Liraglutide vs Tirzepatide: Daily Single Agonist vs Weekly Dual Agonist
Evidence-based comparison of liraglutide (Saxenda/Victoza) and tirzepatide (Mounjaro/Zepbound), covering single vs dual receptor agonism, SCALE vs SURMOUNT trials, daily vs weekly dosing, and cardiovascular evidence.
Verdict at a Glance
Tirzepatide is substantially superior to liraglutide in weight loss efficacy (20.9% vs 8.0%), glycemic control (HbA1c -2.58% vs -1.5%), and dosing convenience (weekly vs daily injection). The dual GIP/GLP-1 mechanism provides complementary metabolic benefits that a single GLP-1 agonist cannot match. Liraglutide's main advantage is its completed cardiovascular outcomes trial (LEADER) demonstrating 13% MACE reduction, while tirzepatide's CVOT is still pending. For patients where cardiovascular risk reduction is the primary goal and a proven CVOT is required, liraglutide (or semaglutide) may be preferred. For maximum weight loss or glycemic control, tirzepatide is the clear choice.
| Best for | Pick | Why |
|---|---|---|
| Maximum weight loss | Tirzepatide | SURMOUNT-1 showed 20.9% mean weight loss at 15 mg, approximately 3-fold greater than liraglutide SCALE results (8.0%) |
| Type 2 diabetes glycemic control | Tirzepatide | SURPASS trials demonstrated up to 2.58% HbA1c reduction, superior to all tested comparators including semaglutide |
| Proven cardiovascular risk reduction | Liraglutide | LEADER trial provides completed evidence of 13% MACE reduction; tirzepatide CVOT is still ongoing |
| Weekly dosing preference | Tirzepatide | Once-weekly injection (52 per year) vs once-daily liraglutide (365 per year), a 7-fold reduction in injection burden |
| Adolescent obesity or cost-sensitive settings | Liraglutide | Saxenda approved for ages 12+; biosimilar and generic competition may offer lower cost access to GLP-1 therapy |
| Category | Liraglutide | Tirzepatide | Advantage |
|---|---|---|---|
