CT-388 vs Retatrutide: Dual Agonist vs Triple Agonist for Weight Loss
Comparison of CT-388 (signaling-biased dual GLP-1/GIP agonist by Roche) and retatrutide (triple GLP-1/GIP/glucagon agonist by Eli Lilly), two next-generation weight loss peptides in clinical development.
Verdict at a Glance
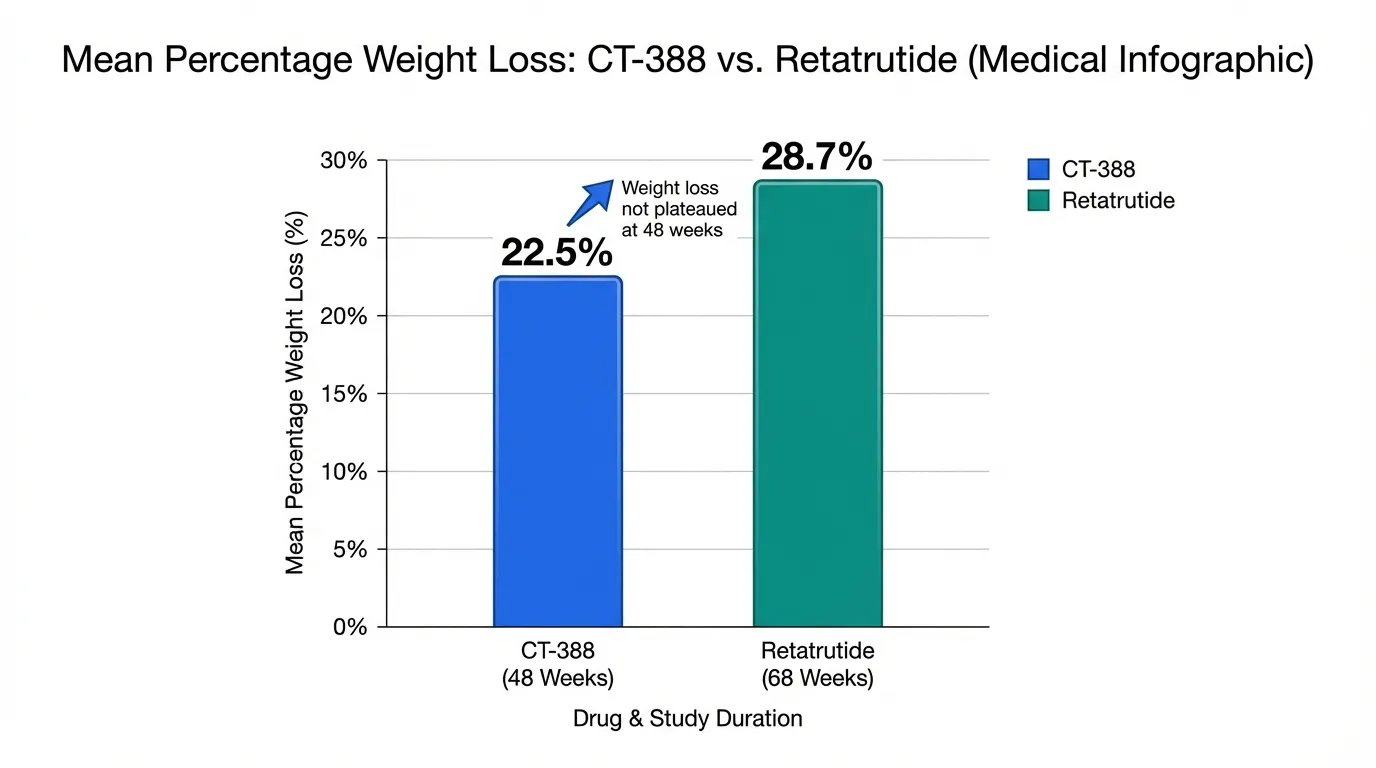
Retatrutide holds a clear advantage in both efficacy and development timeline. Its triple-receptor mechanism produced 28.7% weight loss in Phase 3 -- substantially greater than CT-388's 22.5% in Phase 2 -- and it is approximately 2-3 years ahead in the regulatory pathway. However, this superior efficacy comes at a cost: higher GI side effect rates and a novel dysesthesia safety signal. CT-388's signaling-biased approach offers a potentially better-tolerated dual agonist with impressive Phase 2 results and no plateau at 48 weeks. For patients who cannot tolerate triple agonist side effects, CT-388 may eventually represent a compelling alternative. Both remain investigational and are not available outside clinical trials.
