Retatrutide Side Effects Guide

Retatrutide Side Effects Guide#
Introduction#
Retatrutide (LY3437943) represents a novel class of investigational metabolic therapy: a triple agonist targeting the glucose-dependent insulinotropic polypeptide (GIP), glucagon-like peptide-1 (GLP-1), and glucagon receptors simultaneously. Developed by Eli Lilly, retatrutide is under clinical investigation for obesity and type 2 diabetes (T2D), with its unique triple-receptor mechanism distinguishing it from dual agonists such as tirzepatide and single-receptor GLP-1 agonists like semaglutide and liraglutide.
As with any emerging therapeutic agent, understanding the safety and tolerability profile is essential for clinicians, researchers, and patients evaluating this compound. The safety data currently available are drawn primarily from phase 2 clinical trials conducted in both obesity and T2D populations. While these trials provide meaningful insight into common adverse events, dose-dependent patterns, and short-to-medium term tolerability, they also underscore areas where longer-term data remain limited.
This guide reviews the clinical evidence on retatrutide side effects, organized by system, severity, and dose relationship, to provide a thorough and evidence-based overview of its safety profile as understood through published trial data.
Understanding Retatrutide's Mechanism and Side Effect Profile#
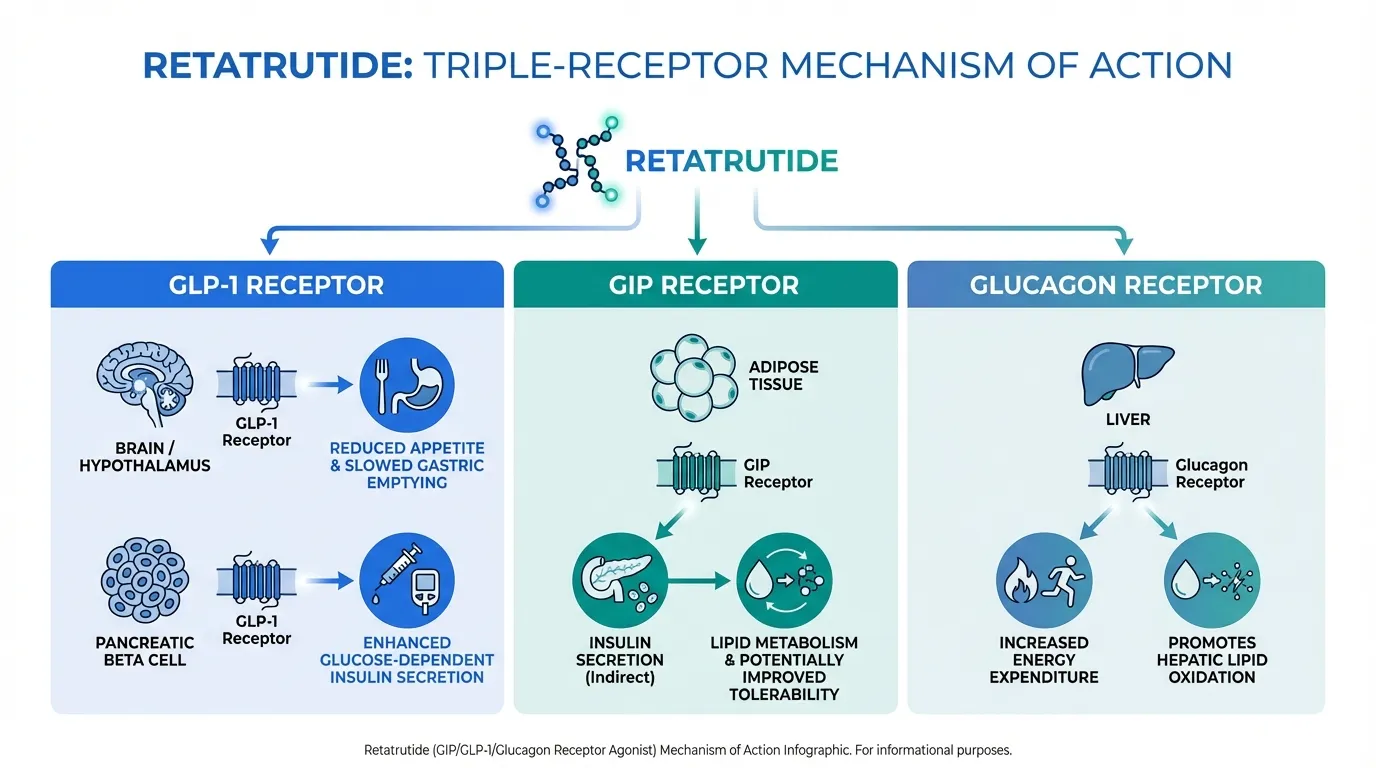
Retatrutide's triple-receptor agonism is central to both its therapeutic potential and its side effect profile. Each of its three target receptors contributes distinct physiological effects:
- GLP-1 receptor agonism reduces appetite, slows gastric emptying, and enhances glucose-dependent insulin secretion. This pathway is well characterized in the incretin therapy class and is the primary driver of the gastrointestinal side effects commonly observed with GLP-1-based treatments.
