Retatrutide Canada Guide

Introduction#
Retatrutide (LY3437943) is among the most closely watched investigational compounds in metabolic medicine. Developed by Eli Lilly and Company, it is the first triple-receptor agonist targeting the GIP, GLP-1, and glucagon receptors simultaneously -- a mechanism of action that produced the highest weight loss figures ever reported in a clinical trial for obesity pharmacotherapy. In Phase 2 data published in 2023, the 12 mg dose achieved 24.2% body weight reduction at 48 weeks, surpassing both semaglutide and tirzepatide at comparable timepoints.
For Canadians, the compound is particularly relevant because multiple Phase 3 clinical trial sites are actively enrolling participants across the country, from Calgary to Montreal. However, retatrutide has not been approved by Health Canada and remains an investigational agent with no regulatory submission timeline publicly disclosed. This guide synthesizes the available clinical evidence, explains the triple-agonist mechanism, maps the Canadian trial landscape, and contextualizes retatrutide within the broader field of metabolic peptide therapeutics.
All data presented here are drawn from peer-reviewed publications, registered clinical trial databases (ClinicalTrials.gov), and official regulatory filings. This article is intended for educational purposes and does not constitute medical advice. Canadians interested in accessing retatrutide should consult their physician about clinical trial eligibility.
What Is Retatrutide?#
Retatrutide (LY3437943) is a once-weekly subcutaneous injectable peptide developed by Eli Lilly as a triple GIP/GLP-1/glucagon receptor agonist. Structurally, it is a fatty-acid conjugated peptide engineered to bind albumin in circulation, which extends its plasma half-life to approximately 6 days and enables weekly dosing.
The molecule was designed to engage three distinct metabolic receptor systems in a single compound:
- GIP receptor (glucose-dependent insulinotropic polypeptide): Retatrutide demonstrates the highest relative potency at this receptor, with approximately 8.9-fold activity compared to native GIP. This receptor drives incretin-mediated insulin secretion, central appetite regulation, and adipose tissue signaling.
- GLP-1 receptor (glucagon-like peptide-1): Relative potency at the GLP-1 receptor is approximately 0.4-fold compared to native GLP-1. Though lower than its GIP activity, this is sufficient to provide glucose-dependent insulin secretion, gastric motility modulation, and hypothalamic satiety signaling.
- Glucagon receptor: Relative potency at the glucagon receptor is approximately 0.3-fold compared to native glucagon. This component drives hepatic fat oxidation, thermogenesis via brown adipose tissue activation, and increased resting energy expenditure.
This receptor binding profile -- GIP-dominant with moderate GLP-1 and glucagon activity -- represents a deliberate pharmacological design. The GIP and GLP-1 components provide the counter-regulatory glucose-lowering effects necessary to offset glucagon's inherent hyperglycemic action, while glucagon's catabolic properties add metabolic benefits that neither GLP-1 nor GIP agonism alone can provide.
Retatrutide is administered via subcutaneous injection once weekly and is being evaluated in clinical trials across dose ranges from 0.5 mg to 12 mg, with dose escalation protocols designed to mitigate gastrointestinal side effects during initiation.
How Does It Work?#
The Triple-Agonist Mechanism#
To understand why retatrutide's triple-receptor approach is significant, it is useful to examine what each receptor contributes independently and how these contributions interact.
GLP-1 receptor agonism has been the foundation of incretin-based metabolic therapy since the development of exenatide and, more recently, semaglutide. GLP-1 receptor activation produces glucose-dependent insulin secretion (reducing hyperglycemia risk), suppresses inappropriate glucagon release in the fed state, delays gastric emptying (contributing to satiety), and activates central appetite-suppressive circuits in the hypothalamus and brainstem. Semaglutide, the benchmark GLP-1 monoagonist, achieves approximately 15-17% body weight loss through these mechanisms.
GIP receptor agonism was historically underappreciated in metabolic pharmacology. GIP was considered primarily an insulin secretagogue, and some early data even suggested that GIP receptor antagonism might benefit obesity. Tirzepatide's clinical success overturned this view, demonstrating that GIP agonism, when combined with GLP-1, activates partially distinct central satiety pathways and provides complementary effects on adipose tissue metabolism, beta-cell function, and bone health. The addition of GIP to GLP-1 increased weight loss from the 15-17% range to approximately 20.9% in Phase 3 trials.