| Best for | Pick | Why |
|---|---|---|
| Maximum Weight Loss Potential | Retatrutide | Retatrutide's 28.7% weight loss at 68 weeks is the highest reported in any obesity clinical trial. The triple-receptor mechanism (adding glucagon for energy expenditure) appears to produce fundamentally greater weight reduction than dual agonism. |
| Better Tolerability Profile | CT-388 | CT-388's signaling-biased design produced lower discontinuation rates (5.9% vs 12-18% for retatrutide) and no novel safety signals. For patients sensitive to GI side effects, the biased agonist approach may offer meaningful advantages. |
| Closer to Market Availability | Retatrutide | Retatrutide has completed Phase 3 and could receive FDA approval as early as 2027. CT-388 is just entering Phase 3 in 2026, placing potential approval in 2028-2029 at the earliest. |
| Metabolic Liver Benefits | Retatrutide | The glucagon receptor component of retatrutide directly promotes hepatic fat oxidation. This mechanism is being studied for MASLD/NASH in the TRIUMPH program. CT-388 lacks glucagon receptor activity. |
| Novel Pharmacological Approach | CT-388 | CT-388's signaling bias -- minimizing beta-arrestin recruitment to sustain receptor activity -- is a pharmacological innovation not found in retatrutide or any other approved obesity drug. The ongoing weight loss at 48 weeks may reflect sustained receptor signaling. |
| Category | CT-388 | Retatrutide | Advantage |
|---|---|---|---|
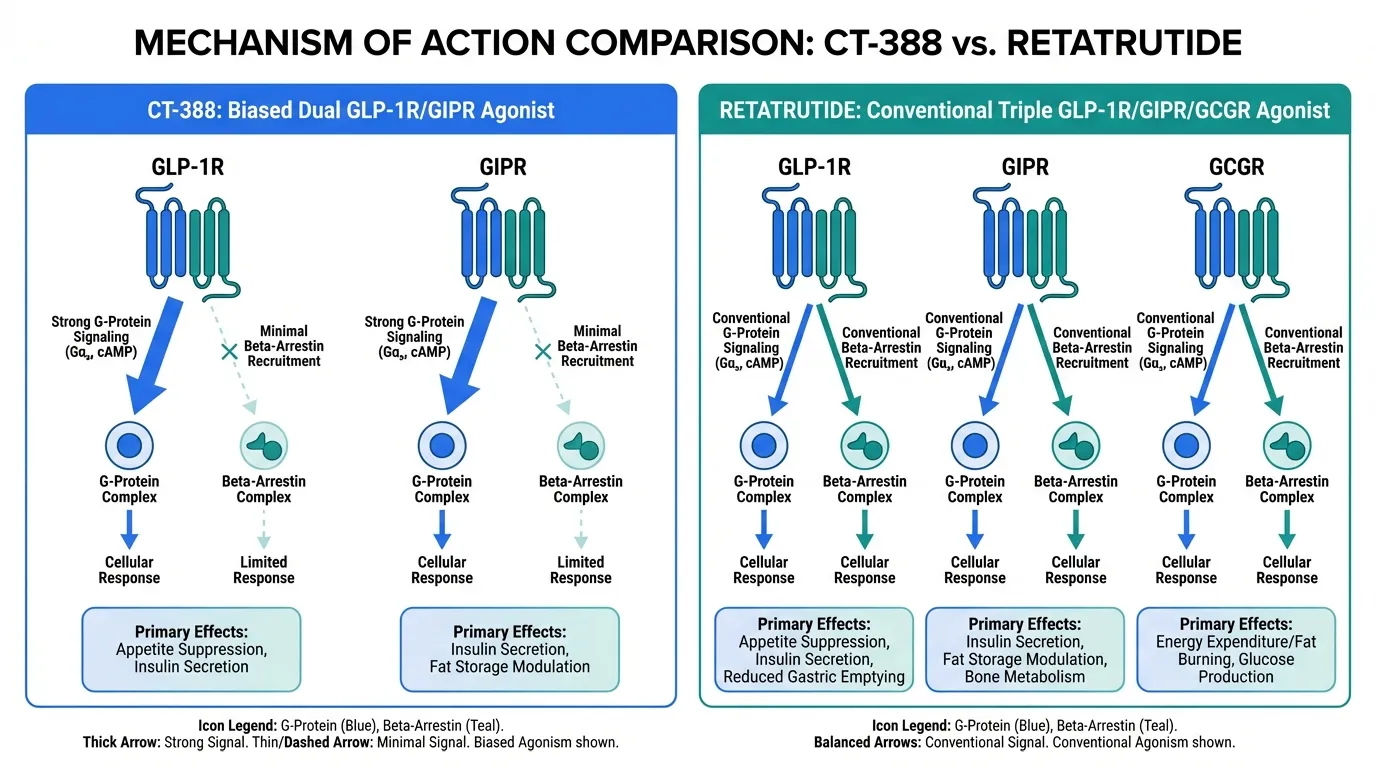
| Mechanism of Action | Signaling-biased dual GLP-1/GIP receptor agonist (Roche/Carmot). Engineered to minimize beta-arrestin recruitment, reducing receptor internalization and desensitization. Activates two incretin receptors with sustained pharmacological activity through biased G-protein signaling. | First-in-class triple GLP-1/GIP/glucagon receptor agonist (Eli Lilly). Activates three metabolic receptors simultaneously. The glucagon component adds increased energy expenditure and hepatic fat oxidation beyond what dual GLP-1/GIP agonism achieves. Conventional (unbiased) signaling. | Retatrutide |