| Mechanism of Action | Selective GLP-1 receptor agonist only. C16 fatty acid chain extends half-life to 13 hours for once-daily injection. 97% homology to human GLP-1. First-generation acylated GLP-1 analog. Single-pathway appetite suppression and glucose homeostasis. | First-in-class dual GIP and GLP-1 receptor agonist. C20 fatty diacid extends half-life to approximately 5 days for once-weekly injection. GIP receptor agonism provides complementary metabolic effects including enhanced insulin sensitivity and adipose tissue signaling. | Tirzepatide |
| Weight Loss Efficacy | SCALE trial showed 8.0% mean weight loss at 3.0 mg over 56 weeks. In STEP 8, liraglutide achieved only 6.4% at 68 weeks. 33.1% achieved 10% or more loss in SCALE. First-generation obesity drug efficacy. | SURMOUNT-1 demonstrated up to 20.9% mean weight loss at 15 mg over 72 weeks. 63.2% achieved 20% or more loss at highest dose. Approximately 3-fold greater weight loss than liraglutide. Among the most effective obesity treatments available. | Tirzepatide |
| Glycemic Control | LEAD trials showed HbA1c reduction of 1.0-1.5% at 1.2-1.8 mg for T2D. Victoza approved at max 1.8 mg daily. Effective but modest glycemic improvements compared to newer agents. | SURPASS trials demonstrated HbA1c reduction of up to 2.58% at 15 mg. Superior to all comparators tested, including semaglutide 1.0 mg (SURPASS-2). Dual incretin pathway provides potent glucose lowering. | Tirzepatide |
| Dosing Convenience | Once-daily subcutaneous injection. 4-5 week titration from 0.6 mg to 3.0 mg for weight loss. 365 injections per year. Pen device with disposable needles. No oral option for weight management. | Once-weekly subcutaneous injection. Monthly dose escalation from 2.5 mg to 15 mg over 16-20 weeks. 52 injections per year (7-fold fewer than daily). Pre-filled single-dose pen. | Tirzepatide |