Glucagon receptor agonism is the distinguishing feature of retatrutide. Glucagon is the body's primary counter-regulatory hormone to insulin, and its inclusion in a metabolic therapeutic initially appears paradoxical. However, glucagon has several metabolic effects beyond glycogenolysis that are therapeutically valuable:
- Hepatic fat oxidation: Glucagon potently stimulates beta-oxidation of fatty acids in the liver, directly reducing hepatic steatosis through a mechanism independent of weight loss.
- Thermogenesis: Glucagon activates brown adipose tissue and increases resting energy expenditure via futile metabolic cycling, contributing to caloric deficit without requiring additional appetite suppression.
- Amino acid catabolism: Glucagon promotes hepatic amino acid processing, with downstream effects on body composition.
- Central satiety: Glucagon signaling in the brain provides an additional appetite-suppressive input, partially independent of GLP-1 and GIP pathways.
The triple-agonist design of retatrutide captures all three mechanistic pathways: GLP-1 and GIP provide strong incretin-based appetite suppression and glucose control while counterbalancing glucagon's hyperglycemic potential; glucagon provides additional weight loss through energy expenditure and hepatic fat catabolism that neither incretin alone can achieve. The net effect is a metabolic profile that addresses appetite, glucose homeostasis, liver fat, and energy expenditure simultaneously through partially non-overlapping biological mechanisms.
Why the Receptor Ratio Matters#
Retatrutide's receptor binding profile is not uniform across its three targets. The approximately 8.9-fold potency at the GIP receptor, 0.4-fold at GLP-1, and 0.3-fold at glucagon reflects a deliberate optimization. High GIP activity maximizes incretin-mediated appetite suppression and glucose lowering. Moderate GLP-1 activity provides sufficient glycemic counter-regulation and satiety without the dose-limiting gastrointestinal effects seen at maximal GLP-1 engagement. Lower glucagon activity captures the catabolic and thermogenic benefits while minimizing the risk of clinically significant hyperglycemia. This ratio is a pharmacological balancing act -- enough glucagon to drive liver fat reduction and energy expenditure, enough GLP-1 and GIP to prevent glucagon from raising blood glucose, and enough of all three to produce weight loss exceeding what any single- or dual-receptor approach has demonstrated.
Clinical Trial Results#
Obesity#
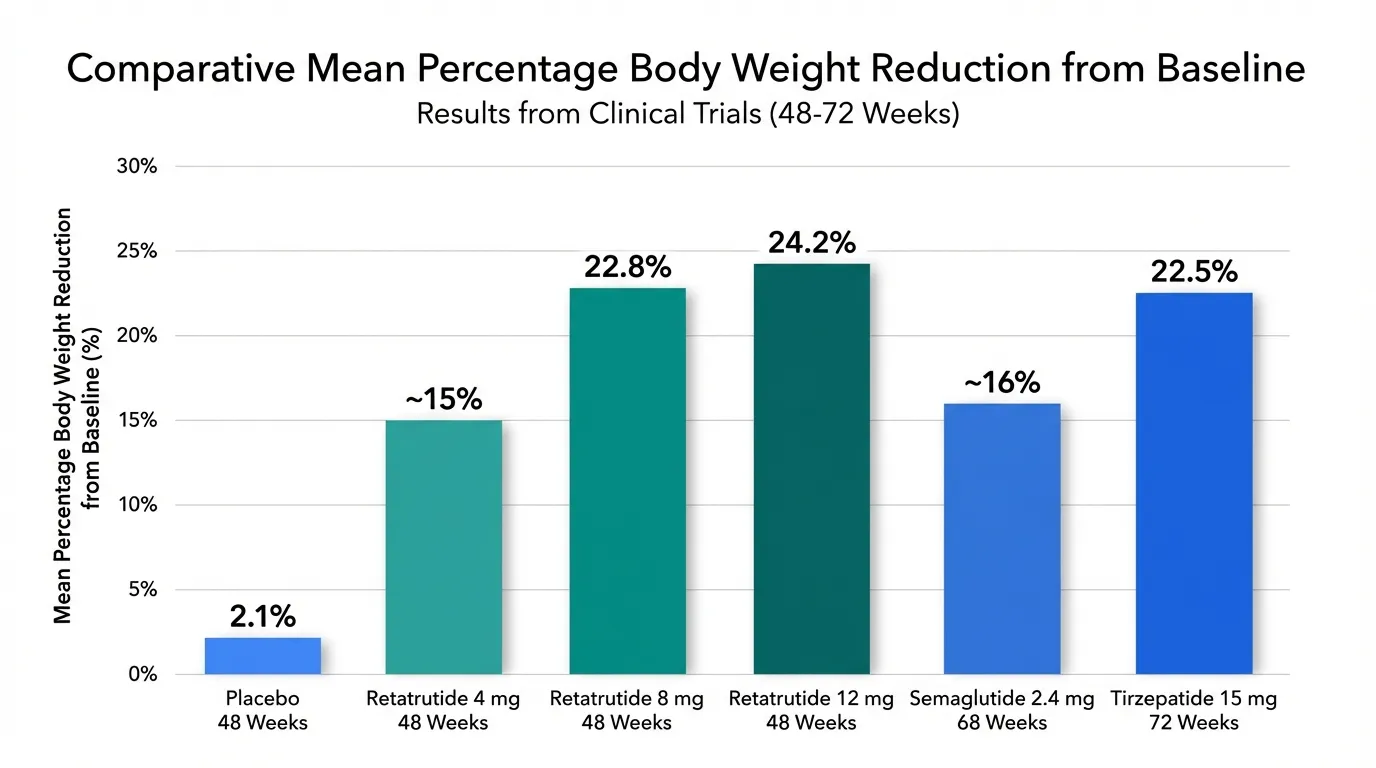
The Phase 2 obesity trial of retatrutide was published in the New England Journal of Medicine in 2023 and produced the highest weight loss figures reported for any pharmacological intervention in a controlled clinical trial at that time. The study evaluated multiple dose levels (1 mg, 4 mg, 8 mg, and 12 mg, administered weekly) against placebo over 48 weeks in adults with obesity or overweight with at least one weight-related comorbidity.
