Liraglutide vs Semaglutide: Predecessor vs Successor GLP-1 Agonists
Evidence-based comparison of liraglutide (Saxenda/Victoza) and semaglutide (Wegovy/Ozempic), including the STEP 8 head-to-head trial, SCALE vs STEP data, and cardiovascular outcomes from LEADER and SELECT.
Verdict at a Glance
Semaglutide is superior to liraglutide across every major clinical dimension. The STEP 8 head-to-head trial demonstrated nearly 2.5-fold greater weight loss with semaglutide (15.8% vs 6.4%) and a lower discontinuation rate (3.2% vs 12.6%). Semaglutide also offers once-weekly dosing (vs daily), broader cardiovascular evidence (SELECT trial in non-diabetic obesity), and both injectable and oral formulations. Liraglutide retains value as a lower-cost option with a longer safety track record, and it remains the only GLP-1 approved for adolescent obesity (ages 12+).
| Best for | Pick | Why |
|---|---|---|
| Maximum weight loss efficacy | Semaglutide | STEP 8 showed 15.8% weight loss vs 6.4% with liraglutide; 70.9% achieved 10% or more vs 25.6% with liraglutide |
| Once-weekly injection convenience | Semaglutide | Once-weekly dosing (Wegovy/Ozempic) dramatically reduces injection burden vs daily liraglutide injections |
| Cardiovascular risk reduction in obesity without diabetes | Semaglutide | SELECT trial demonstrated 20% MACE reduction specifically in overweight/obese adults without diabetes |
| Adolescent obesity treatment | Liraglutide | Saxenda is approved for adolescents aged 12+ with obesity; semaglutide has more limited pediatric data |
| Lower cost or insurance access challenges | Liraglutide | Generic liraglutide and biosimilars are emerging, potentially offering lower-cost GLP-1 therapy compared to semaglutide |
| Category | Liraglutide | Semaglutide | Advantage |
|---|---|---|---|
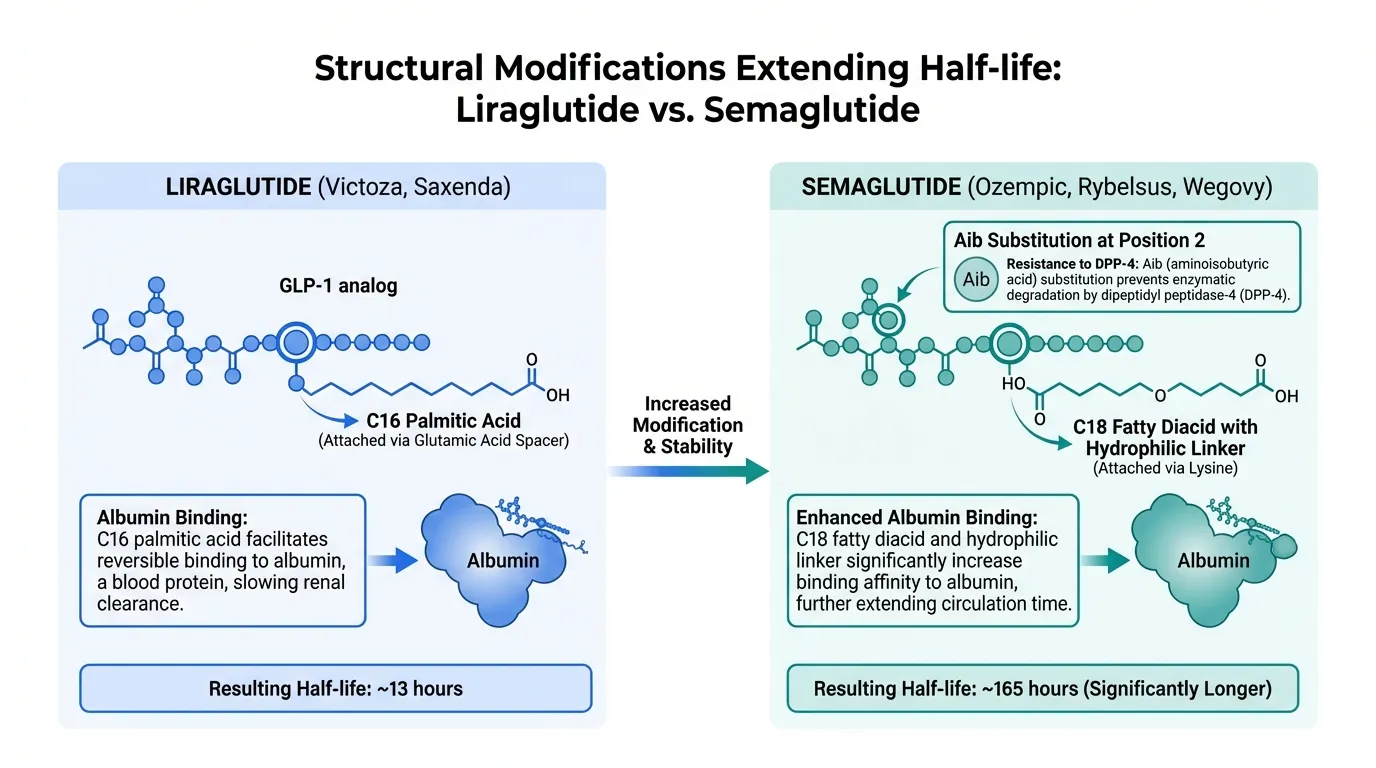
| Mechanism of Action | Selective GLP-1 receptor agonist with 97% homology to native GLP-1. C16 fatty acid chain enables albumin binding and extends half-life to 13 hours, requiring once-daily subcutaneous injection. First-generation acylated GLP-1 analog (Novo Nordisk, approved 2010/2014). | Selective GLP-1 receptor agonist with enhanced albumin binding via C18 fatty diacid chain, extending half-life to approximately 165 hours (7 days). Once-weekly injection or daily oral tablet. Second-generation acylated GLP-1 analog (Novo Nordisk, approved 2017/2021). | Semaglutide |
| Weight Loss Efficacy | SCALE Obesity trial showed 8.0% mean weight loss at 3.0 mg over 56 weeks. 63.2% achieved 5% or more weight loss. In the head-to-head STEP 8 trial, liraglutide achieved only 6.4% weight loss at 68 weeks. | STEP 1 demonstrated 14.9% mean weight loss at 2.4 mg over 68 weeks. In STEP 8 head-to-head, semaglutide achieved 15.8% vs liraglutide 6.4% (nearly 2.5-fold greater). 70.9% achieved 10% or more weight loss. | Semaglutide |
