MariTide vs Semaglutide: Monthly Antibody-Peptide Conjugate vs Weekly GLP-1
Evidence-based comparison of MariTide (maridebart cafraglutide), Amgen's once-monthly antibody-peptide conjugate, and semaglutide (Ozempic/Wegovy), the established GLP-1 standard of care for obesity and diabetes.
Verdict at a Glance
Semaglutide remains the proven standard with FDA approval, cardiovascular benefit, and the broadest evidence base of any GLP-1 agonist. MariTide offers a genuinely differentiated approach with three key innovations -- monthly dosing, an antibody-peptide conjugate platform, and GIP receptor antagonism (vs the GIP agonism used by tirzepatide). The phase 2 NEJM-published data showing up to 20% weight loss at 52 weeks with monthly injections and GI side effects concentrated at the first dose are particularly promising. If phase 3 confirms these results, MariTide could become the preferred option for patients who want the least frequent dosing schedule.
| Best for | Pick | Why |
|---|---|---|
| Available Treatment Now | Semaglutide | Semaglutide is FDA-approved and commercially available in injectable and oral formulations. MariTide is investigational and not available outside clinical trials. |
| Cardiovascular Risk Reduction | Semaglutide | The SELECT trial (n=17,604) demonstrated a 20% reduction in MACE in overweight/obese adults with CVD. MariTide has no cardiovascular outcomes data. |
| Minimal Injection Frequency (Future) | MariTide | MariTide's once-monthly dosing (12 injections per year) represents a major convenience advantage over semaglutide's weekly schedule (52 injections per year). This could significantly improve adherence. |
