundamentally: amycretin pairs GLP-1 with amylin receptor agonism, while tirzepatide pairs GLP-1 with GIP receptor agonism.
Mechanism of Action Comparison#
Amycretin#
Amycretin is a unimolecular peptide that simultaneously activates GLP-1 receptors (appetite suppression, glucose homeostasis) and amylin receptors (brainstem satiety, gastric emptying delay, leptin resensitization). The amylin pathway is particularly relevant for sustained weight loss, as leptin resensitization may help overcome the weight loss plateaus seen with GLP-1-only agents.
Tirzepatide#
Tirzepatide is a 39-amino acid single molecule that simultaneously activates GIP and GLP-1 receptors. GIP receptor activation potentiates insulin secretion, may improve fat distribution, and provides complementary appetite suppression through distinct central pathways.
Two Different Second Pathways#
| Feature | Amycretin | Tirzepatide |
|---|---|---|
| Primary pathway | GLP-1 agonism | GLP-1 agonism |
| Second pathway | Amylin agonism | GIP agonism |
| Molecule type | Unimolecular peptide | Unimolecular peptide |
| Leptin sensitization | Yes (via amylin) | Not established |
| Incretin enhancement | Via GLP-1 only | Via GLP-1 + GIP |
| Oral formulation | In development | Not available |
Weight Loss Data#
| Parameter | Amycretin (Phase 1b/2a) | Tirzepatide (SURMOUNT-1) |
|---|---|---|
| Weight loss (max dose) | Up to 24.3% | 20.9% |
| Duration | 36 weeks | 72 weeks |
| Sample size | 125 patients | 2,539 patients |
| Trial phase | Phase 1b/2a | Phase 3 |
| Weight plateau | Not reached | Approaching plateau |
| Publication | The Lancet | NEJM |
Critical caveat: Comparing Phase 1b/2a data (small, short) to Phase 3 data (large, long) is methodologically inappropriate. Weight loss often diminishes in larger, longer trials with more diverse populations. Amycretin's 24.3% figure must be confirmed in Phase 3.
Safety Comparison#
| Parameter | Amycretin | Tirzepatide |
|---|---|---|
| Total patients studied | <600 | 14,000+ |
| GI events | High frequency | Nausea 12-33% |
| Severity | Mostly mild-moderate | Mostly mild-moderate |
| Long-term data | None | Growing (2+ years) |
| CV outcomes | None | CVOT pending |
Key Differences Summary#
- Weight loss: Amycretin 24.3% (Phase 1b, 36 wk) vs tirzepatide 20.9% (Phase 3, 72 wk)
- Evidence maturity: Phase 1b/2a vs FDA-approved Phase 3
- Second mechanism: Amylin (amycretin) vs GIP (tirzepatide)
- Formulations: SC + oral (amycretin) vs SC only (tirzepatide)
- Availability: Years away vs available now
- Manufacturer: Both competing for market leadership (Novo Nordisk vs Eli Lilly)
Conclusion#
This comparison ultimately pits promise against proof. Amycretin's Phase 1b/2a results are the most impressive early-phase weight loss data ever reported, and the dual GLP-1/amylin mechanism with both injectable and oral options positions it as potentially transformative. But tirzepatide is real, available, and proven in thousands of patients. Until amycretin's Phase 3 results are reported, tirzepatide remains the evidence-based choice for maximum weight loss. If amycretin's Phase 3 confirms its early promise, the obesity treatment landscape could shift dramatically.
Detailed Category Analysis#
Mechanism of Action#
Amycretin: Unimolecular dual GLP-1 and amylin receptor agonist. Single molecule combining two satiety pathways. Amylin component provides brainstem appetite suppression and leptin resensitization.
Tirzepatide: Dual GIP and GLP-1 receptor agonist. Single 39-amino acid molecule with ~5-fold potency at GIPR relative to native GIP. Synergistic incretin activation for insulin secretion and appetite suppression.
Advantage: Neither (tie)
Weight Loss Efficacy#
Amycretin: Phase 1b/2a showed up to 24.3% weight loss at highest SC dose at 36 weeks, with no plateau observed. If the weight loss trajectory continues, final efficacy could be substantially higher.
Tirzepatide: SURMOUNT-1 demonstrated 20.9% mean weight loss at 15 mg at 72 weeks. Up to 36% achieved 25% or more weight loss. Largest FDA-approved weight loss of any medication.
Advantage: Amycretin
Development Stage and Evidence#
Amycretin: Phase 1b/2a completed (125 patients, 36 weeks, Lancet). Phase 2 in T2D completed (448 patients). Phase 3 entering for obesity and T2D. Earliest approval years away.
Tirzepatide: FDA-approved 2022. SURPASS (5 T2D trials, 9,000+ patients) and SURMOUNT (obesity trials). Head-to-head superiority over semaglutide (SURPASS-2). Growing real-world safety experience.
Advantage: Tirzepatide
Formulation Options#
Amycretin: Both subcutaneous weekly and oral daily formulations in development. Oral formulation does not require fasting restrictions. Both showed efficacy in Phase 2 T2D trial.
Tirzepatide: Once-weekly subcutaneous injection only. No oral formulation available or in advanced development. Six dose strengths (2.5-15 mg) with hidden-needle pens.