| Cardiovascular Evidence | LEADER trial (9,340 patients, median 3.8 years) demonstrated 13% reduction in 3-point MACE (CV death, nonfatal MI, nonfatal stroke) vs placebo in T2D with high CV risk. First GLP-1 agonist to prove CV benefit. | SELECT trial (17,604 patients, 39.8 months) demonstrated 20% reduction in MACE in overweight/obese adults without diabetes. Broader indication than LEADER. SUSTAIN 6 showed 26% MACE reduction in T2D. | Semaglutide |
| Dosing Convenience | Once-daily subcutaneous injection at any time of day. Requires 4-5 week titration (0.6 mg to 3.0 mg for weight loss). Pen device with disposable needles. No oral formulation for weight management. | Once-weekly subcutaneous injection (Wegovy/Ozempic) or once-daily oral tablet (Rybelsus, 14 mg for T2D; 25 mg oral approved for weight loss in 2025). Weekly injection greatly reduces injection burden. | Semaglutide |
| Safety and Tolerability | Well-characterized GI side effects (nausea, vomiting, diarrhea). In STEP 8, 12.6% discontinued due to adverse events. Longer track record (approved since 2010). Known risk profile with no novel safety signals after 15+ years of use. | Similar GI side effect profile. In STEP 8, only 3.2% discontinued due to adverse events despite greater weight loss. Lower discontinuation rate than liraglutide in head-to-head comparison. Post-marketing signal monitoring ongoing. | Semaglutide |

Introduction#
Liraglutide and semaglutide are both selective GLP-1 receptor agonists developed by Novo Nordisk, representing successive generations of the same drug class. Liraglutide (marketed as Victoza for diabetes, Saxenda for obesity) was the first GLP-1 agonist approved for chronic weight management (FDA 2014), while semaglutide (Ozempic/Wegovy/Rybelsus) arrived later with improved pharmacokinetics and substantially greater efficacy. The STEP 8 trial provided a definitive head-to-head comparison, establishing semaglutide's clear superiority.
This comparison examines the clinical data supporting each agent, including the landmark head-to-head trial, independent program data, cardiovascular outcomes, and practical considerations for treatment selection.
Mechanism of Action Comparison#
Shared GLP-1 Receptor Agonism#
Both liraglutide and semaglutide are synthetic analogs of human glucagon-like peptide-1 (GLP-1) with fatty acid modifications that enable albumin binding and resist DPP-4 degradation. They share the same receptor target and produce the same downstream effects: appetite suppression via hypothalamic signaling, delayed gastric emptying, enhanced glucose-dependent insulin secretion, and suppressed inappropriate glucagon release.