| Cardiovascular Evidence | LEADER trial (9,340 patients) demonstrated 13% MACE reduction in T2D with high CV risk (HR 0.87, p=0.01). 22% reduction in CV death. First GLP-1 agonist with proven CV benefit. Well-established evidence base. | SURPASS-CVOT ongoing for T2D cardiovascular outcomes. No completed dedicated CVOT yet. Preliminary signals suggest CV benefit from metabolic improvements. FDA approved based on glycemic/weight data without dedicated CVOT requirement for obesity indication. | Liraglutide |

Introduction#
Liraglutide and tirzepatide represent different generations and fundamentally different pharmacological approaches to incretin-based obesity and diabetes treatment. Liraglutide (Victoza/Saxenda) is a selective GLP-1 receptor agonist requiring daily injection, while tirzepatide (Mounjaro/Zepbound) is a first-in-class dual GIP/GLP-1 receptor agonist with weekly dosing. Tirzepatide's dual mechanism has produced substantially greater clinical outcomes, establishing it as one of the most effective pharmaceutical obesity treatments available.
This comparison examines the mechanistic, clinical, and practical differences between these agents, drawing on the SCALE, LEAD, SURMOUNT, and SURPASS trial programs.
Mechanism of Action Comparison#
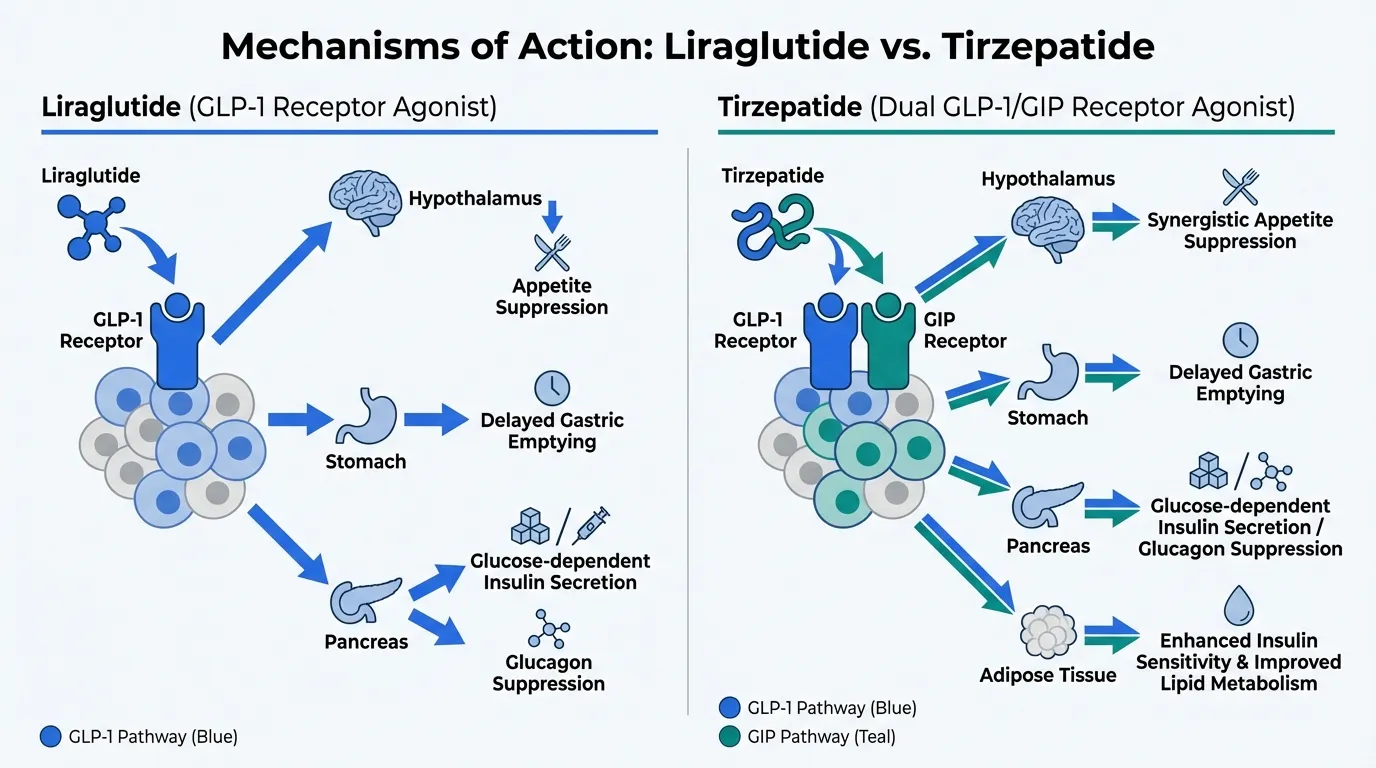
Liraglutide: Single Receptor Agonism#
Liraglutide activates only the GLP-1 receptor. This produces appetite suppression (via hypothalamic signaling), delayed gastric emptying, glucose-dependent insulin secretion, and glucagon suppression. It is a 31-amino acid peptide with 97% homology to native human GLP-1 and a C16 palmitic acid chain that enables albumin binding and a 13-hour half-life.
Tirzepatide: Dual Receptor Agonism#
Tirzepatide simultaneously activates both the GIP receptor and the GLP-1 receptor. It is a 39-amino acid synthetic peptide based on the GIP sequence with engineered GLP-1 receptor cross-reactivity. A C20 fatty diacid moiety enables albumin binding and a half-life of approximately 5 days.
The GIP receptor component provides complementary metabolic effects:
- Enhanced insulin sensitivity through direct action on adipose tissue
- Improved lipid metabolism via GIP-mediated effects on fat storage and mobilization