- GIP receptor agonism complements the GLP-1 pathway, contributing to insulin secretion, lipid metabolism, and potentially improved tolerability compared to GLP-1-only approaches. The GIP receptor is expressed in adipose tissue, bone, and the central nervous system, introducing a broader physiological footprint.
- Glucagon receptor agonism increases energy expenditure, promotes hepatic lipid oxidation, and may enhance weight loss beyond what GLP-1 or dual-agonist therapies achieve alone. However, glucagon receptor activation also raises theoretical considerations regarding hepatic glucose output and lipase activity.
The convergence of these three pathways means that the side effect profile of retatrutide reflects a composite of incretin-class effects and glucagon-mediated effects. The phase 2 trial data published to date suggest that the overall adverse event pattern is broadly consistent with the incretin-based therapy class, with gastrointestinal events predominating, but the glucagon component introduces nuances that warrant ongoing surveillance.
Gastrointestinal Effects#
Gastrointestinal adverse events are the most frequently reported side effects of retatrutide across phase 2 clinical trials, consistent with the well-established pattern seen with GLP-1 receptor agonists and dual GIP/GLP-1 agonists. These events represent the primary tolerability concern during treatment initiation and dose escalation.
Overall Incidence#
Across retatrutide treatment arms in phase 2 studies, approximately 35% of participants reported at least one gastrointestinal adverse event. This figure represents an aggregate across multiple dose levels, with considerable variation by dose cohort. By comparison, the placebo arm reported gastrointestinal adverse events in approximately 13% of participants, while the active comparator arm receiving dulaglutide (a GLP-1 receptor agonist) reported a rate of approximately 35%, comparable to the overall retatrutide figure.
Specific Gastrointestinal Events#
The most commonly reported gastrointestinal side effects included:
- Nausea was the single most frequent gastrointestinal complaint. It typically presented during the initial weeks of treatment or following dose escalation and tended to diminish over time as participants continued therapy.
- Diarrhea was the second most commonly reported event, occurring across dose levels and generally described as mild to moderate in intensity.
- Vomiting was reported less frequently than nausea but followed a similar temporal pattern, with higher incidence during dose titration periods.
- Constipation was also reported, reflecting the slowed gastrointestinal motility associated with GLP-1 receptor activation.
Severity and Duration#
The vast majority of gastrointestinal adverse events were classified as mild to moderate in severity. Severe gastrointestinal events were uncommon. Importantly, these events were largely transient, most pronounced during the dose-escalation phase and tending to resolve or diminish substantially as participants reached stable maintenance doses. This temporal pattern is consistent with the adaptation phenomenon well documented across the GLP-1 receptor agonist class.
Dose-Response Relationship in Gastrointestinal Events#
Gastrointestinal adverse event rates demonstrated a clear dose-dependent relationship. At lower retatrutide doses, the incidence was closer to 13%, while at the highest doses studied (8 mg and 12 mg), gastrointestinal adverse events affected up to approximately 50% of participants. This dose-response gradient is a key consideration for clinical dosing strategies and supports the use of gradual dose titration to mitigate tolerability concerns.
| Dose Level | Approximate GI AE Incidence | Characterization |
|---|---|---|
| Placebo | ~13% | Baseline rate |
| Low-dose retatrutide | ~13-20% | Similar to placebo |
| Mid-dose retatrutide | ~25-35% | Moderate increase |
| High-dose (8-12 mg) | ~40-50% | Highest incidence |
| Dulaglutide (comparator) | ~35% | Comparable to mid-range retatrutide |
Metabolic and Laboratory Effects#
Beyond gastrointestinal tolerability, the phase 2 trial data provide important information on metabolic safety parameters, hepatic effects, and laboratory markers.