Key Pharmacokinetic Differences#
The critical difference lies in their albumin binding and metabolic stability:
| Property | Liraglutide | Semaglutide |
|---|---|---|
| Fatty acid modification | C16 palmitic acid | C18 fatty diacid via linker |
| Half-life | ~13 hours | ~165 hours (7 days) |
| Dosing frequency | Once daily | Once weekly (injection) or once daily (oral) |
| GLP-1 homology | 97% | ~94% (Aib at position 2) |
| Bioavailability (oral) | Not available | ~1% (with SNAC absorption enhancer) |
Semaglutide's longer half-life results from three structural modifications: an aminoisobutyric acid (Aib) substitution at position 2 that confers DPP-4 resistance, a C18 fatty diacid (vs C16 in liraglutide) that strengthens albumin binding, and a hydrophilic linker that optimizes the fatty acid orientation. These changes produce a 12-fold increase in half-life compared to liraglutide.
Weight Loss Efficacy#
Head-to-Head: STEP 8 Trial#
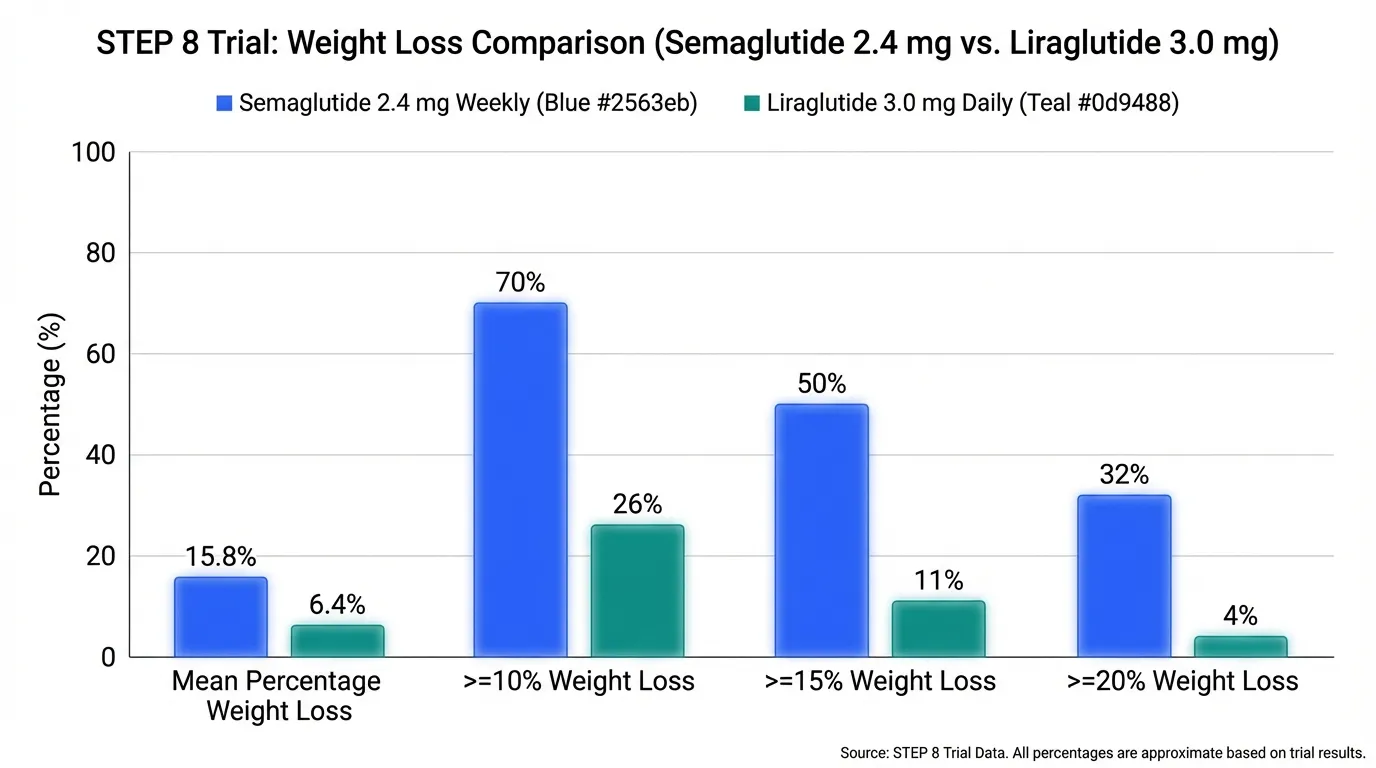
The STEP 8 trial (Rubino et al., JAMA 2022) directly compared semaglutide 2.4 mg weekly to liraglutide 3.0 mg daily in 338 adults with overweight or obesity without diabetes over 68 weeks. Results were unequivocal:
| Outcome | Semaglutide 2.4 mg | Liraglutide 3.0 mg |
|---|---|---|
| Mean weight loss | -15.8% | -6.4% |
| Achieved 10% or more loss | 70.9% | 25.6% |
| Achieved 15% or more loss | 38.5% | 12.0% |
| Achieved 20% or more loss | 25.6% | 6.0% |
Semaglutide achieved approximately 2.5-fold greater weight reduction than liraglutide. The separation between treatment groups was evident by week 12 and continued to widen through week 68.