- Synergistic appetite suppression through combined incretin receptor activation in the hypothalamus
- Potentially better tolerated GI profile as GIP may partially offset GLP-1-mediated nausea
Key Pharmacological Differences#
| Property | Liraglutide | Tirzepatide |
|---|---|---|
| Receptor targets | GLP-1R only | GIP-R + GLP-1R |
| Amino acid length | 31 | 39 |
| Half-life | ~13 hours | ~5 days (120 hours) |
| Dosing | Once daily | Once weekly |
| Fatty acid | C16 palmitic acid | C20 fatty diacid |
| GLP-1 receptor affinity | Full agonist | Partial/biased agonist |
| GIP receptor affinity | None | Full agonist |
Weight Loss Efficacy#
Liraglutide (SCALE Program)#
The SCALE Obesity and Prediabetes trial (Pi-Sunyer et al., NEJM 2015) was the pivotal trial for Saxenda approval:
- 3,731 adults without diabetes, liraglutide 3.0 mg daily for 56 weeks
- Mean weight loss: 8.0% (vs 2.6% placebo)
- 63.2% achieved 5% or more weight loss
- 33.1% achieved 10% or more weight loss
Tirzepatide (SURMOUNT Program)#
The SURMOUNT-1 trial (Jastreboff et al., NEJM 2022) established tirzepatide as a leading obesity treatment:
- 2,539 adults without diabetes, tirzepatide 5/10/15 mg weekly for 72 weeks
- Mean weight loss at 15 mg: 20.9% (vs 2.4% placebo)
- Mean weight loss at 10 mg: 21.4%
- Mean weight loss at 5 mg: 16.0%
- 63.2% achieved 20% or more weight loss at 15 mg
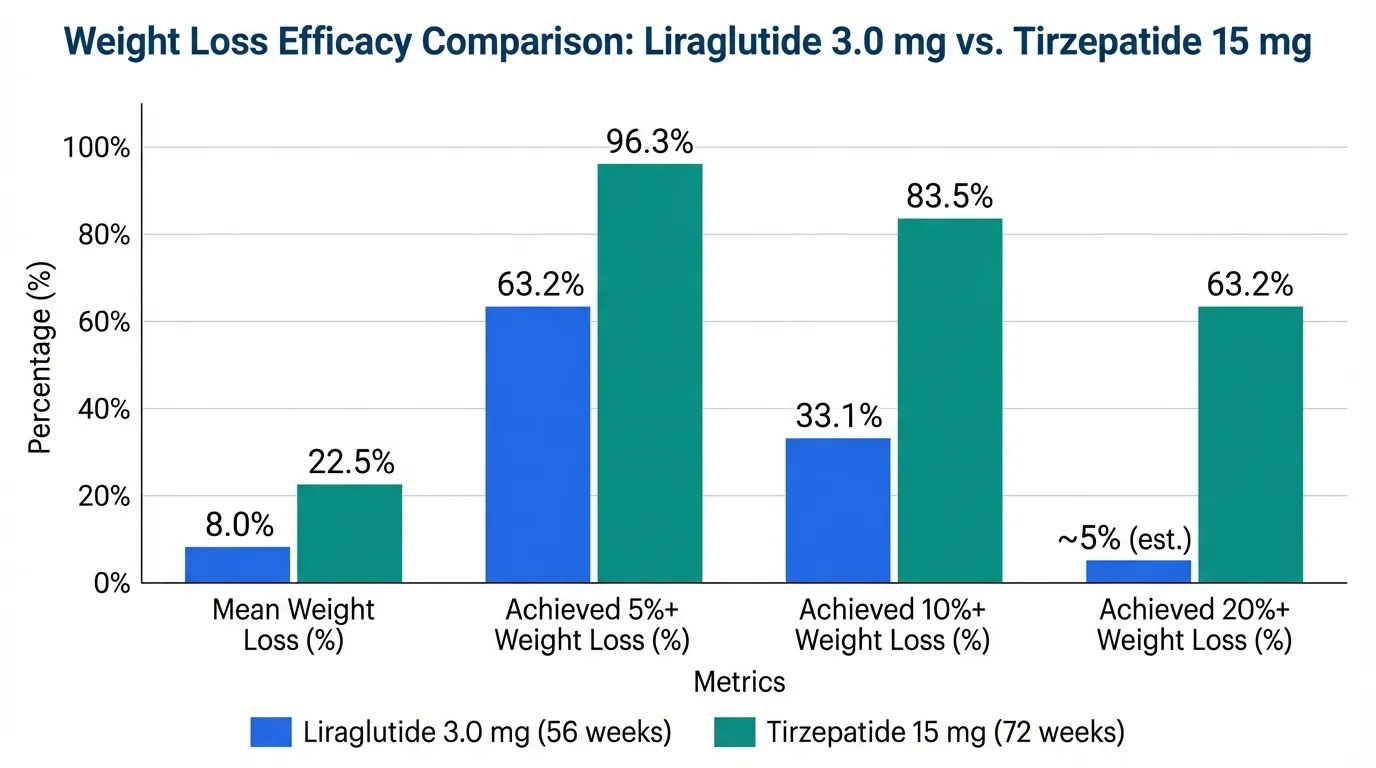
Cross-Trial Comparison#
While cross-trial comparisons have inherent limitations (different populations, durations, endpoints), the magnitude of difference is clear:
| Metric | Liraglutide 3.0 mg | Tirzepatide 15 mg |
|---|---|---|
| Mean weight loss | 8.0% (56 weeks) | 20.9% (72 weeks) |
| Achieved 5% or more | 63.2% | 96.3% |
| Achieved 10% or more | 33.1% | 83.5% |
| Achieved 20% or more | ~5% (estimated) | 63.2% |
Tirzepatide achieves approximately 2.8-fold greater mean weight loss, and the proportion reaching clinically meaningful thresholds is substantially higher across all categories.