Hypoglycemia#
No episodes of severe hypoglycemia were reported in phase 2 trials of retatrutide. Rare cases of moderate hypoglycemia were documented, predominantly in participants with type 2 diabetes who were receiving concomitant glucose-lowering therapies. This safety signal is consistent with the glucose-dependent mechanism of incretin-based insulin secretion, which carries an inherently lower risk of hypoglycemia compared to sulfonylureas or exogenous insulin. The absence of severe hypoglycemia across both the obesity and T2D study populations is a favorable finding, although real-world use in combination with other antidiabetic agents will require continued monitoring.
Lipase Elevations#
Infrequent increases in serum lipase levels were noted among retatrutide-treated participants. Elevated lipase is a recognized class effect of GLP-1 receptor agonists and has been observed with semaglutide, liraglutide, and tirzepatide. In the retatrutide trials, these elevations were generally asymptomatic, and no cases of confirmed acute pancreatitis were reported in published phase 2 data. However, lipase monitoring remains a prudent clinical consideration given the theoretical risk of pancreatitis across incretin-based therapies, and any symptoms of persistent severe abdominal pain should be evaluated promptly.
Hepatic Safety#
Hepatic safety is of particular interest for retatrutide given its glucagon receptor agonism, as glucagon signaling plays a direct role in hepatic lipid metabolism and glucose homeostasis. Data from the metabolic dysfunction-associated steatotic liver disease (MASLD) substudy, which evaluated hepatic endpoints through 48 weeks, did not identify hepatotoxicity signals. This is a reassuring finding for a compound that actively modulates hepatic metabolic pathways.
It is important to note that the MASLD substudy excluded participants with advanced hepatic fibrosis or cirrhosis. The safety of retatrutide in populations with more severe liver disease therefore remains unknown and will require dedicated investigation. For the population studied, however, the absence of hepatotoxicity through 48 weeks provides a meaningful data point supporting the hepatic safety of the compound at the doses evaluated.
Mortality#
No deaths were reported in the phase 2 clinical trial programs for retatrutide. While this is expected in relatively short-duration trials conducted in metabolically unwell but otherwise medically managed populations, it remains a relevant safety data point for an investigational agent.
Dose-Dependent Safety Patterns#
The phase 2 trial design allowed evaluation of retatrutide across a range of doses, providing insight into the dose-response characteristics of both efficacy and adverse events.
Low to Mid Doses#
At the lower end of the dosing range, retatrutide demonstrated gastrointestinal adverse event rates that were comparable to or only modestly higher than placebo. This suggests that the triple-agonist mechanism does not intrinsically produce poor tolerability at therapeutic doses and that the gastrointestinal burden is primarily a function of dose intensity and escalation speed.
Higher Doses (8-12 mg)#
At the higher doses of 8 mg and 12 mg, which also corresponded to the greatest weight loss and metabolic improvements observed in the trials, gastrointestinal adverse events became more frequent, affecting approximately 40-50% of participants in these cohorts. The most notable increases were in nausea and vomiting, while diarrhea and constipation also occurred at elevated rates relative to lower doses.
This dose-dependent pattern presents a familiar challenge in metabolic pharmacotherapy: the doses associated with maximal efficacy are also those associated with the greatest tolerability burden. However, the characterization of these events as predominantly mild to moderate and transient suggests that the higher doses remain clinically viable for most patients, particularly when appropriate titration strategies are employed.
Safety Floor#
Across all dose levels studied, no severe hypoglycemia, deaths, or hepatotoxicity signals were identified. This consistent safety floor across the dosing range is an important finding, indicating that the fundamental safety profile of retatrutide does not deteriorate at higher doses even as gastrointestinal tolerability becomes more challenging.
How Titration Affects Tolerability#
One of the more clinically actionable findings from the phase 2 trial program is the impact of dose titration speed on the tolerability profile of retatrutide.
Slow Versus Fast Escalation#
Phase 2 trials evaluated different titration schedules, including slow escalation protocols (for example, 2 mg to 4 mg to 8 mg, with defined intervals at each step) versus faster escalation approaches. The data demonstrate that the speed of dose escalation meaningfully influences the incidence and intensity of gastrointestinal adverse events.