Independent Program Data#
Liraglutide (SCALE program): The SCALE Obesity and Prediabetes trial (Pi-Sunyer et al., NEJM 2015) enrolled 3,731 adults without diabetes. Mean weight loss was 8.0% at 56 weeks with liraglutide 3.0 mg vs 2.6% with placebo. 63.2% achieved 5% or more weight loss.
Semaglutide (STEP program): STEP 1 (Wilding et al., NEJM 2021) enrolled 1,961 adults without diabetes. Mean weight loss was 14.9% at 68 weeks with semaglutide 2.4 mg vs 2.4% with placebo. 86.4% achieved 5% or more weight loss.
The STEP 8 head-to-head data eliminates confounders inherent in cross-trial comparisons and definitively establishes semaglutide's superiority in this population.
Cardiovascular Outcomes#
LEADER Trial (Liraglutide)#
The LEADER trial (Marso et al., NEJM 2016) enrolled 9,340 patients with type 2 diabetes and high cardiovascular risk. Liraglutide 1.8 mg daily reduced 3-point MACE by 13% vs placebo (HR 0.87, 95% CI 0.78-0.97, p=0.01). This was the first GLP-1 agonist to demonstrate cardiovascular benefit. The trial also showed a 22% reduction in cardiovascular death.
SELECT Trial (Semaglutide)#
The SELECT trial (Lincoff et al., NEJM 2023) enrolled 17,604 adults aged 45 or older with overweight or obesity and established cardiovascular disease, but without diabetes. Semaglutide 2.4 mg weekly reduced MACE by 20% vs placebo (HR 0.80, 95% CI 0.72-0.90, p<0.001). This was the first cardiovascular outcomes trial in obesity (rather than diabetes) and established GLP-1 agonist benefit independent of glucose-lowering effects.
Both agents have proven cardiovascular benefit, but semaglutide's evidence extends to the overweight/obese non-diabetic population, a substantially broader indication.
Dosing and Administration#
Liraglutide#
- Saxenda (obesity): Start 0.6 mg daily, titrate weekly by 0.6 mg to 3.0 mg daily (5-week titration)
- Victoza (T2D): Start 0.6 mg daily, increase to 1.2 mg, max 1.8 mg daily
- Subcutaneous injection, abdomen/thigh/upper arm
- Any time of day, with or without food
- No oral weight management formulation
Semaglutide#
- Wegovy (obesity): Start 0.25 mg weekly, titrate monthly to 2.4 mg weekly (16-week titration)
- Ozempic (T2D): Start 0.25 mg weekly, titrate to 0.5 mg, max 2.0 mg weekly
- Rybelsus (T2D): 3 mg daily oral for 30 days, then 7 mg, max 14 mg
- Oral semaglutide 25 mg (approved 2025): Oral formulation for weight management
- Weekly injection or daily oral tablet; taken on empty stomach for oral
Safety Comparison#
STEP 8 Head-to-Head Safety#
In the STEP 8 trial, overall adverse event rates were similar (semaglutide 95.2% vs liraglutide 96.1%), but discontinuation rates were notably different:
| Safety Outcome | Semaglutide | Liraglutide |
|---|---|---|
| Any adverse event | 95.2% | 96.1% |
| GI adverse events | ~70% | ~68% |
| Discontinuation due to AEs | 3.2% | 12.6% |
| Nausea | ~44% | ~48% |
The substantially lower discontinuation rate with semaglutide (3.2% vs 12.6%) suggests better tolerability despite greater pharmacological effect. This may reflect the gradual dose escalation with weekly dosing that allows adaptation to GI side effects.