| Oral Medication Preference | Semaglutide | Rybelsus is the only approved oral GLP-1 agonist. MariTide is injectable-only with no oral formulation in development due to its antibody-peptide conjugate structure. |
| GI Tolerability (Future) | MariTide | Phase 2 data showed GI side effects were predominantly mild, transient, and concentrated at the first dose, suggesting potentially better long-term GI tolerability compared to weekly incretin injections. |
| Weight Loss with Muscle Preservation (Future) | MariTide | MariTide's GIPR antagonism may help preserve lean mass during weight loss (though this has not been definitively demonstrated). The activin pathway effects could theoretically promote muscle retention. |
| Category | MariTide | Semaglutide | Advantage |
|---|---|---|---|
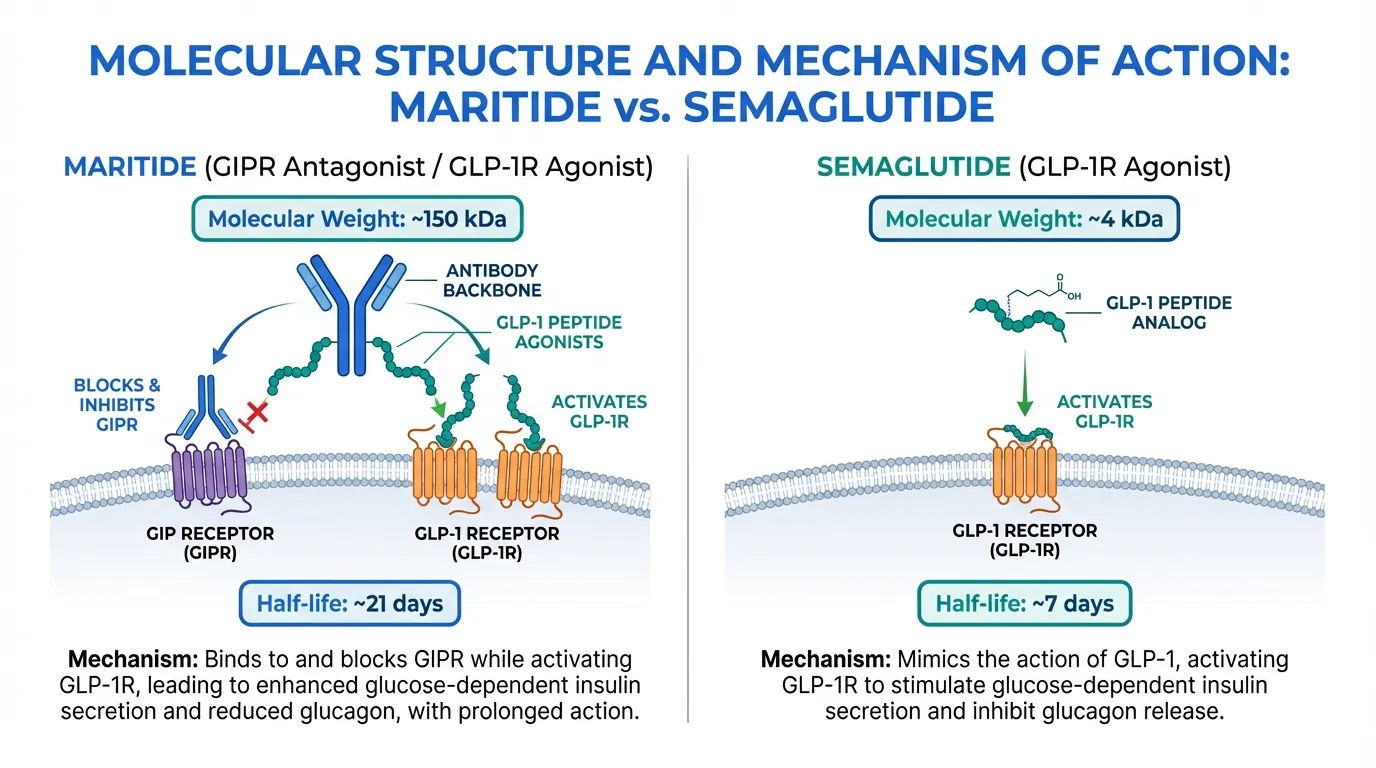
| Mechanism of Action | Novel antibody-peptide conjugate combining GLP-1 receptor agonism with GIP receptor antagonism. A fully human anti-GIPR monoclonal antibody conjugated to two GLP-1 analog peptides. Unique bispecific design with ~21-day half-life enabling monthly dosing. | Selective GLP-1 receptor agonist. Synthetic analog of human GLP-1 with Aib substitution and C18 fatty diacid for albumin binding. ~7-day half-life enabling weekly dosing. Single-target mechanism with well- understood pharmacology. | MariTide |
| Weight Loss Efficacy | Phase 2 showed up to 20% weight loss in the obesity-only cohort at 52 weeks (up to 16.2% mean from baseline vs 2.5% placebo), with weight loss not plateauing. Up to 17% in the obesity-with-T2D cohort. | STEP 1 demonstrated 14.9% mean weight loss at 68 weeks with 2.4 mg weekly. STEP 3 showed 16.0% with intensive lifestyle intervention. Proven across multiple large phase 3 trials. | MariTide |