Advantage: Amycretin
Safety Profile#
Amycretin: GI adverse events most common, consistent with GLP-1/amylin class. High frequency of GI events in early trials. Limited to <600 total participants. No long-term or cardiovascular data.
Tirzepatide: Well-characterized GI profile (nausea 12-33%, diarrhea 12-21%). FDA-approved with growing post-marketing experience. CVOT underway. Lower GI rates than semaglutide at equivalent efficacy.
Advantage: Tirzepatide
Summary and Verdict#
Amycretin's early-phase data (24.3% weight loss at 36 weeks, no plateau) suggest it could substantially exceed tirzepatide's 20.9%, potentially becoming the most effective anti-obesity agent ever tested. However, this comparison is fundamentally unequal: amycretin's results come from 125 patients over 36 weeks, while tirzepatide's come from thousands of patients over 72 weeks in rigorous Phase 3 trials. Early-phase weight loss often diminishes in larger trials. Tirzepatide is FDA-approved and available today. Amycretin's promise must be confirmed in Phase 3 before definitive conclusions can be drawn.
Best For Recommendations#
Treatment Available Now#
Recommendation: Tirzepatide
Reason: Tirzepatide is FDA-approved and available as Mounjaro/Zepbound. Amycretin is years from potential approval. For patients who need treatment today, tirzepatide is the only option.
Maximum Weight Loss (Proven)#
Recommendation: Tirzepatide
Reason: With 20.9% weight loss at 15 mg in SURMOUNT-1, tirzepatide is the most effective approved anti-obesity medication, supported by thousands of patients across multiple Phase 3 trials.
Maximum Weight Loss Potential (Future)#
Recommendation: Amycretin
Reason: If Phase 3 confirms the 24.3% weight loss seen in Phase 1b/2a (with no plateau at 36 weeks), amycretin could become the most effective obesity treatment ever developed.
Oral Treatment Option (Future)#
Recommendation: Amycretin
Reason: Amycretin has an oral formulation in development without fasting restrictions. Tirzepatide has no oral formulation, making amycretin the only dual-agonist option with oral potential.
Type 2 Diabetes#
Recommendation: Tirzepatide
Reason: Five SURPASS trials with 9,000+ patients, FDA approval, and demonstrated superiority over semaglutide. Amycretin's T2D data is limited to Phase 2.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Treatment Available Now
Tirzepatide
Tirzepatide is FDA-approved and available as Mounjaro/Zepbound. Amycretin is years from potential approval. For patients who need treatment today, tirzepatide is the only option.
Maximum Weight Loss (Proven)
Tirzepatide
With 20.9% weight loss at 15 mg in SURMOUNT-1, tirzepatide is the most effective approved anti-obesity medication, supported by thousands of patients across multiple Phase 3 trials.
Maximum Weight Loss Potential (Future)
Amycretin
If Phase 3 confirms the 24.3% weight loss seen in Phase 1b/2a (with no plateau at 36 weeks), amycretin could become the most effective obesity treatment ever developed.
Oral Treatment Option (Future)
Amycretin
Amycretin has an oral formulation in development without fasting restrictions. Tirzepatide has no oral formulation, making amycretin the only dual-agonist option with oral potential.
Type 2 Diabetes
Tirzepatide
Five SURPASS trials with 9,000+ patients, FDA approval, and demonstrated superiority over semaglutide. Amycretin's T2D data is limited to Phase 2.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Amycretin vs Tirzepatide: Emerging GLP-1/Amylin vs Approved GIP/GLP-1
Which is better, Amycretin or Tirzepatide?
Amycretin's early-phase data (24.3% weight loss at 36 weeks, no plateau) suggest it could substantially exceed tirzepatide's 20.9%, potentially becoming the most effective anti-obesity agent ever tested. However, this comparison is fundamentally unequal: amycretin's results come from 125 patients over 36 weeks, while tirzepatide's come from thousands of patients over 72 weeks in rigorous Phase 3 trials. Early-phase weight loss often diminishes in larger trials. Tirzepatide is FDA-approved and... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Amycretin and Tirzepatide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Weight Loss Efficacy: advantage goes to Amycretin; Development Stage and Evidence: advantage goes to Tirzepatide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Tirzepatide over Amycretin?
For the scenario of "Treatment Available Now," research data suggests Tirzepatide may be more relevant. Tirzepatide is FDA-approved and available as Mounjaro/Zepbound. Amycretin is years from potential approval. For patients who need treatment today, tirzepatide is the only option.. This is based on currently available evidence and individual circumstances may differ.
How do Amycretin and Tirzepatide differ in their mechanisms of action?
Amycretin: Unimolecular dual GLP-1 and amylin receptor agonist. Single molecule combining two satiety pathways. Amylin component provides brainstem appetite suppression and leptin resensitization.. Tirzepatide: Dual GIP and GLP-1 receptor agonist. Single 39-amino acid molecule with ~5-fold potency at GIPR relative to native GIP. Synergistic incretin activation for insulin secretion and appetite suppression..
Which has fewer side effects, Amycretin or Tirzepatide?
In terms of side effects and tolerability, the advantage goes to Tirzepatide. Amycretin: GI adverse events most common, consistent with GLP-1/amylin class. High frequency of GI events in early trials. Limited to <600 total participants..... Tirzepatide: Well-characterized GI profile (nausea 12-33%, diarrhea 12-21%). FDA-approved with growing post-marketing experience. CVOT underway. Lower GI rates ....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.