CT-388 vs Tirzepatide: Signaling-Biased Dual Agonist vs Market Leader
Comparison of CT-388 (Roche/Carmot) and tirzepatide (Mounjaro/Zepbound), two dual GLP-1/GIP agonists with different signaling profiles, weight loss data, and development status.
Verdict at a Glance
Tirzepatide remains the proven standard with FDA approval, extensive phase 3 data, and commercial availability. CT-388 is a compelling next-generation competitor with a novel signaling-biased mechanism that produced 22.5% weight loss in phase 2 at 48 weeks -- potentially competitive with tirzepatide's 20.9% at 72 weeks in SURMOUNT-1. CT-388's key innovation is minimizing beta-arrestin-mediated receptor desensitization, which may explain the sustained weight loss trajectory observed. However, CT-388 must still complete phase 3 trials to confirm these results in larger populations.
| Best for | Pick | Why |
|---|---|---|
| Available Treatment Now | Tirzepatide | Tirzepatide is FDA-approved as Mounjaro and Zepbound, with immediate availability. CT-388 is investigational and years from potential approval. |
| Type 2 Diabetes | Tirzepatide | Tirzepatide has robust T2D evidence with HbA1c reductions up to 2.58% and head-to-head superiority over semaglutide 1 mg. CT-388 has not been studied in diabetes-specific populations. |
| Potential for Greater Weight Loss (Future) | CT-388 | CT-388's 22.5% weight loss at 48 weeks with no plateau suggests potentially greater long-term efficacy. Its signaling-biased mechanism may sustain receptor activation longer than conventional agonists. |
| Novel Mechanism Approach (Future) | CT-388 | CT-388's signaling-biased design -- minimizing beta-arrestin recruitment and receptor desensitization -- represents a pharmacological innovation that may improve both efficacy and tolerability if confirmed in phase 3. |
| Established Safety Profile | Tirzepatide | Tirzepatide has data from over 14,000 trial participants plus real-world post-marketing surveillance since 2022. CT-388 has limited safety data from early clinical trials only. |
| Category | CT-388 | Tirzepatide | Advantage |
|---|---|---|---|
| Mechanism of Action | Signaling-biased dual GLP-1/GIP receptor agonist from Roche (via Carmot Therapeutics). Designed to minimize beta-arrestin recruitment, reducing receptor internalization and desensitization for prolonged pharmacological activity at both receptors. | First-in-class dual GIP/GLP-1 receptor agonist with imbalanced potency profile (~5x native GIP at GIPR, ~0.2x native GLP-1 at GLP-1R). A 39-amino-acid peptide with C20 fatty diacid for ~5-day half-life. Does not employ signaling bias. | CT-388 |
| Weight Loss Efficacy | Phase 2 demonstrated 22.5% placebo-adjusted weight loss at 48 weeks with 24 mg dose. 87% of participants achieved at least 10% weight loss, and 26.1% achieved 30% or more. Weight loss had not plateaued at study end. | SURMOUNT-1 demonstrated 20.9% mean weight loss at 72 weeks with 15 mg. Up to 36% of participants achieved 25% or more weight loss. SURPASS-2 showed superiority over semaglutide 1 mg for both weight and glycemic control. | Comparable |
| Research Evidence | Phase 1b and phase 2 data. Phase 1b showed 18.8% placebo-adjusted weight loss. Phase 2 showed 22.5% at 48 weeks. Phase 3 planned. No head-to-head comparisons. No cardiovascular outcomes data. | Extensive phase 3 programs (SURPASS, SURMOUNT) with over 14,000 patients. FDA-approved for T2D (Mounjaro) and obesity (Zepbound). Head-to-head superiority over semaglutide in SURPASS-2. SURPASS-CVOT underway. | Tirzepatide |
| Side Effect Profile | GI adverse events are primarily mild to moderate and consistent with the incretin class. Treatment discontinuation due to adverse events was low at 5.9% vs 1.3% placebo. Signaling-biased design may theoretically improve tolerability. | Well-characterized GI side effects. Nausea 12-33%, diarrhea 12-21%, vomiting 5-13%. Favorable tolerability compared to semaglutide in SURPASS-2. Discontinuation due to GI events was 4.3-7.1%. Years of post-marketing data. | Tirzepatide |
| Dosing Convenience | Once-weekly subcutaneous injection. Phase 2 tested doses up to 24 mg. Injectable formulation only. Roche also has an oral small molecule GLP-1 program (CT-996) separate from CT-388. | Once-weekly subcutaneous injection. Six dose strengths (2.5-15 mg) with single-dose pre-filled pens and hidden needle design. Injectable only. Well-established device and delivery system. | Comparable |

Introduction#
CT-388 and tirzepatide represent two approaches to dual GLP-1/GIP receptor agonism for obesity treatment. Tirzepatide (Mounjaro/Zepbound) by Eli Lilly is the established market leader, with the largest weight reductions of any approved anti-obesity drug and proven superiority over semaglutide. CT-388, developed by Carmot Therapeutics (acquired by Roche for $2.7 billion in 2023), introduces a novel concept: signaling-biased dual agonism designed to minimize receptor desensitization.
