Exenatide vs Liraglutide: First-Generation vs Second-Generation GLP-1 Agonists
Evidence-based comparison of exenatide (Byetta/Bydureon) and liraglutide (Victoza/Saxenda), including the LEAD-6 head-to-head trial, DURATION vs SCALE data, and the evolution from exendin-4-based to human GLP-1-based analogs.
Verdict at a Glance
Liraglutide is superior to exenatide across all major clinical dimensions. The LEAD-6 head-to-head trial demonstrated greater HbA1c reduction (1.12% vs 0.79%), fewer hypoglycemia events, and better tolerability. Liraglutide also has an FDA-approved obesity indication (Saxenda, 8.0% weight loss in SCALE), proven cardiovascular benefit (LEADER, 13% MACE reduction), and once-daily dosing without microsphere-related injection site reactions. Exenatide retains historical significance as the first GLP-1 agonist and may serve as a lower-cost option in resource-limited settings, but liraglutide is the preferred agent for new prescriptions among these two options.
| Best for | Pick | Why |
|---|---|---|
| Type 2 diabetes glycemic control | Liraglutide | LEAD-6 head-to-head showed superior HbA1c reduction with liraglutide (1.12% vs 0.79%) and higher proportion reaching target below 7% |
| Chronic weight management | Liraglutide | Saxenda (3.0 mg) is FDA-approved for obesity with 8.0% mean weight loss; exenatide has no obesity indication |
| Cardiovascular risk reduction in T2D | Liraglutide | LEADER proved 13% MACE reduction (superiority); EXSCEL achieved only non-inferiority for exenatide |
| Budget-constrained diabetes treatment | Exenatide | Lower cost and generic availability; 20 years of post-marketing safety experience; adequate for glycemic control when cost is primary concern |
| Patients intolerant of daily injections | Exenatide | Bydureon offers once-weekly dosing for patients who cannot tolerate daily liraglutide injections (though newer weekly agents are preferred) |