Participants who underwent slower, stepwise titration experienced a more favorable tolerability profile during the escalation period, with lower peak incidence of nausea and vomiting compared to those who reached higher doses more quickly. This finding aligns with extensive clinical experience across the GLP-1 receptor agonist class, where gradual dose escalation is standard practice to improve patient adherence and reduce treatment discontinuation due to gastrointestinal intolerance.
Clinical Implications of Titration#
The titration data suggest that clinicians initiating retatrutide therapy, should it receive regulatory approval, would benefit from a structured, stepwise escalation protocol. The principle is straightforward: allowing the gastrointestinal system adequate time to adapt to incretin-mediated slowing of gastric motility and appetite suppression reduces the severity and duration of initial adverse events. This approach may also improve long-term adherence, as early intolerance is a significant driver of treatment discontinuation with incretin-based therapies.
For patients who experience gastrointestinal symptoms during titration, temporary dose maintenance (holding at the current dose for an additional period before escalating) may be a practical strategy, as it was in phase 2 protocols. The goal is to reach the target maintenance dose while preserving patient comfort and treatment continuity.
Comparison to Other GLP-1 Class Therapies#
Placing retatrutide's safety profile in context with approved incretin-based therapies is useful for understanding its relative tolerability.
Consistency With the Incretin Class#
The overall pattern of adverse events observed with retatrutide, dominated by gastrointestinal events that are dose-dependent, transient, and mostly mild to moderate, is broadly consistent with the established safety profile of the incretin therapy class. Semaglutide, liraglutide, tirzepatide, and dulaglutide all share this pattern. The phase 2 active comparator arm receiving dulaglutide reported a gastrointestinal adverse event rate of approximately 35%, which was comparable to the aggregate rate across retatrutide arms, suggesting that the addition of GIP and glucagon receptor agonism does not substantially worsen gastrointestinal tolerability beyond what is already expected from GLP-1-based therapies.
Differentiating Factors#
Where retatrutide may differ from existing therapies is in the implications of glucagon receptor agonism. The glucagon component introduces effects on hepatic metabolism and energy expenditure that are not present with GLP-1-only or GIP/GLP-1 dual agonists. While the phase 2 data have not revealed unique safety signals attributable to glucagon agonism, the theoretical considerations include potential effects on hepatic glucose output and lipase activity. These will require continued monitoring in larger and longer-duration studies.
The absence of severe hypoglycemia and the favorable hepatic safety data from the MASLD substudy are notable and suggest that the addition of glucagon receptor agonism does not introduce the metabolic destabilization that might theoretically be expected from activating a pathway that promotes hepatic gluconeogenesis.
Class-Wide Considerations#
Certain safety considerations apply broadly across all incretin-based therapies and are relevant for retatrutide:
- Pancreatitis risk: While no cases of confirmed pancreatitis were reported in phase 2 retatrutide trials, lipase elevations and the theoretical risk of pancreatitis remain a consideration for the class. Patients should be counseled on the symptoms of pancreatitis and instructed to seek medical evaluation for persistent severe abdominal pain.
- Gallbladder events: Rapid weight loss from any cause, including pharmacotherapy with incretin-based agents, is associated with increased risk of cholelithiasis. This class-wide consideration applies to retatrutide, particularly at higher doses that produce more substantial weight reduction.
- Thyroid C-cell tumors: GLP-1 receptor agonists carry label warnings regarding thyroid C-cell tumors based on rodent data. Whether this theoretical risk translates to humans remains uncertain after years of clinical use of GLP-1 agonists, but it is a standard class consideration.
What We Don't Yet Know#
While the phase 2 data provide a meaningful foundation for understanding retatrutide's safety profile, several important questions remain unanswered and will require data from ongoing and future clinical studies.
Cardiovascular Outcomes#
Longer-term cardiovascular safety and potential benefit have not yet been established for retatrutide. GLP-1 receptor agonists such as semaglutide and liraglutide have demonstrated cardiovascular risk reduction in dedicated outcomes trials (CVOTs), while tirzepatide has also generated favorable cardiovascular data. Whether retatrutide's triple-agonist mechanism provides comparable, superior, or different cardiovascular effects remains an open question that will require dedicated cardiovascular outcomes studies.