| Weight Loss Efficacy | Phase 2 showed 22.5% placebo-adjusted weight loss at 48 weeks (24 mg dose). 87% of participants achieved at least 10% loss, 26.1% achieved at least 30%. Weight loss trajectory had not plateaued at study end, suggesting greater losses with longer treatment. | Phase 3 TRIUMPH-4 showed 28.7% mean weight loss at 68 weeks (12 mg dose) and 26.4% at 9 mg. These are the highest weight reductions reported in any obesity clinical trial. Phase 2 had shown up to 24.2% at 48 weeks. | Retatrutide |
| Research Evidence | Phase 1b and Phase 2 completed. Phase 2 enrolled a limited number of participants. Phase 3 trials (Enith1 and Enith2) announced January 2026. No head-to-head comparisons. No cardiovascular outcomes or long-term safety data. | Phase 2 completed (N=338) and published in NEJM 2023. TRIUMPH-4 Phase 3 completed (N=445). Seven additional Phase 3 trials expected to complete in 2026. No head-to-head comparisons with other agents yet. No CV outcomes data yet. | Retatrutide |
| Side Effect Profile | GI adverse events mild to moderate, consistent with incretin class. Treatment discontinuation due to adverse events was 5.9% vs 1.3% placebo. Signaling-biased design may theoretically reduce GI side effects by preventing receptor desensitization. No novel safety signals reported. | Higher GI adverse event rates than dual agonists. Nausea 38-43%, diarrhea 33-35%, vomiting 20-21%. Discontinuation 12-18% at therapeutic doses. Novel dysesthesia signal in Phase 3 (8.8-20.9% vs 0.7% placebo), though generally mild. Higher tolerability burden. | CT-388 |
| Development Status | Phase 3 trials (Enith1, Enith2) announced January 2026 by Roche. Earliest potential FDA approval likely 2028-2029 based on typical timelines. Roche also developing oral CT-996 as a complementary GLP-1 program. | TRIUMPH-4 Phase 3 completed December 2025. Seven additional Phase 3 trials expected to complete in 2026. Eli Lilly expected to submit NDA in 2026 with potential FDA approval in 2027. Significantly ahead of CT-388 in the regulatory timeline. | Retatrutide |

Introduction#
CT-388 and Retatrutide represent two distinct strategies for advancing beyond the current generation of weight loss medications. Both are investigational, and both aim to surpass the efficacy of FDA-approved agents like tirzepatide and semaglutide. But they take fundamentally different approaches.