Key efficacy results at 48 weeks (Phase 2):
- Placebo: Approximately 2.1% weight loss
- 1 mg: Moderate weight loss, establishing a floor for the dose-response curve
- 4 mg: Intermediate weight loss with a favorable tolerability profile
- 8 mg: 22.8% mean body weight reduction from baseline
- 12 mg: 24.2% mean body weight reduction from baseline
These Phase 2 results have since been confirmed and exceeded by Phase 3 data. The TRIUMPH-4 trial demonstrated 28.7% mean weight loss at 68 weeks with the 12 mg dose -- the highest reported for any metabolic peptide in a Phase 3 trial. This exceeds semaglutide 2.4 mg (approximately 15-17% in the STEP program at 68 weeks) and tirzepatide 15 mg (20.9% in SURMOUNT-1 at 72 weeks) by a substantial margin.
The dose-response relationship was clear and monotonic, with each dose increment producing additional weight loss. This pattern is important for clinical dosing strategies, as it suggests that patients who tolerate escalation to higher doses will achieve proportionally greater benefit.
Type 2 Diabetes#
A separate Phase 2 trial evaluated retatrutide in adults with type 2 diabetes (T2D) over 36 weeks, assessing both glycemic and weight endpoints across doses from 0.5 mg to 12 mg weekly.
Glycemic control (HbA1c reductions at 24 weeks):
- 0.5 mg: -0.43% reduction from baseline
- 4 mg: Approximately -1.4% reduction
- 8 mg: Approximately -1.7% reduction
- 12 mg: -2.02% reduction from baseline
The HbA1c reduction of -2.02% at the 12 mg dose is comparable to the strongest reductions seen with tirzepatide in the SURPASS program (up to -2.59% at the 15 mg dose) and substantially exceeds semaglutide 1 mg (approximately -1.86% in SURPASS-2's comparator arm). These reductions brought a substantial proportion of participants to the clinically meaningful threshold of HbA1c below 7.0%, and many to below 5.7% (the normal range).
Weight loss in T2D (at 36 weeks):
- 0.5 mg: Approximately 3.2% body weight reduction
- 4 mg: Approximately 7-10% body weight reduction
- 8-12 mg: Approximately 16.9% body weight reduction
Weight loss in the T2D population was, as expected, somewhat lower than in the non-diabetic obesity population. This pattern is consistent across all incretin-based therapies and reflects the metabolic differences in individuals with established insulin resistance and diabetes. Nonetheless, 16.9% weight loss at 36 weeks in a T2D population exceeds what semaglutide or tirzepatide achieved at comparable timepoints in their respective T2D programs, suggesting that the triple-agonist mechanism provides incremental benefit even in this more treatment-resistant population.