Long-Term Safety#
Liraglutide has a longer post-marketing track record (approved 2010 vs 2017) with over 15 years of safety data. Both agents carry the same class warnings: boxed warning for thyroid C-cell tumors (rodent studies), risk of pancreatitis, and contraindication with personal/family history of medullary thyroid carcinoma or MEN 2 syndrome.
Key Differences Summary#
| Feature | Liraglutide | Semaglutide |
|---|---|---|
| Dosing | Daily injection | Weekly injection or daily oral |
| Weight loss (head-to-head) | 6.4% at 68 weeks | 15.8% at 68 weeks |
| CV outcomes trial | LEADER (T2D, 13% MACE reduction) | SELECT (obesity, 20% MACE reduction) |
| Discontinuation rate | 12.6% (STEP 8) | 3.2% (STEP 8) |
| Pediatric approval | Ages 12+ (Saxenda) | Limited pediatric data |
| Oral formulation | None for weight loss | 25 mg oral approved (2025) |
| Cost trajectory | Biosimilars emerging | Still patent-protected |
Conclusion#
The comparison between liraglutide and semaglutide illustrates the progress within the GLP-1 receptor agonist class. Semaglutide's structural improvements over liraglutide translate directly into superior clinical outcomes: approximately 2.5 times greater weight loss, lower treatment discontinuation, more convenient dosing, and broader cardiovascular evidence. For most adults seeking GLP-1-based obesity treatment, semaglutide is the clear first-line choice. Liraglutide may retain a role in pediatric obesity (ages 12+), cost-sensitive situations where biosimilars become available, or as a stepping stone for patients who prefer daily dosing flexibility before committing to weekly injections.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Maximum weight loss efficacy
Semaglutide
STEP 8 showed 15.8% weight loss vs 6.4% with liraglutide; 70.9% achieved 10% or more vs 25.6% with liraglutide
Once-weekly injection convenience
Semaglutide
Once-weekly dosing (Wegovy/Ozempic) dramatically reduces injection burden vs daily liraglutide injections
Cardiovascular risk reduction in obesity without diabetes
Semaglutide
SELECT trial demonstrated 20% MACE reduction specifically in overweight/obese adults without diabetes
Adolescent obesity treatment
Liraglutide
Saxenda is approved for adolescents aged 12+ with obesity; semaglutide has more limited pediatric data
Lower cost or insurance access challenges
Liraglutide
Generic liraglutide and biosimilars are emerging, potentially offering lower-cost GLP-1 therapy compared to semaglutide
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Liraglutide vs Semaglutide: Predecessor vs Successor GLP-1 Agonists
Which is better, Liraglutide or Semaglutide?
Semaglutide is superior to liraglutide across every major clinical dimension. The STEP 8 head-to-head trial demonstrated nearly 2.5-fold greater weight loss with semaglutide (15.8% vs 6.4%) and a lower discontinuation rate (3.2% vs 12.6%). Semaglutide also offers once-weekly dosing (vs daily), broader cardiovascular evidence (SELECT trial in non-diabetic obesity), and both injectable and oral formulations. Liraglutide retains value as a lower-cost option with a longer safety track record, and... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Liraglutide and Semaglutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Semaglutide; Weight Loss Efficacy: advantage goes to Semaglutide; Cardiovascular Evidence: advantage goes to Semaglutide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Semaglutide over Liraglutide?
For the scenario of "Maximum weight loss efficacy," research data suggests Semaglutide may be more relevant. STEP 8 showed 15.8% weight loss vs 6.4% with liraglutide; 70.9% achieved 10% or more vs 25.6% with liraglutide. This is based on currently available evidence and individual circumstances may differ.
How do Liraglutide and Semaglutide differ in their mechanisms of action?
Liraglutide: Selective GLP-1 receptor agonist with 97% homology to native GLP-1. C16 fatty acid chain enables albumin binding and extends half-life to 13 hours, requiring once-daily subcutaneous injection. Firs.... Semaglutide: Selective GLP-1 receptor agonist with enhanced albumin binding via C18 fatty diacid chain, extending half-life to approximately 165 hours (7 days). Once-weekly injection or daily oral tablet. Secon....
Which has fewer side effects, Liraglutide or Semaglutide?
In terms of side effects and tolerability, the advantage goes to Semaglutide. Liraglutide: Well-characterized GI side effects (nausea, vomiting, diarrhea). In STEP 8, 12.6% discontinued due to adverse events. Longer track record (approved.... Semaglutide: Similar GI side effect profile. In STEP 8, only 3.2% discontinued due to adverse events despite greater weight loss. Lower discontinuation rate tha....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.