CT-388 (Roche/Carmot Therapeutics) is a dual GLP-1/GIP receptor agonist with a key innovation: signaling bias. By engineering the molecule to minimize beta-arrestin recruitment, CT-388 aims to reduce receptor desensitization and maintain stronger pharmacological activity over time. It targets the same two receptors as tirzepatide but with a more refined signaling profile.
Retatrutide (Eli Lilly) takes a different path: adding a third receptor. As a triple GLP-1/GIP/glucagon agonist, retatrutide combines the appetite-suppressing effects of GLP-1 and GIP with glucagon's ability to increase energy expenditure and promote fat burning. The result is the highest weight loss ever reported in a clinical trial.
This comparison examines how these two approaches stack up across mechanism, efficacy, safety, evidence, and development timeline.
Mechanism of Action Comparison#
CT-388#
CT-388 is a once-weekly subcutaneous dual GLP-1/GIP receptor agonist developed by Carmot Therapeutics (acquired by Roche for $2.7 billion in 2023). Its defining feature is signaling bias -- a deliberate design choice that distinguishes it from other dual agonists.
Most G-protein coupled receptor (GPCR) agonists activate two downstream pathways: G-protein signaling (which mediates the desired metabolic effects) and beta-arrestin recruitment (which causes the receptor to be pulled inside the cell and desensitized). CT-388 was engineered to strongly activate G-protein signaling while minimizing beta-arrestin recruitment at both GLP-1 and GIP receptors.
The practical implication: receptors remain active on the cell surface longer, potentially maintaining stronger and more consistent metabolic effects between weekly doses. Preclinical data showed that biased agonism produced greater weight loss than unbiased agonism in animal models.
Retatrutide#
Retatrutide (LY3437943) is a 39-amino acid peptide that activates GLP-1, GIP, and glucagon receptors simultaneously. Each receptor contributes distinct metabolic effects:
- GLP-1 receptor: Appetite suppression, satiety signaling, slowed gastric emptying
- GIP receptor: Enhanced insulin secretion, potentially improved fat metabolism and appetite modulation
- Glucagon receptor: Increased energy expenditure, hepatic fat oxidation, thermogenesis
The glucagon component is what sets retatrutide apart from all dual agonists. While GLP-1 and GIP primarily reduce energy intake (how much you eat), glucagon increases energy output (how many calories you burn). This dual approach -- eating less and burning more -- is the leading hypothesis for why retatrutide produces substantially greater weight loss than dual agonists.
Mechanistic Comparison#
| Feature | CT-388 | Retatrutide |
|---|---|---|
| Receptor targets | GLP-1R + GIPR | GLP-1R + GIPR + GCGR |
| Number of receptors | 2 | 3 |
| Signaling bias | G-protein biased | Conventional (unbiased) |
| Energy intake reduction | Yes (GLP-1 + GIP) | Yes (GLP-1 + GIP) |
| Energy expenditure increase | No | Yes (glucagon) |
| Hepatic fat oxidation | No direct mechanism | Yes (glucagon) |
| Developer | Roche/Carmot | Eli Lilly |
Weight Loss Efficacy Comparison#
CT-388 Efficacy Data#
CT-388's Phase 2 trial results were announced by Roche in January 2026:
- 48-week placebo-adjusted weight loss (efficacy estimand): 22.5% at the 24 mg dose
- Treatment-regimen estimand: 18.3% placebo-adjusted
- Responder rates (24 mg): 95.7% achieved at least 5% loss, 87% at least 10%, 47.8% at least 20%, 26.1% at least 30%
- Obesity resolution: 54% of the 24 mg group achieved BMI below 30 vs 13% with placebo
- Weight loss trajectory: Had not plateaued at 48 weeks
The absence of a plateau is clinically significant. It suggests that with longer treatment duration, CT-388 could produce even greater weight loss than the 22.5% observed at 48 weeks.