| Research Evidence | Phase 2 trial published in NEJM (2025) with 592 participants across two cohorts (obesity, obesity+T2D) over 52 weeks. Phase 3 trials planned. No cardiovascular outcomes data. No head-to-head comparisons. | Extensive evidence across SUSTAIN, PIONEER, STEP, and SELECT programs with over 25,000 trial participants. Proven cardiovascular benefit in SELECT (20% MACE reduction). 7+ years of post-marketing surveillance. | Semaglutide |
| Side Effect Profile | GI adverse events were the most common, including nausea, vomiting, and constipation. Notably, nausea and vomiting were predominantly mild, transient, and primarily associated with the first dose only. | Well-characterized GI profile. Nausea 15-44%, vomiting 5-24%, diarrhea 8-30%. Higher rates at the 2.4 mg weight management dose. Most effects diminish with continued treatment. Extensive post-marketing safety data. | MariTide |
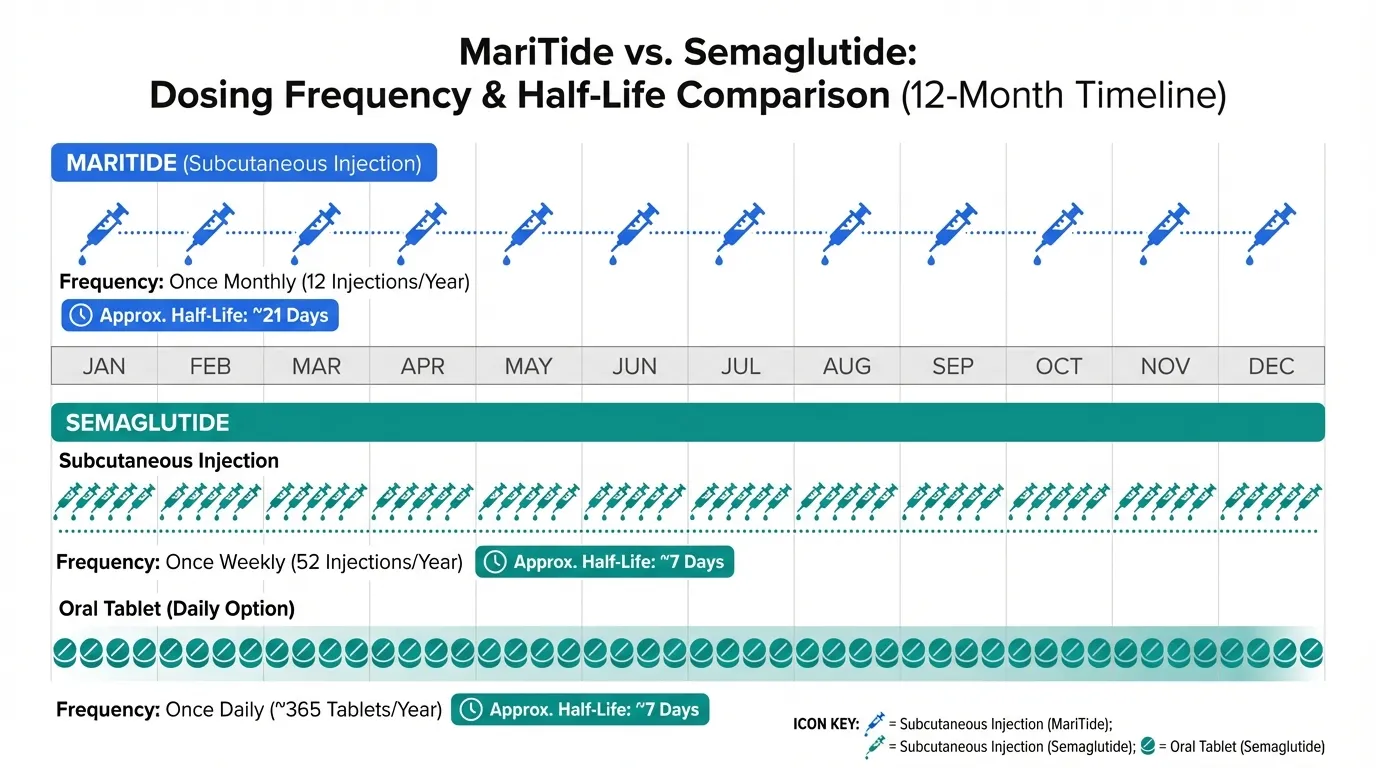
| Dosing Convenience | Once-monthly subcutaneous injection -- the longest dosing interval of any obesity medication in development. ~21-day half-life (three times longer than any approved GLP-1/GIP therapy). No oral formulation. | Once-weekly injection (Ozempic/Wegovy) or daily oral tablet (Rybelsus). Multiple formulations provide flexibility. Oral form requires empty stomach with minimal water. | MariTide |

Introduction#
MariTide (maridebart cafraglutide) and semaglutide represent fundamentally different approaches to incretin-based obesity therapy. Semaglutide is the most widely prescribed GLP-1 agonist, with an extensive evidence base spanning diabetes, obesity, and cardiovascular outcomes. MariTide, developed by Amgen, is a first-in-class antibody-peptide conjugate that combines GLP-1 receptor agonism with GIP receptor antagonism in a single molecule designed for once-monthly dosing.