| Category | Exenatide | Liraglutide | Advantage |
|---|---|---|---|
| Mechanism of Action | Synthetic exendin-4 from Gila monster venom. 39 amino acids with 53% homology to human GLP-1. Naturally DPP-4 resistant. Byetta has 2.4-hour half-life (twice daily); Bydureon uses microsphere encapsulation for weekly dosing. First GLP-1 agonist (FDA 2005). | Synthetic human GLP-1 analog with 97% homology to native GLP-1. C16 fatty acid chain enables albumin binding and 13-hour half-life for once-daily dosing. No microsphere technology needed. Second-generation design (FDA 2010 for T2D, 2014 for obesity). | Liraglutide |
| Weight Loss Efficacy | Modest weight loss of 2-4 kg (2-4%) in DURATION trials for T2D. Not FDA-approved for obesity. Weight loss is secondary benefit only. LEAD-6 head-to-head showed 2.87 kg loss with exenatide vs 3.24 kg with liraglutide at 26 weeks. | SCALE trial demonstrated 8.0% mean weight loss at 3.0 mg over 56 weeks. FDA-approved for chronic weight management (Saxenda). Superior to exenatide in LEAD-6 head-to-head for weight. Only early GLP-1 agonist with obesity indication. | Liraglutide |
| Glycemic Control | DURATION-1 showed HbA1c reduction of 1.9% with Bydureon at 30 weeks. Effective for T2D but inferior to liraglutide in LEAD-6 head-to-head (0.79% vs 1.12% HbA1c reduction at 26 weeks). Anti-drug antibodies in ~45% may attenuate response. | LEAD-6 showed 1.12% HbA1c reduction vs 0.79% for exenatide at 26 weeks (statistically superior). 54% achieved HbA1c below 7% vs 42% with exenatide. Consistent glycemic control without anti-drug antibody issues. | Liraglutide |
| Cardiovascular Outcomes | EXSCEL trial (14,752 patients) demonstrated CV safety (non-inferiority) but not superiority for MACE (HR 0.91, p=0.06). 14% reduction in all-cause mortality was a secondary finding. Established CV safety only. | LEADER trial (9,340 patients) demonstrated 13% MACE reduction (HR 0.87, p=0.01) and 22% CV death reduction. First GLP-1 agonist with proven cardiovascular benefit. Statistically significant superiority. | Liraglutide |