Retatrutide Efficacy Data#
Retatrutide has both Phase 2 and Phase 3 data:
Phase 2 (NEJM 2023): In 338 adults with obesity, weight loss at 48 weeks ranged from 8.7% (1 mg) to 24.2% (12 mg) compared to 2.1% with placebo.
Phase 3 TRIUMPH-4 (December 2025): In 445 adults with obesity and knee osteoarthritis:
- 12 mg dose: 28.7% mean weight loss at 68 weeks
- 9 mg dose: 26.4% mean weight loss at 68 weeks
- Placebo: 2.1% weight loss
The 28.7% result is the largest mean weight loss ever reported in a completed Phase 3 obesity trial.
Efficacy Comparison Table#
| Metric | CT-388 | Retatrutide |
|---|---|---|
| Study phase | Phase 2 | Phase 3 |
| Duration | 48 weeks | 68 weeks |
| Best dose result | 22.5% (24 mg) | 28.7% (12 mg) |
| Participants achieving 10%+ loss | 87% | Not yet reported |
| Participants achieving 20%+ loss | 47.8% | Not yet reported |
| Participants achieving 30%+ loss | 26.1% | Not yet reported |
| Weight loss plateau | Not reached | Not reported |
Important caveats: These trials cannot be directly compared. They used different study designs, patient populations, durations, and dose titration schemes. CT-388's 22.5% at 48 weeks without a plateau could potentially approach retatrutide's results with longer treatment, but this is speculative. Retatrutide's Phase 3 data is inherently more reliable due to larger sample size and longer duration.
Side Effect Profile Comparison#
CT-388 Safety#
CT-388's safety profile from Phase 2:
- GI adverse events were predominantly mild to moderate
- Consistent with the incretin drug class (nausea, diarrhea, constipation)
- Treatment discontinuation due to adverse events: 5.9% (CT-388) vs 1.3% (placebo)
- No novel safety signals were reported
- The signaling-biased mechanism may theoretically improve tolerability by reducing receptor desensitization
Retatrutide Safety#
Retatrutide's Phase 3 safety data from TRIUMPH-4:
- Nausea: 38-43%
- Diarrhea: 33-35%
- Constipation: 21-25%
- Vomiting: 20-21%
- Treatment discontinuation due to adverse events: 12.2% (9 mg) and 18.2% (12 mg) vs 4.0% (placebo)
- Dysesthesia (new signal): 8.8% at 9 mg and 20.9% at 12 mg vs 0.7% with placebo. This abnormal touch sensation was not observed in Phase 2 and represents a novel safety signal requiring monitoring in ongoing trials. Events were generally mild and rarely led to discontinuation.
Safety Comparison Table#
| Parameter | CT-388 | Retatrutide |
|---|---|---|
| GI adverse events | Mild-moderate, class-consistent | Higher rates than dual agonists |
| Discontinuation rate | 5.9% | 12.2-18.2% |
| Novel safety signals | None reported | Dysesthesia (8.8-20.9%) |
| Long-term safety data | Not available | Limited (Phase 3) |
| Post-marketing data | None | None |
The tolerability difference is notable. CT-388's lower discontinuation rate (5.9% vs 12-18%) may reflect either its signaling-biased mechanism, the inherently lower side effect burden of dual vs triple agonism, or differences in study populations and dose titration. Regardless of the cause, fewer patients stopping treatment translates to more patients benefiting from the drug in practice.