This comparison is noteworthy not just for the efficacy data, but for the strategic divergence in mechanism: while tirzepatide and other dual agonists activate the GIP receptor alongside GLP-1R, MariTide takes the opposite approach by blocking GIPR while activating GLP-1R. Both strategies appear to enhance weight loss beyond GLP-1 agonism alone, raising fundamental questions about GIP receptor biology in obesity.
Mechanism of Action Comparison#
MariTide#
MariTide is a bispecific antibody-peptide conjugate (APC) consisting of a fully human monoclonal antibody that antagonizes the GIP receptor (GIPR), conjugated to two GLP-1 receptor agonist peptide molecules via amino acid linkers. This design enables three distinct pharmacological actions in a single molecule:
- GLP-1 receptor agonism: The two conjugated GLP-1 analog peptides activate GLP-1R to produce appetite suppression, glucose-dependent insulin secretion, glucagon suppression, and delayed gastric emptying
- GIP receptor antagonism: The antibody component blocks GIP signaling, which may reduce fat storage and modify energy metabolism
- Extended half-life: The antibody backbone provides a half-life of approximately 21 days -- three times longer than any approved weekly incretin therapy -- enabling once-monthly dosing
The GIP antagonism approach is the most distinctive feature. While tirzepatide enhances GIP signaling (agonism) to produce metabolic benefits, MariTide blocks GIP signaling (antagonism). The fact that both approaches appear to enhance weight loss beyond GLP-1 agonism alone suggests that modulating GIP activity in either direction may be beneficial, potentially through different downstream mechanisms.
Semaglutide#
Semaglutide is a selective GLP-1 receptor agonist -- a synthetic analog of human GLP-1(7-37) with an Aib substitution at position 8 for DPP-4 resistance and a C18 fatty diacid chain at lysine-26 for albumin binding. The half-life is approximately 7 days, enabling once-weekly injection.
GLP-1R activation produces glucose-dependent insulin secretion, glucagon suppression, delayed gastric emptying, and central appetite reduction through hypothalamic and brainstem signaling. The oral formulation (Rybelsus) uses a sodium N-(8-[2-hydroxybenzoyl] amino) caprylate (SNAC) absorption enhancer for oral bioavailability.
Mechanistic Comparison#
| Feature | MariTide | Semaglutide |
|---|---|---|
| Drug class | Antibody-peptide conjugate | Peptide GLP-1 agonist |
| GLP-1R effect | Agonism (via conjugated peptides) | Agonism |
| GIPR effect | Antagonism (via antibody) | None |
| Molecular weight | ~150 kDa (antibody + peptides) | ~4,114 Da |
| Half-life | ~21 days | ~7 days |
| Dosing frequency | Monthly | Weekly (injectable) or daily (oral) |
Dosing Comparison#
MariTide Dosing#
MariTide is administered as a once-monthly subcutaneous injection -- the longest dosing interval of any obesity medication in development. The phase 2 trial tested multiple dose levels over 52 weeks. The ~21-day half-life means patients require only 12 injections per year compared to 52 with weekly therapies.
Phase 3 dose selection has not been publicly announced.
Semaglutide Dosing#
- Wegovy (obesity): 0.25 mg weekly escalating over 16 weeks to the target dose of 2.4 mg
- Ozempic (T2D): 0.25 mg weekly escalating to 0.5, 1, or 2 mg
- Rybelsus (oral): 3 mg daily escalating to 7 or 14 mg
Dosing Comparison Table#
| Parameter | MariTide | Semaglutide |
|---|---|---|
| Injection frequency | Monthly (12/year) | Weekly (52/year) or daily oral |
| Route | Subcutaneous only | SC or oral |
| Half-life | ~21 days | ~7 days |
| Time to steady state | Longer (monthly kinetics) | ~4-5 weeks |
| Oral option | No (antibody structure) | Yes (Rybelsus) |
Side Effects Comparison#
MariTide Side Effects#
The phase 2 trial showed that the most common adverse events with MariTide were GI-related, including nausea, vomiting, and constipation. A distinctive finding was that nausea and vomiting were predominantly mild, transient, and primarily associated with the first dose. This pattern is potentially significant because it suggests that GI tolerability improves substantially after the initial injection, unlike weekly incretins where GI effects tend to recur with each dose escalation.