| Safety and Tolerability | More persistent nausea than liraglutide in LEAD-6. Bydureon causes injection site nodules in ~10-15% due to microsphere formulation. 45% develop anti-drug antibodies. More minor hypoglycemia events than liraglutide (2.60 vs 1.93 events/patient/year in LEAD-6). | Less persistent nausea and fewer hypoglycemia events than exenatide in LEAD-6. No injection site nodules. Minimal anti-drug antibody formation. Better patient-reported outcomes (LEAD-6 PRO substudy). Higher treatment satisfaction scores. | Liraglutide |

Introduction#
Exenatide and liraglutide represent the first and second generations of GLP-1 receptor agonist therapy, both playing foundational roles in establishing the incretin drug class. Exenatide (Byetta/Bydureon), derived from Gila monster venom, was the first GLP-1 agonist approved in 2005. Liraglutide (Victoza/Saxenda) followed in 2010 as a human GLP-1 analog with improved pharmacokinetics and broader clinical utility, including the first GLP-1 obesity indication.
The LEAD-6 trial provided a definitive head-to-head comparison between these agents, and subsequent cardiovascular outcomes trials (EXSCEL and LEADER) further differentiated them. This comparison examines the clinical evidence, mechanistic differences, and practical considerations for each agent.
Mechanism of Action Comparison#
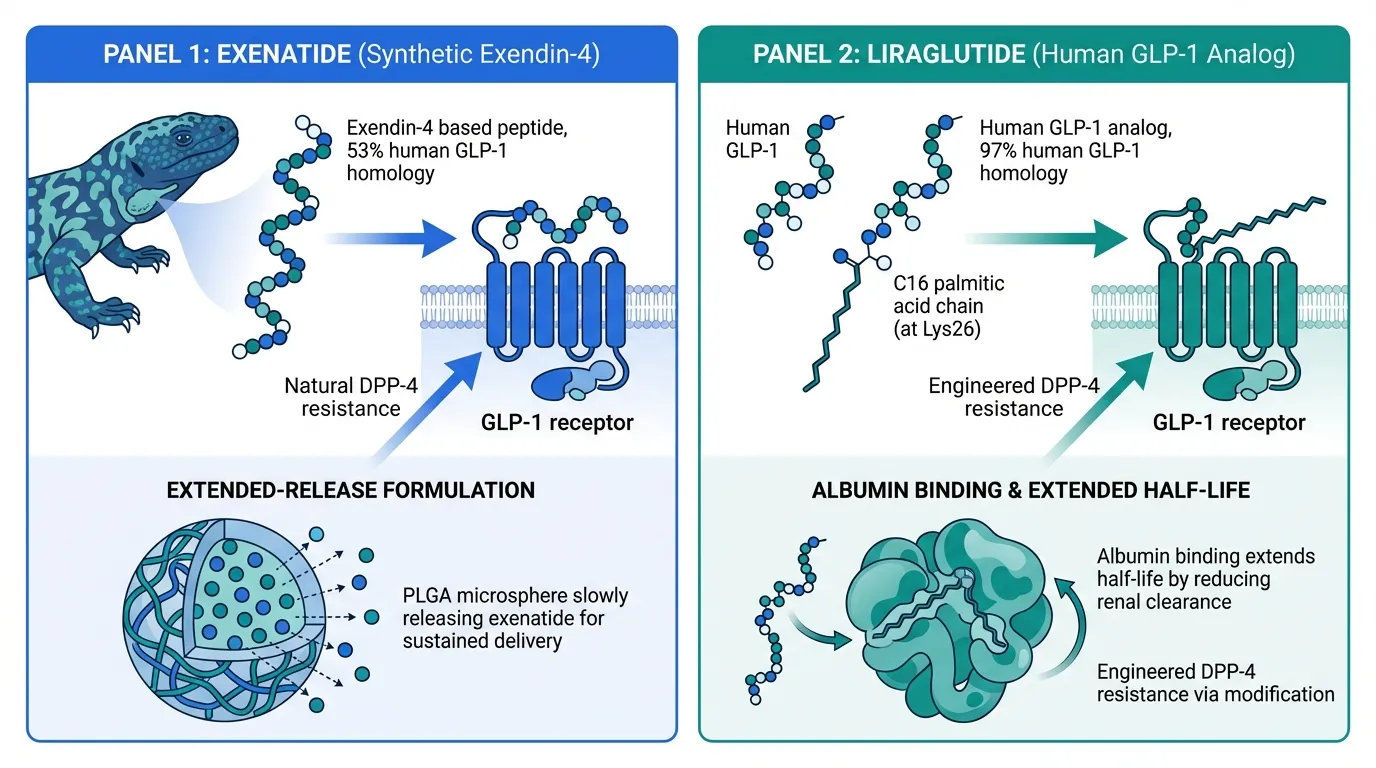
Exenatide: Exendin-4 Based#
Exenatide is a synthetic 39-amino acid peptide identical to exendin-4, isolated from the saliva of the Gila monster lizard (Heloderma suspectum). Despite only 53% homology to human GLP-1, exendin-4 is a full agonist at the GLP-1 receptor. Its non-human sequence confers natural resistance to DPP-4 degradation.