Glycemic Control#
Liraglutide (LEAD Program)#
- LEAD trials demonstrated HbA1c reductions of 1.0-1.5% at 1.2-1.8 mg daily
- Victoza approved for T2D at max 1.8 mg daily
- Effective monotherapy and combination therapy for glucose control
Tirzepatide (SURPASS Program)#
- SURPASS-1 (monotherapy): HbA1c reduction of 2.07% at 15 mg over 40 weeks
- SURPASS-2 (vs semaglutide 1.0 mg): Superior HbA1c reduction (2.46% vs 1.86%)
- Up to 2.58% HbA1c reduction across SURPASS trials
Tirzepatide's dual incretin mechanism provides markedly superior glycemic control, driven by additive insulin-sensitizing and insulinotropic effects from both receptor pathways.
Cardiovascular Evidence#
LEADER Trial (Liraglutide)#
The LEADER trial (Marso et al., NEJM 2016) enrolled 9,340 patients with T2D and high CV risk, followed for median 3.8 years:
- 3-point MACE: HR 0.87 (95% CI 0.78-0.97, p=0.01) -- 13% reduction
- Cardiovascular death: HR 0.78 (22% reduction)
- All-cause mortality: HR 0.85 (15% reduction)
Liraglutide was the first GLP-1 agonist to demonstrate cardiovascular benefit, and LEADER remains a landmark trial in the class.
Tirzepatide CVOT (Pending)#
The SURPASS-CVOT trial is ongoing and will evaluate tirzepatide's cardiovascular outcomes in T2D. No completed dedicated CVOT data are available yet. However, the metabolic improvements observed in SURPASS and SURMOUNT (weight loss, glycemic control, lipid changes, blood pressure reduction) provide strong mechanistic rationale for expected cardiovascular benefit.
This is a meaningful limitation for tirzepatide: until the CVOT is complete, liraglutide has a stronger evidence base for CV risk reduction in patients where this is the primary treatment goal.
Dosing and Administration#
Liraglutide#
- Saxenda (obesity): Start 0.6 mg daily, increase by 0.6 mg weekly to target 3.0 mg (5-week titration)
- Victoza (T2D): Start 0.6 mg daily, increase to 1.2 mg, max 1.8 mg
- Subcutaneous injection daily at any time, with or without food
- Multi-dose pen, 6 mg/mL concentration
- 365 injections per year at maintenance
Tirzepatide#
- Zepbound (obesity): Start 2.5 mg weekly for 4 weeks, then 5 mg; escalate monthly as tolerated to max 15 mg
- Mounjaro (T2D): Same escalation schedule
- Subcutaneous injection weekly, any time of day
- Single-dose pre-filled pen (KwikPen) or auto-injector
- 52 injections per year at maintenance
Safety Comparison#
| Safety Aspect | Liraglutide (SCALE) | Tirzepatide (SURMOUNT-1) |
|---|---|---|
| Nausea | 39% | 24-33% (dose-dependent) |
| Vomiting | 16% | 9-13% |
| Diarrhea | 21% | 18-25% |
| Constipation | 19% | 11-17% |
| Discontinuation due to AEs | ~10% | 4.3-7.1% |
| Thyroid C-cell warning | Boxed warning | Boxed warning |
| Pancreatitis risk | Post-marketing signal | Post-marketing signal |
Despite producing substantially greater weight loss, tirzepatide has comparable or lower rates of GI adverse events and treatment discontinuation compared to liraglutide. This may reflect the modulatory effect of GIP receptor activation on GLP-1-mediated nausea, as well as the once-weekly dosing that provides more stable drug levels.