Research Evidence Comparison#
CT-388#
- Phase 1b: Multi-cohort trial showing 18.8% placebo-adjusted weight loss. Strong responder rates.
- Phase 2: 22.5% at 48 weeks, results announced January 2026. Limited sample size.
- Phase 3: Enith1 and Enith2 announced, expected to start Q1 2026.
- Published peer-reviewed data: Phase 1b data published in 2025.
- Head-to-head data: None.
- CV outcomes: None.
Evidence level: Low-moderate. Promising early data with impressive responder rates, but small sample sizes and no confirmatory Phase 3 results.
Retatrutide#
- Phase 2: 338 patients, published in NEJM 2023 (PMID: 37366315). Dose-ranging from 1-12 mg.
- Phase 3 TRIUMPH-4: 445 patients, completed December 2025. Top-line results disclosed.
- Phase 3 program: Seven additional TRIUMPH trials expected to complete in 2026.
- Liver disease: Phase 2a trial in MASLD/NASH published in Nature Medicine 2024.
- Head-to-head data: None vs other agents.
- CV outcomes: Not yet available.
Evidence level: Moderate-high. Phase 2 data published in a top-tier journal, first Phase 3 trial completed with strong results, extensive program underway. Substantially more data than CT-388.
Development Timeline#
| Milestone | CT-388 | Retatrutide |
|---|---|---|
| Phase 2 completion | January 2026 | 2023 |
| Phase 3 start | Q1 2026 | 2023 |
| First Phase 3 results | ~2028 (estimated) | December 2025 |
| Full Phase 3 program | ~2028-2029 | Expected 2026 |
| Potential NDA submission | ~2029 | 2026 (estimated) |
| Potential FDA approval | ~2029-2030 | 2027 (estimated) |
Retatrutide holds a 2-3 year lead in the development timeline. If approved, it would reach patients years before CT-388 could.
Key Differences Summary#
- Receptor count: CT-388 targets two receptors (GLP-1 + GIP); retatrutide targets three (GLP-1 + GIP + glucagon). The glucagon component is retatrutide's key differentiator.
- Signaling approach: CT-388's beta-arrestin minimization is a pharmacological innovation that may sustain receptor activity and improve tolerability. Retatrutide uses conventional agonism.
- Weight loss: Retatrutide's 28.7% at 68 weeks exceeds CT-388's 22.5% at 48 weeks, though CT-388 had not plateaued and may narrow this gap with longer treatment.
- Tolerability: CT-388 shows markedly lower discontinuation rates and no novel safety signals. Retatrutide has higher GI rates and a new dysesthesia signal.
- Energy expenditure: Only retatrutide increases energy expenditure via glucagon receptor activation. CT-388, like all pure GLP-1/GIP agonists, primarily reduces energy intake.
- Timeline: Retatrutide is approximately 2-3 years ahead of CT-388 in development and could reach the market by 2027.
- Company strategy: Roche pairs CT-388 (injectable) with CT-996 (oral GLP-1) for a two-pronged obesity strategy. Eli Lilly pairs retatrutide with tirzepatide (approved) and orforglipron (oral GLP-1 in development).
Conclusion#
This comparison highlights two philosophically different approaches to next-generation obesity treatment. Retatrutide asks: what if we activate more metabolic pathways? CT-388 asks: what if we activate existing pathways more effectively?
Retatrutide currently leads on both efficacy and development timeline. Its triple-receptor mechanism produces the highest weight loss ever seen in clinical trials, and with Phase 3 data already in hand, it is years ahead of CT-388 in the path to market. For patients and clinicians focused on maximum weight reduction and the earliest access to a next-generation agent, retatrutide is the more relevant drug to watch.