Two formulations address different pharmacokinetic needs:
- Byetta (immediate-release): 2.4-hour half-life, twice-daily injection 60 minutes before meals
- Bydureon (extended-release): Exenatide encapsulated in PLGA microspheres for sustained release, enabling once-weekly dosing
Liraglutide: Human GLP-1 Analog#
Liraglutide is a 31-amino acid peptide with 97% homology to native human GLP-1. A C16 palmitic acid chain attached at Lys26 enables reversible albumin binding, extending the half-life to approximately 13 hours and enabling once-daily dosing. Unlike exenatide ER, liraglutide achieves extended duration through molecular design rather than formulation technology.
Key Structural Differences#
| Property | Exenatide | Liraglutide |
|---|---|---|
| Origin | Gila monster venom (exendin-4) | Human GLP-1 analog |
| GLP-1 homology | 53% | 97% |
| DPP-4 resistance | Natural (non-human sequence) | Engineered (acylation) |
| Duration extension | Microsphere encapsulation (ER) | Albumin binding (fatty acid) |
| Anti-drug antibodies | Common (~45% with Bydureon) | Rare |
Head-to-Head: LEAD-6 Trial#
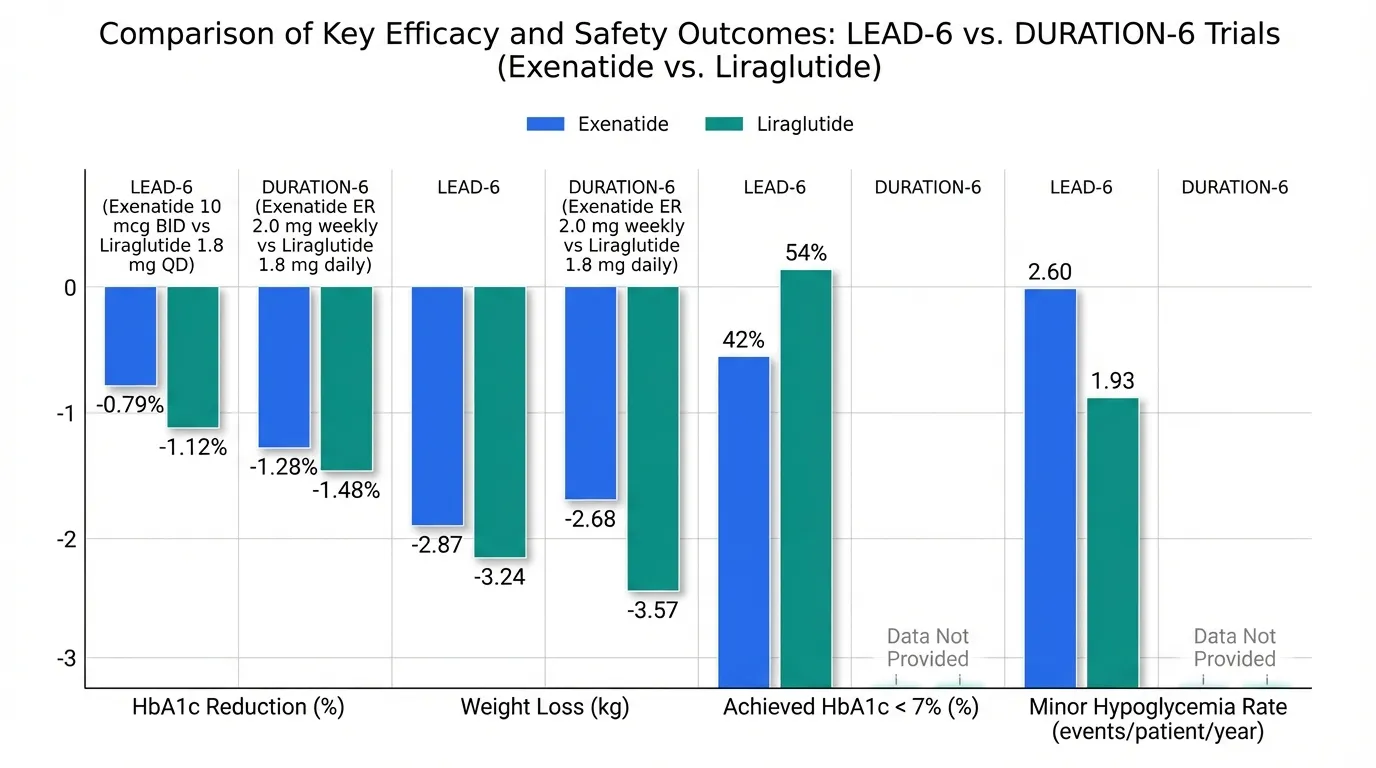
The LEAD-6 trial (Buse et al., Lancet 2009) directly compared liraglutide 1.8 mg once daily with exenatide 10 mcg twice daily in 464 adults with type 2 diabetes inadequately controlled on metformin, sulfonylurea, or both over 26 weeks:
| Outcome | Exenatide 10 mcg BID | Liraglutide 1.8 mg QD |
|---|---|---|
| HbA1c reduction | -0.79% | -1.12% |
| Achieved HbA1c < 7% | 42% | 54% |
| Weight loss | -2.87 kg | -3.24 kg |
| Minor hypoglycemia rate | 2.60 events/patient/year | 1.93 events/patient/year |
| Nausea (persistent) | More persistent | Less persistent |
Liraglutide was statistically superior for glycemic control and demonstrated better tolerability, with less persistent nausea and fewer hypoglycemia events.