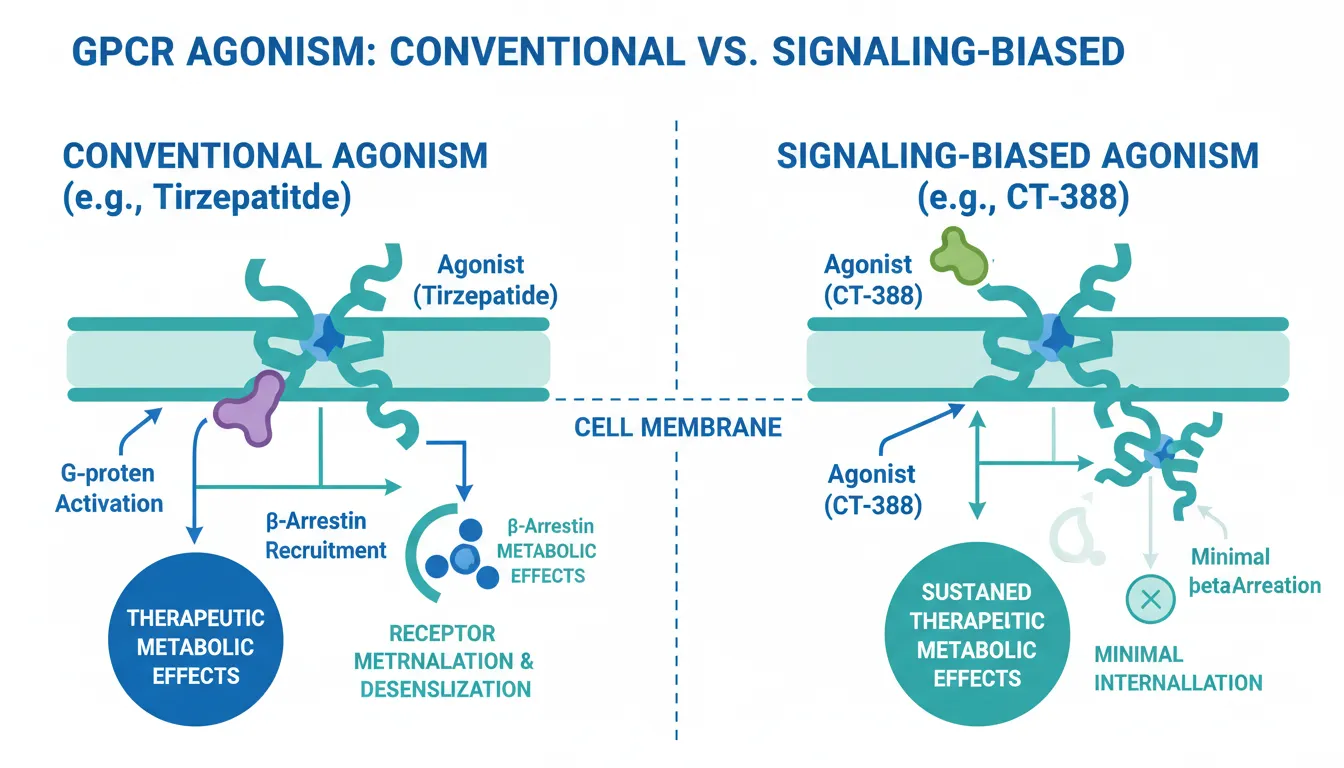
What makes CT-388 unique among dual agonists is its deliberate bias toward G-protein signaling while minimizing beta-arrestin recruitment. This pharmacological distinction has a practical implication: reduced receptor internalization may allow CT-388 to maintain its metabolic effects more consistently over time. The phase 2 results -- 22.5% weight loss at 48 weeks with no plateau -- provide early evidence that this approach may translate into meaningful clinical advantages.
Mechanism of Action Comparison#
CT-388#
CT-388 is a once-weekly subcutaneous dual GLP-1/GIP receptor agonist with a critical differentiating feature: signaling bias. CT-388 was designed to produce potent activation of both GLP-1 and GIP receptors while minimizing beta-arrestin recruitment on either receptor.