Improvements in cardiometabolic markers including waist circumference, blood pressure, hs-CRP, and lipid parameters were also observed.
Semaglutide Side Effects#
Semaglutide's GI profile is well characterized. Nausea 15-44%, vomiting 5-24%, diarrhea 8-30%, constipation 5-24%. Rates are higher at the 2.4 mg weight management dose. Most effects are mild to moderate and diminish with continued treatment but can recur during dose escalation. Additional known effects include cholelithiasis, modest heart rate increase of 2-4 bpm, and a boxed warning for thyroid C-cell tumors.
Safety Comparison Table#
| Parameter | MariTide | Semaglutide |
|---|---|---|
| GI events | Primarily first-dose, mild-transient | Recurring during escalation, 15-44% nausea |
| GI tolerability pattern | Improves substantially after first dose | Improves with continued use |
| Post-marketing data | None | 7+ years |
| CV outcomes data | None | SELECT (20% MACE reduction) |
| Cardiometabolic markers | Improvements observed in phase 2 | Well-documented improvements |
Research Evidence Comparison#
MariTide Research#
MariTide's key evidence comes from a phase 2 trial published in the New England Journal of Medicine (2025):
- Design: 592 participants across two cohorts -- obesity without T2D, and obesity with T2D -- over 52 weeks
- Obesity cohort: Mean weight loss ranged from -12.3% to -16.2% with MariTide vs -2.5% with placebo (up to 20% in some analyses)
- Obesity + T2D cohort: Mean weight loss ranged from -8.4% to -12.3% with MariTide vs -1.7% with placebo; HbA1c reductions up to 1.6 percentage points
- Weight trajectory: Weight loss had not plateaued by 52 weeks, indicating potential for further reduction with continued treatment
- Cardiometabolic: Improvements in waist circumference, blood pressure, hs-CRP, and lipid parameters
Evidence level: Moderate -- well-designed phase 2 with NEJM publication, but single trial, no head-to-head comparisons.
Semaglutide Research#
- SUSTAIN (T2D): Seven trials, >4,000 patients, HbA1c 1.2-2.2%
- PIONEER (oral T2D): Nine trials, >9,000 patients
- STEP (obesity): STEP 1 showed 14.9% at 68 weeks; STEP 5 confirmed 15.2% at 2 years
- SELECT (CV outcomes): 17,604 patients, 20% MACE reduction
Evidence level: Very high -- extensive multi-program evidence with cardiovascular outcomes.
Key Differences Summary#
- Drug platform: MariTide is a large antibody-peptide conjugate (~150 kDa). Semaglutide is a small peptide (~4 kDa). This structural difference enables MariTide's monthly dosing but prevents oral formulation.
- GIP receptor approach: MariTide blocks GIPR (antagonism). Semaglutide does not interact with GIPR. Tirzepatide activates GIPR (agonism). All three approaches produce weight loss, raising questions about GIP biology.
- Dosing frequency: MariTide monthly (12/year) vs semaglutide weekly (52/year). This is the most practical differentiator for patients.
- GI tolerability pattern: MariTide's GI side effects appear concentrated at the first dose, while semaglutide's recur with dose escalation. If confirmed in phase 3, this could meaningfully improve patient experience.
- Weight loss: MariTide showed up to 20% at 52 weeks (phase 2, no plateau). Semaglutide showed 14.9% at 68 weeks (phase 3, STEP 1). Different study phases limit direct comparison.
- CV outcomes: Semaglutide has proven benefit (SELECT). MariTide has none.
- Formulation flexibility: Semaglutide offers oral and injectable options. MariTide's antibody structure limits it to injectable delivery.
Conclusion#
MariTide and semaglutide represent two fundamentally different therapeutic modalities applied to the same disease. Semaglutide is the established standard of care with unmatched evidence breadth, proven cardiovascular benefit, and the flexibility of injectable and oral formulations. For any patient requiring treatment today, semaglutide remains the evidence-based choice.