DURATION-6 Confirmation#
The DURATION-6 trial (Buse et al., Lancet 2013) compared liraglutide 1.8 mg daily with exenatide ER 2.0 mg weekly in 912 patients with T2D over 26 weeks. Results confirmed liraglutide's superiority:
- HbA1c reduction: -1.48% (liraglutide) vs -1.28% (exenatide ER)
- Weight loss: -3.57 kg (liraglutide) vs -2.68 kg (exenatide ER)
Weight Loss Comparison#
Exenatide (DURATION Program)#
Exenatide was developed for type 2 diabetes, not weight management:
- DURATION-1: 3.7 kg weight loss with Bydureon over 30 weeks
- DURATION-5: 2.3 kg weight loss over 24 weeks
- Three-year extension: 2.3 kg sustained weight reduction
- No FDA approval for chronic weight management
Liraglutide (SCALE Program)#
Liraglutide was specifically developed for obesity at the higher 3.0 mg dose:
- SCALE Obesity and Prediabetes (Pi-Sunyer et al., NEJM 2015): 8.0% mean weight loss at 56 weeks
- 63.2% achieved 5% or more weight loss; 33.1% achieved 10% or more
- FDA-approved as Saxenda (2014) for chronic weight management
- Also approved for adolescent obesity (ages 12+)
The weight loss advantage of liraglutide over exenatide is approximately 2-3 fold when comparing the obesity-specific liraglutide dose to exenatide's diabetes-dose weight effects.
Cardiovascular Outcomes#
EXSCEL Trial (Exenatide)#
The EXSCEL trial (Holman et al., NEJM 2017) enrolled 14,752 patients with T2D (73.1% with prior CV disease):
- Primary MACE: HR 0.91 (95% CI 0.83-1.00, p=0.06 for superiority)
- Non-inferiority achieved; superiority narrowly missed
- All-cause mortality: HR 0.86 (p=0.016, secondary analysis)
LEADER Trial (Liraglutide)#
The LEADER trial (Marso et al., NEJM 2016) enrolled 9,340 patients with T2D and high CV risk:
- Primary MACE: HR 0.87 (95% CI 0.78-0.97, p=0.01)
- CV death: HR 0.78 (22% reduction)
- All-cause mortality: HR 0.85
LEADER established liraglutide as the first GLP-1 agonist with proven cardiovascular superiority, a distinction exenatide did not achieve.
Dosing and Administration#
Exenatide#
- Byetta: 5 mcg twice daily for 1 month, then 10 mcg twice daily; 60 minutes before meals
- Bydureon: 2 mg once weekly; requires reconstitution (microsphere suspension); any time of day
- Bydureon BCise: Simplified auto-injector version
Liraglutide#
- Victoza (T2D): 0.6 mg daily for 1 week, then 1.2 mg, max 1.8 mg daily
- Saxenda (obesity): 0.6 mg daily, increase weekly by 0.6 mg to 3.0 mg daily
- Subcutaneous injection at any time, with or without food
- Pre-filled multi-dose pen, no reconstitution
Safety Comparison#
| Safety Aspect | Exenatide | Liraglutide |
|---|---|---|
| Nausea | 44% (Byetta), 20% (Bydureon) | 29% (Victoza), 39% (Saxenda) |
| Injection site reactions | 10-15% nodules (Bydureon) | Rare |
| Anti-drug antibodies | ~45% (Bydureon) | Rare |
| Hypoglycemia (LEAD-6) | 33.6% (minor) | 25.5% (minor) |
| Pancreatitis signal | Post-marketing reports | Post-marketing reports |
| Thyroid C-cell warning | Boxed warning | Boxed warning |
| Post-marketing experience | 20+ years (since 2005) | 15+ years (since 2010) |
Bydureon's microsphere formulation causes subcutaneous nodules at injection sites in 10-15% of patients. Anti-drug antibodies develop in approximately 45% of Bydureon-treated patients but rarely affect clinical efficacy. Liraglutide avoids both of these issues through its albumin-binding molecular design.