Key Differences Summary#
| Feature | Liraglutide | Tirzepatide |
|---|---|---|
| Receptor targets | GLP-1 only | GIP + GLP-1 |
| Dosing frequency | Daily | Weekly |
| Weight loss (obesity trials) | 8.0% (56 weeks) | 20.9% (72 weeks) |
| HbA1c reduction (T2D) | 1.0-1.5% | Up to 2.58% |
| CV outcomes trial | LEADER (13% MACE reduction) | Pending (SURPASS-CVOT) |
| Injections per year | 365 | 52 |
| FDA approval year | 2010 (T2D), 2014 (obesity) | 2022 (T2D), 2023 (obesity) |
| Pediatric obesity approval | Ages 12+ (Saxenda) | Not yet approved |
| Cost trajectory | Biosimilars emerging | Patent-protected |
Conclusion#
The comparison between liraglutide and tirzepatide illustrates the advancement from first-generation single-agonist to next-generation dual-agonist incretin therapy. Tirzepatide's dual GIP/GLP-1 mechanism produces approximately 2.8-fold greater weight loss, substantially better glycemic control, lower treatment discontinuation rates, and the convenience of weekly dosing. Liraglutide's completed LEADER cardiovascular outcomes trial remains its most significant differentiator, providing proven CV risk reduction evidence that tirzepatide has not yet matched. For most patients seeking weight management or glycemic control, tirzepatide is the more effective option. Liraglutide may retain relevance in adolescent obesity (ages 12+), cost-sensitive situations where biosimilars offer savings, and clinical settings where a completed CVOT is required for prescribing decisions.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Maximum weight loss
Tirzepatide
SURMOUNT-1 showed 20.9% mean weight loss at 15 mg, approximately 3-fold greater than liraglutide SCALE results (8.0%)
Type 2 diabetes glycemic control
Tirzepatide
SURPASS trials demonstrated up to 2.58% HbA1c reduction, superior to all tested comparators including semaglutide
Proven cardiovascular risk reduction
Liraglutide
LEADER trial provides completed evidence of 13% MACE reduction; tirzepatide CVOT is still ongoing
Weekly dosing preference
Tirzepatide
Once-weekly injection (52 per year) vs once-daily liraglutide (365 per year), a 7-fold reduction in injection burden
Adolescent obesity or cost-sensitive settings
Liraglutide
Saxenda approved for ages 12+; biosimilar and generic competition may offer lower cost access to GLP-1 therapy
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Liraglutide vs Tirzepatide: Daily Single Agonist vs Weekly Dual Agonist
Which is better, Liraglutide or Tirzepatide?
Tirzepatide is substantially superior to liraglutide in weight loss efficacy (20.9% vs 8.0%), glycemic control (HbA1c -2.58% vs -1.5%), and dosing convenience (weekly vs daily injection). The dual GIP/GLP-1 mechanism provides complementary metabolic benefits that a single GLP-1 agonist cannot match. Liraglutide's main advantage is its completed cardiovascular outcomes trial (LEADER) demonstrating 13% MACE reduction, while tirzepatide's CVOT is still pending. For patients where cardiovascular ... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Liraglutide and Tirzepatide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Tirzepatide; Weight Loss Efficacy: advantage goes to Tirzepatide; Glycemic Control: advantage goes to Tirzepatide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Tirzepatide over Liraglutide?
For the scenario of "Maximum weight loss," research data suggests Tirzepatide may be more relevant. SURMOUNT-1 showed 20.9% mean weight loss at 15 mg, approximately 3-fold greater than liraglutide SCALE results (8.0%). This is based on currently available evidence and individual circumstances may differ.
How do Liraglutide and Tirzepatide differ in their mechanisms of action?
Liraglutide: Selective GLP-1 receptor agonist only. C16 fatty acid chain extends half-life to 13 hours for once-daily injection. 97% homology to human GLP-1. First-generation acylated GLP-1 analog. Single-pathw.... Tirzepatide: First-in-class dual GIP and GLP-1 receptor agonist. C20 fatty diacid extends half-life to approximately 5 days for once-weekly injection. GIP receptor agonism provides complementary metabolic effec....
In what scenario might Tirzepatide be preferred?
For "Type 2 diabetes glycemic control," Tirzepatide may be more appropriate. SURPASS trials demonstrated up to 2.58% HbA1c reduction, superior to all tested comparators including semaglutide. Individual factors and clinical context should guide any decisions.
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.