MariTide's differentiation is compelling on multiple fronts. Once-monthly dosing could dramatically improve adherence -- a major barrier in chronic weight management. The GIP receptor antagonism represents a genuinely novel mechanism that has produced competitive weight loss results. The observation that GI side effects concentrate at the first dose (rather than recurring with each injection) could improve the patient experience if confirmed in larger trials.
The critical unanswered questions are whether MariTide's phase 2 results will replicate in phase 3, whether the GIP antagonism approach provides unique metabolic benefits (such as lean mass preservation) beyond weight loss, and whether the antibody-peptide conjugate format introduces any long-term immunogenicity concerns. Phase 3 trials will need to address all of these questions before MariTide can challenge semaglutide's market position.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Available Treatment Now
Semaglutide
Semaglutide is FDA-approved and commercially available in injectable and oral formulations. MariTide is investigational and not available outside clinical trials.
Cardiovascular Risk Reduction
Semaglutide
The SELECT trial (n=17,604) demonstrated a 20% reduction in MACE in overweight/obese adults with CVD. MariTide has no cardiovascular outcomes data.
Minimal Injection Frequency (Future)
MariTide
MariTide's once-monthly dosing (12 injections per year) represents a major convenience advantage over semaglutide's weekly schedule (52 injections per year). This could significantly improve adherence.
Oral Medication Preference
Semaglutide
Rybelsus is the only approved oral GLP-1 agonist. MariTide is injectable-only with no oral formulation in development due to its antibody-peptide conjugate structure.
GI Tolerability (Future)
MariTide
Phase 2 data showed GI side effects were predominantly mild, transient, and concentrated at the first dose, suggesting potentially better long-term GI tolerability compared to weekly incretin injections.
Weight Loss with Muscle Preservation (Future)
MariTide
MariTide's GIPR antagonism may help preserve lean mass during weight loss (though this has not been definitively demonstrated). The activin pathway effects could theoretically promote muscle retention.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About MariTide vs Semaglutide: Monthly Antibody-Peptide Conjugate vs Weekly GLP-1
Which is better, MariTide or Semaglutide?
Semaglutide remains the proven standard with FDA approval, cardiovascular benefit, and the broadest evidence base of any GLP-1 agonist. MariTide offers a genuinely differentiated approach with three key innovations -- monthly dosing, an antibody-peptide conjugate platform, and GIP receptor antagonism (vs the GIP agonism used by tirzepatide). The phase 2 NEJM-published data showing up to 20% weight loss at 52 weeks with monthly injections and GI side effects concentrated at the first dose are ... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between MariTide and Semaglutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to MariTide; Weight Loss Efficacy: advantage goes to MariTide; Research Evidence: advantage goes to Semaglutide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Semaglutide over MariTide?
For the scenario of "Available Treatment Now," research data suggests Semaglutide may be more relevant. Semaglutide is FDA-approved and commercially available in injectable and oral formulations. MariTide is investigational and not available outside clinical trials.. This is based on currently available evidence and individual circumstances may differ.
How do MariTide and Semaglutide differ in their mechanisms of action?
MariTide: Novel antibody-peptide conjugate combining GLP-1 receptor agonism with GIP receptor antagonism. A fully human anti-GIPR monoclonal antibody conjugated to two GLP-1 analog peptides. Unique bispecifi.... Semaglutide: Selective GLP-1 receptor agonist. Synthetic analog of human GLP-1 with Aib substitution and C18 fatty diacid for albumin binding. ~7-day half-life enabling weekly dosing. Single-target mechanism wi....
Which has fewer side effects, MariTide or Semaglutide?
In terms of side effects and tolerability, the advantage goes to MariTide. MariTide: GI adverse events were the most common, including nausea, vomiting, and constipation. Notably, nausea and vomiting were predominantly mild, transie.... Semaglutide: Well-characterized GI profile. Nausea 15-44%, vomiting 5-24%, diarrhea 8-30%. Higher rates at the 2.4 mg weight management dose. Most effects dimin....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.