The significance of this design lies in receptor biology. Most GPCR agonists trigger two downstream pathways: G-protein signaling (which mediates the therapeutic metabolic effects) and beta-arrestin recruitment (which causes receptor internalization and desensitization). By biasing toward G-protein signaling, CT-388 reduces the rate of receptor downregulation, potentially sustaining pharmacological activity between doses.
Preclinical data showed that biased agonism at both GLP-1 and GIP receptors produced greater weight loss and better glycemic control than unbiased agonism in animal models.
Tirzepatide#
Tirzepatide is a 39-amino-acid synthetic peptide with conventional (non-biased) dual agonism at GIPR and GLP-1R. Its potency profile is imbalanced: approximately 5-fold greater potency at GIPR relative to native GIP and about 0.2-fold the potency of native GLP-1 at GLP-1R. A C20 fatty diacid at lysine-20 enables albumin binding and a half-life of approximately 5 days.
The dual activation produces synergistic effects on insulin secretion, glucagon suppression, gastric emptying delay, appetite reduction, and potentially lipid metabolism. Tirzepatide proved that dual incretin agonism produces superior outcomes to GLP-1 agonism alone in the SURPASS-2 head-to-head trial against semaglutide.
Mechanistic Comparison#
| Feature | CT-388 | Tirzepatide |
|---|---|---|
| Receptor targets | GLP-1R + GIPR | GLP-1R + GIPR |
| Signaling bias | G-protein biased (minimal beta-arrestin) | Conventional (unbiased) |
| Receptor desensitization | Reduced | Standard |
| Dosing frequency | Once weekly | Once weekly |
| Developer | Roche/Carmot | Eli Lilly |
| Development stage | Phase 2 completed | FDA-approved |
Dosing Comparison#
CT-388 Dosing#
CT-388 is administered as a once-weekly subcutaneous injection. Phase 2 studied doses up to 24 mg over 48 weeks. The dose escalation scheme and final phase 3 dosing have not been publicly confirmed. Roche plans to advance CT-388 into phase 3 trials.
Tirzepatide Dosing#
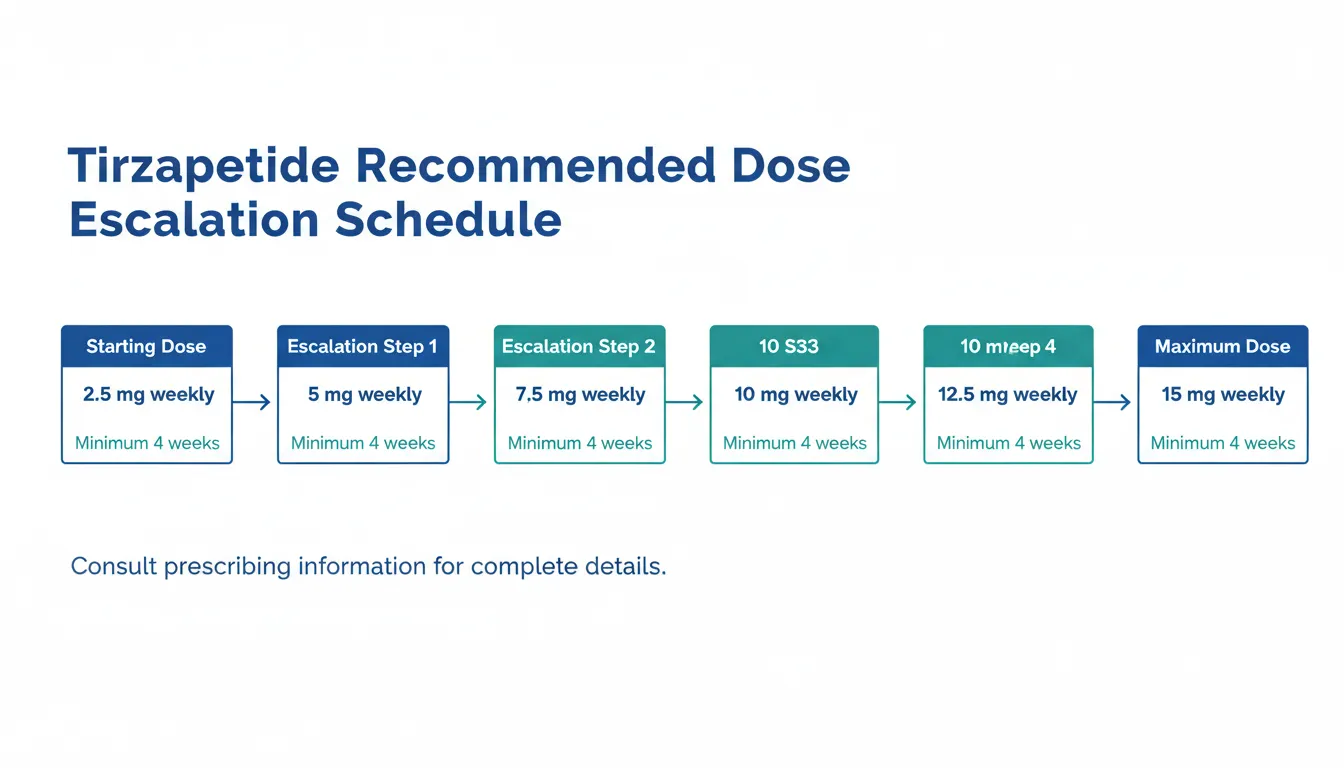
Tirzepatide uses a well-established escalation:
- Starting dose: 2.5 mg weekly for 4 weeks
- Escalation: 2.5 mg increments at minimum 4-week intervals
- Dose range: 2.5, 5, 7.5, 10, 12.5, 15 mg
- Maximum: 15 mg weekly
Supplied as single-dose pre-filled pens with hidden needle design.