Renal Outcomes#
Similarly, the renal safety and potential renal protective effects of retatrutide have not been assessed in dedicated outcomes trials. Some GLP-1 receptor agonists have shown kidney-protective effects in clinical studies, but this cannot be extrapolated to retatrutide without direct evidence.
Long-Term Safety Beyond 48 Weeks#
The phase 2 trial data extend through approximately 48 weeks. The safety profile of retatrutide during chronic use over years, as would be expected with a therapy for obesity or T2D, remains to be characterized. Long-term studies will be essential for identifying any adverse events that emerge only with extended exposure.
Populations With Advanced Liver Disease#
The exclusion of participants with advanced hepatic fibrosis or cirrhosis from the MASLD substudy means that the hepatic safety of retatrutide in these populations is unknown. Given the compound's direct glucagon-mediated effects on hepatic metabolism, dedicated evaluation in patients with more advanced liver disease is warranted.
Rare Adverse Events#
Phase 2 trials are not powered to detect rare adverse events. Side effects with incidence rates below 1% may only become apparent in larger phase 3 trials or post-marketing surveillance. The transition from phase 2 to broader clinical use will inevitably expand the known safety profile.
Drug Interactions and Special Populations#
Comprehensive data on drug-drug interactions, safety in pregnancy and lactation, and tolerability in geriatric or renally impaired populations are not yet available from the published clinical trial program.
Conclusion#
The phase 2 clinical trial data for retatrutide reveal a safety and tolerability profile that is broadly consistent with the established incretin-based therapy class. Gastrointestinal adverse events, including nausea, diarrhea, vomiting, and constipation, are the most commonly reported side effects, occurring in approximately 35% of participants across dose groups. These events are dose-dependent, predominantly mild to moderate in severity, and largely transient during the dose-escalation phase.
Importantly, no severe hypoglycemia or deaths were reported in phase 2 trials. The MASLD substudy demonstrated no hepatotoxicity signals through 48 weeks in participants without advanced fibrosis or cirrhosis. Infrequent lipase elevations and rare moderate hypoglycemia were noted but did not constitute major safety concerns within the trial context.
The titration data offer a practical takeaway: slower, stepwise dose escalation meaningfully improves tolerability during the initiation phase. This finding is directly relevant to future clinical practice and underscores the importance of structured titration protocols.
However, significant gaps in the safety evidence remain. Cardiovascular and renal outcomes data are not yet available, long-term safety beyond 48 weeks has not been established, and populations with advanced liver disease have not been studied. As retatrutide progresses through phase 3 development and toward potential regulatory review, these questions will need to be addressed through larger, longer, and more diverse clinical studies.
For now, the available evidence supports the characterization of retatrutide as a well-tolerated investigational agent with a manageable side effect profile at the doses studied, provided that appropriate titration strategies are employed. Continued vigilance and comprehensive data collection through ongoing trials will be essential for building a complete picture of its safety in clinical practice.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:

{kind=link}
Frequently Asked Questions About Retatrutide Side Effects Guide
What does this article cover?
Retatrutide Side Effects: What the Research Shows — part of the Next-Gen Weight Loss content cluster. This article is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Retatrutide. Key context: Retatrutide (Referenced in cluster "Next-Gen Weight Loss"). Each peptide is discussed based on available research evidence.
Is this article based on research evidence?
This article draws on published research data and publicly available information about the peptides discussed. It is intended for educational purposes only. Pricing and availability may vary by region and change over time.
What is Retatrutide and why is it significant?
Retatrutide is a peptide discussed in this article because: Referenced in cluster "Next-Gen Weight Loss". For a complete profile of Retatrutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

The History of Peptide Research: From Insulin to Modern Therapeutics
History of peptide research from insulin's 1921 discovery to modern GLP-1 agonists. Key milestones in synthesis and therapeutics.

The Evolution of GLP-1 Receptor Agonists: From Single-Target to Multi-Receptor Metabolic Therapeutics
A research review tracing the evolution of GLP-1 receptor agonists from semaglutide through tirzepatide, retatrutide, and survodutide, examining how multi-receptor approaches have progressively expanded efficacy in obesity and metabolic disease.

Retatrutide Canada Guide
Retatrutide in Canada: Everything You Need to Know — part of the Next-Gen Weight Loss content cluster.
You Might Also Like
Related content you may find interesting