CT-388 offers a different value proposition. Its signaling-biased design -- minimizing receptor desensitization through reduced beta-arrestin recruitment -- is a genuine pharmacological innovation. The lower discontinuation rates and the absence of a weight loss plateau at 48 weeks suggest that this approach may yield a drug that is both effective and well-tolerated. For patients who cannot tolerate triple agonist side effects, or who experience diminishing returns from conventional agonists over time, CT-388 could fill an important gap.
Both remain investigational. Neither should be considered an available treatment. The definitive comparison will require CT-388's Phase 3 results and ideally a head-to-head trial, neither of which exists today.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Maximum Weight Loss Potential
Retatrutide
Retatrutide's 28.7% weight loss at 68 weeks is the highest reported in any obesity clinical trial. The triple-receptor mechanism (adding glucagon for energy expenditure) appears to produce fundamentally greater weight reduction than dual agonism.
Better Tolerability Profile
CT-388
CT-388's signaling-biased design produced lower discontinuation rates (5.9% vs 12-18% for retatrutide) and no novel safety signals. For patients sensitive to GI side effects, the biased agonist approach may offer meaningful advantages.
Closer to Market Availability
Retatrutide
Retatrutide has completed Phase 3 and could receive FDA approval as early as 2027. CT-388 is just entering Phase 3 in 2026, placing potential approval in 2028-2029 at the earliest.
Metabolic Liver Benefits
Retatrutide
The glucagon receptor component of retatrutide directly promotes hepatic fat oxidation. This mechanism is being studied for MASLD/NASH in the TRIUMPH program. CT-388 lacks glucagon receptor activity.
Novel Pharmacological Approach
CT-388
CT-388's signaling bias -- minimizing beta-arrestin recruitment to sustain receptor activity -- is a pharmacological innovation not found in retatrutide or any other approved obesity drug. The ongoing weight loss at 48 weeks may reflect sustained receptor signaling.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About CT-388 vs Retatrutide: Dual Agonist vs Triple Agonist for Weight Loss
Which is better, CT-388 or Retatrutide?
Retatrutide holds a clear advantage in both efficacy and development timeline. Its triple-receptor mechanism produced 28.7% weight loss in Phase 3 -- substantially greater than CT-388's 22.5% in Phase 2 -- and it is approximately 2-3 years ahead in the regulatory pathway. However, this superior efficacy comes at a cost: higher GI side effect rates and a novel dysesthesia safety signal. CT-388's signaling-biased approach offers a potentially better-tolerated dual agonist with impressive Phase ... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between CT-388 and Retatrutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Retatrutide; Weight Loss Efficacy: advantage goes to Retatrutide; Research Evidence: advantage goes to Retatrutide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Retatrutide over CT-388?
For the scenario of "Maximum Weight Loss Potential," research data suggests Retatrutide may be more relevant. Retatrutide's 28.7% weight loss at 68 weeks is the highest reported in any obesity clinical trial. The triple-receptor mechanism (adding glucagon for energy expenditure) appears to produce fundamen.... This is based on currently available evidence and individual circumstances may differ.
How do CT-388 and Retatrutide differ in their mechanisms of action?
CT-388: Signaling-biased dual GLP-1/GIP receptor agonist (Roche/Carmot). Engineered to minimize beta-arrestin recruitment, reducing receptor internalization and desensitization. Activates two incretin rece.... Retatrutide: First-in-class triple GLP-1/GIP/glucagon receptor agonist (Eli Lilly). Activates three metabolic receptors simultaneously. The glucagon component adds increased energy expenditure and hepatic fat o....
Which has fewer side effects, CT-388 or Retatrutide?
In terms of side effects and tolerability, the advantage goes to CT-388. CT-388: GI adverse events mild to moderate, consistent with incretin class. Treatment discontinuation due to adverse events was 5.9% vs 1.3% placebo. Signa.... Retatrutide: Higher GI adverse event rates than dual agonists. Nausea 38-43%, diarrhea 33-35%, vomiting 20-21%. Discontinuation 12-18% at therapeutic doses. Nov....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.