Side Effects Comparison#
CT-388 Side Effects#
CT-388's safety profile is based on limited clinical data. GI adverse events were the most common class, consistent with the incretin mechanism, and were predominantly mild to moderate. The treatment discontinuation rate due to adverse events was low at 5.9% in CT-388 arms vs 1.3% in placebo. The signaling-biased mechanism may theoretically improve GI tolerability by reducing receptor desensitization, though this remains unproven in large trials.
Tirzepatide Side Effects#
Tirzepatide's side effect profile is well characterized through over 14,000 patients in SURPASS and SURMOUNT programs. Nausea 12-33%, diarrhea 12-21%, vomiting 5-13%. GI tolerability was comparable to or slightly better than semaglutide in the head-to-head SURPASS-2 trial despite producing greater metabolic effects. Tirzepatide carries a boxed warning for thyroid C-cell tumors based on rodent data.
Safety Comparison Table#
| Parameter | CT-388 | Tirzepatide |
|---|---|---|
| GI adverse events | Mild-moderate, class-consistent | Nausea 12-33%, vomiting 5-13% |
| Discontinuation (AEs) | 5.9% | 4.3-7.1% |
| Post-marketing data | None | Since 2022 |
| Boxed warning | Not yet determined | MTC/MEN2 |
| Long-term safety | Unknown | Growing dataset |
Research Evidence Comparison#
CT-388 Research#
CT-388 has early but notable clinical data:
- Phase 1b: Multi-arm, multi-cohort trial in adults with overweight/obesity and adults with obesity and T2D. Mean placebo-adjusted weight loss of 18.8%. 100% of participants achieved >5% loss, 85% >10%, 70% >15%, 45% >20%.
- Phase 2: At 48 weeks, the 24 mg dose produced 22.5% placebo-adjusted weight loss. 95.7% achieved at least 5%, 87% at least 10%, 47.8% at least 20%, 26.1% at least 30%. Weight had not plateaued.
- Phase 3: Planned by Roche
Evidence level: Low-moderate -- promising phase 1b/2 data with impressive responder rates, but small sample sizes and no head-to-head comparisons.
Tirzepatide Research#
- SURPASS (T2D): Five trials, >9,000 patients. SURPASS-2 showed superiority over semaglutide 1 mg: HbA1c -2.46% vs -1.86%, weight -12.4 kg vs -6.2 kg at 40 weeks
- SURMOUNT (obesity): SURMOUNT-1 demonstrated 20.9% mean weight loss at 72 weeks (15 mg). 36% achieved 25% or more
- SURPASS-CVOT: Cardiovascular outcomes trial underway
Evidence level: High -- large RCTs, head-to-head data, FDA-approved for two indications.
Key Differences Summary#
- Signaling bias: CT-388's primary innovation. By minimizing beta-arrestin recruitment, CT-388 may sustain receptor activation and reduce desensitization. Tirzepatide uses conventional agonism.
- Weight loss: CT-388 showed 22.5% at 48 weeks (phase 2). Tirzepatide showed 20.9% at 72 weeks (phase 3, SURMOUNT-1). Direct comparison is limited by different study designs, durations, and patient populations.
- Responder rates: CT-388 had 26.1% of participants losing 30% or more body weight. Tirzepatide had 36% losing 25% or more.