Key Differences Summary#
| Feature | Exenatide | Liraglutide |
|---|---|---|
| Origin | Gila monster venom peptide | Human GLP-1 analog |
| FDA approval | 2005 (first GLP-1 agonist) | 2010 (T2D), 2014 (obesity) |
| Obesity indication | No | Yes (Saxenda) |
| HbA1c (LEAD-6 head-to-head) | -0.79% | -1.12% (superior) |
| Weight loss (obesity dose) | 2-4% (T2D doses only) | 8.0% (SCALE, Saxenda 3.0 mg) |
| CV outcomes | Non-inferiority only (EXSCEL) | Superiority proven (LEADER) |
| Injection site nodules | Yes (Bydureon) | No |
| Anti-drug antibodies | ~45% | Rare |
| Pediatric indication | No | Ages 12+ (Saxenda) |
Conclusion#
Liraglutide represents a meaningful advancement over exenatide across glycemic control (LEAD-6 and DURATION-6 head-to-head superiority), weight management (only agent with FDA obesity approval among the two), cardiovascular outcomes (LEADER superiority vs EXSCEL non-inferiority), and tolerability (less persistent nausea, no injection site nodules, minimal immunogenicity). Exenatide retains historical significance as the first GLP-1 agonist and proved that the incretin drug class was viable. It may still serve in cost-constrained settings where newer agents are unavailable. However, both exenatide and liraglutide have been largely superseded by semaglutide and tirzepatide for new prescriptions.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Type 2 diabetes glycemic control
Liraglutide
LEAD-6 head-to-head showed superior HbA1c reduction with liraglutide (1.12% vs 0.79%) and higher proportion reaching target below 7%
Chronic weight management
Liraglutide
Saxenda (3.0 mg) is FDA-approved for obesity with 8.0% mean weight loss; exenatide has no obesity indication
Cardiovascular risk reduction in T2D
Liraglutide
LEADER proved 13% MACE reduction (superiority); EXSCEL achieved only non-inferiority for exenatide
Budget-constrained diabetes treatment
Exenatide
Lower cost and generic availability; 20 years of post-marketing safety experience; adequate for glycemic control when cost is primary concern
Patients intolerant of daily injections
Exenatide
Bydureon offers once-weekly dosing for patients who cannot tolerate daily liraglutide injections (though newer weekly agents are preferred)
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Exenatide vs Liraglutide: First-Generation vs Second-Generation GLP-1 Agonists
Which is better, Exenatide or Liraglutide?
Liraglutide is superior to exenatide across all major clinical dimensions. The LEAD-6 head-to-head trial demonstrated greater HbA1c reduction (1.12% vs 0.79%), fewer hypoglycemia events, and better tolerability. Liraglutide also has an FDA-approved obesity indication (Saxenda, 8.0% weight loss in SCALE), proven cardiovascular benefit (LEADER, 13% MACE reduction), and once-daily dosing without microsphere-related injection site reactions. Exenatide retains historical significance as the first ... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Exenatide and Liraglutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Liraglutide; Weight Loss Efficacy: advantage goes to Liraglutide; Glycemic Control: advantage goes to Liraglutide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Liraglutide over Exenatide?
For the scenario of "Type 2 diabetes glycemic control," research data suggests Liraglutide may be more relevant. LEAD-6 head-to-head showed superior HbA1c reduction with liraglutide (1.12% vs 0.79%) and higher proportion reaching target below 7%. This is based on currently available evidence and individual circumstances may differ.
How do Exenatide and Liraglutide differ in their mechanisms of action?
Exenatide: Synthetic exendin-4 from Gila monster venom. 39 amino acids with 53% homology to human GLP-1. Naturally DPP-4 resistant. Byetta has 2.4-hour half-life (twice daily); Bydureon uses microsphere encap.... Liraglutide: Synthetic human GLP-1 analog with 97% homology to native GLP-1. C16 fatty acid chain enables albumin binding and 13-hour half-life for once-daily dosing. No microsphere technology needed. Second-ge....
Which has fewer side effects, Exenatide or Liraglutide?
In terms of side effects and tolerability, the advantage goes to Liraglutide. Exenatide: More persistent nausea than liraglutide in LEAD-6. Bydureon causes injection site nodules in ~10-15% due to microsphere formulation. 45% develop an.... Liraglutide: Less persistent nausea and fewer hypoglycemia events than exenatide in LEAD-6. No injection site nodules. Minimal anti-drug antibody formation. Bet....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.