- Evidence maturity: Tirzepatide has extensive phase 3 data and FDA approval. CT-388 has phase 2 data and plans for phase 3.
- Regulatory status: Tirzepatide is commercially available. CT-388 is years from potential approval.
- Combination potential: Roche has a separate oral GLP-1 program (CT-996) that could complement CT-388, similar to how Eli Lilly pairs tirzepatide with other pipeline assets.
Conclusion#
This comparison highlights how rapidly the dual agonist space is evolving. Tirzepatide established the paradigm -- proving that dual GLP-1/GIP agonism produces superior outcomes to GLP-1 agonism alone -- and remains the clear choice for patients today. Its extensive evidence base, FDA approval, and commercial availability are unmatched.
CT-388 represents a pharmacologically sophisticated refinement of the dual agonist concept. Its signaling-biased design addresses a fundamental limitation of conventional GPCR agonists: receptor desensitization over time. The phase 2 results are encouraging, with 22.5% weight loss at 48 weeks and no plateau suggesting that the biased mechanism may translate into sustained clinical benefit. The responder rate showing 26.1% of patients achieving 30% or more weight loss is particularly notable.
The key question is whether CT-388's signaling bias provides a clinically meaningful advantage over tirzepatide's conventional agonism in properly powered phase 3 trials. If confirmed, CT-388 could challenge tirzepatide's position as the most effective injectable dual agonist. Until then, tirzepatide remains the evidence-based standard of care.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Available Treatment Now
Tirzepatide
Tirzepatide is FDA-approved as Mounjaro and Zepbound, with immediate availability. CT-388 is investigational and years from potential approval.
Type 2 Diabetes
Tirzepatide
Tirzepatide has robust T2D evidence with HbA1c reductions up to 2.58% and head-to-head superiority over semaglutide 1 mg. CT-388 has not been studied in diabetes-specific populations.
Potential for Greater Weight Loss (Future)
CT-388
CT-388's 22.5% weight loss at 48 weeks with no plateau suggests potentially greater long-term efficacy. Its signaling-biased mechanism may sustain receptor activation longer than conventional agonists.
Novel Mechanism Approach (Future)
CT-388
CT-388's signaling-biased design -- minimizing beta-arrestin recruitment and receptor desensitization -- represents a pharmacological innovation that may improve both efficacy and tolerability if confirmed in phase 3.
Established Safety Profile
Tirzepatide
Tirzepatide has data from over 14,000 trial participants plus real-world post-marketing surveillance since 2022. CT-388 has limited safety data from early clinical trials only.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About CT-388 vs Tirzepatide: Signaling-Biased Dual Agonist vs Market Leader
Which is better, CT-388 or Tirzepatide?
Tirzepatide remains the proven standard with FDA approval, extensive phase 3 data, and commercial availability. CT-388 is a compelling next-generation competitor with a novel signaling-biased mechanism that produced 22.5% weight loss in phase 2 at 48 weeks -- potentially competitive with tirzepatide's 20.9% at 72 weeks in SURMOUNT-1. CT-388's key innovation is minimizing beta-arrestin-mediated receptor desensitization, which may explain the sustained weight loss trajectory observed. However, ... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between CT-388 and Tirzepatide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to CT-388; Weight Loss Efficacy: advantage goes to neither (tie); Research Evidence: advantage goes to Tirzepatide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Tirzepatide over CT-388?
For the scenario of "Available Treatment Now," research data suggests Tirzepatide may be more relevant. Tirzepatide is FDA-approved as Mounjaro and Zepbound, with immediate availability. CT-388 is investigational and years from potential approval.. This is based on currently available evidence and individual circumstances may differ.
How do CT-388 and Tirzepatide differ in their mechanisms of action?
CT-388: Signaling-biased dual GLP-1/GIP receptor agonist from Roche (via Carmot Therapeutics). Designed to minimize beta-arrestin recruitment, reducing receptor internalization and desensitization for prol.... Tirzepatide: First-in-class dual GIP/GLP-1 receptor agonist with imbalanced potency profile (~5x native GIP at GIPR, ~0.2x native GLP-1 at GLP-1R). A 39-amino-acid peptide with C20 fatty diacid for ~5-day half-....
Which has fewer side effects, CT-388 or Tirzepatide?
In terms of side effects and tolerability, the advantage goes to Tirzepatide. CT-388: GI adverse events are primarily mild to moderate and consistent with the incretin class. Treatment discontinuation due to adverse events was low at.... Tirzepatide: Well-characterized GI side effects. Nausea 12-33%, diarrhea 12-21%, vomiting 5-13%. Favorable tolerability compared to semaglutide in SURPASS-2. Di....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.