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD)#
A prespecified substudy within the Phase 2 obesity trial evaluated retatrutide's effects on liver fat using magnetic resonance imaging-proton density fat fraction (MRI-PDFF), the gold standard noninvasive measurement of hepatic steatosis. This substudy produced what may be the most striking results of the entire retatrutide clinical program.
Liver fat reduction at 24 weeks (change from baseline by dose):
- Lower doses: -42.9% relative reduction in liver fat content
- Higher doses: Up to -82.4% relative reduction in liver fat content
An 82.4% reduction in liver fat content is extraordinary by any pharmacological standard. For comparison, semaglutide achieves approximately 30-40% liver fat reduction, and tirzepatide approximately 40-55%, primarily through weight-loss-mediated improvements in insulin sensitivity and hepatic metabolism. Retatrutide's glucagon component adds a direct hepatic fat oxidation mechanism that is independent of overall weight loss, explaining why its liver fat reductions far exceed what weight loss alone would predict.
The clinical significance of this finding extends beyond obesity treatment. MASLD affects an estimated 25-30% of the global adult population, and its progressive form -- metabolic dysfunction-associated steatohepatitis (MASH) -- is a leading cause of liver transplantation with very limited approved pharmacological treatments. If retatrutide's Phase 3 data confirm these liver fat reductions, the compound could become a transformative therapy for hepatic metabolic disease in addition to its primary obesity and diabetes indications.
Safety and Side Effects#
The Phase 2 clinical trial data for retatrutide demonstrated a safety profile broadly consistent with other incretin-based therapies, though with some features specific to its glucagon receptor component.
Gastrointestinal effects were the most commonly reported adverse events, as is typical for GLP-1 receptor-containing compounds:
- Nausea, vomiting, and diarrhea were the most frequent GI symptoms
- These events were predominantly mild to moderate in severity
- They were transient in nature, typically occurring during dose escalation and diminishing with continued treatment
- Incidence was dose-dependent, with higher rates at the 8 mg and 12 mg doses
- The 12 mg dose group showed somewhat higher diarrhea rates than would be expected with pure GLP-1 or GIP/GLP-1 agonists, potentially attributable to the glucagon receptor component
Glycemic safety was a key monitoring endpoint given glucagon's hyperglycemic potential:
- No severe hypoglycemia events were reported across any dose group
- Glucose homeostasis was maintained even at the highest doses, confirming that the GLP-1 and GIP components provide adequate counter-regulation against glucagon-mediated glucose elevation
- In the T2D population, retatrutide produced substantial HbA1c reductions rather than hyperglycemia, demonstrating that the receptor ratio effectively manages the glucagon-glucose interaction
Heart rate: Small mean increases of 2-4 beats per minute were observed at higher doses, consistent with glucagon-mediated sympathetic activation. This signal will require monitoring in Phase 3 cardiovascular outcomes data.
Hepatic effects: Transient elevations in liver enzymes (ALT, AST) were noted in some participants, occurring paradoxically in the context of dramatic liver fat reduction. This pattern may reflect hepatic remodeling during rapid fat mobilization rather than hepatotoxicity, but longer-term Phase 3 data will be essential to characterize this signal fully.
Discontinuation rates due to adverse events were low across all dose groups and comparable to rates seen in tirzepatide and semaglutide trials, suggesting that the triple-agonist mechanism does not impose a substantial tolerability burden beyond what is expected with incretin-based therapies.
Overall, the Phase 2 safety data are reassuring but preliminary. Phase 3 trials enrolling thousands of participants over longer treatment durations will be necessary to identify rarer adverse events, characterize long-term safety, and confirm that the benefits observed in Phase 2 are maintained at scale.
Retatrutide in Canada#
Regulatory Status#
As of January 2026, retatrutide has not been approved by Health Canada for any indication. The compound remains investigational, and no New Drug Submission (NDS) has been publicly announced. No timeline for Canadian regulatory filing has been disclosed by Eli Lilly.
Retatrutide is not available through Canadian pharmacies, and it is not covered by any provincial formulary or private insurance plan. Any claims of commercially available retatrutide in Canada should be treated with extreme caution, as the compound is only legitimately accessible through participation in registered clinical trials.
Phase 3 Clinical Trials in Canada#
Canada is an active participant in retatrutide's global Phase 3 clinical trial program. Multiple sites across the country are enrolling participants in trials that will generate the confirmatory data required for regulatory submissions worldwide, including to Health Canada. The major trials with Canadian participation include:
TRIUMPH-1 (NCT05929066) -- This is the pivotal Phase 3 obesity trial evaluating retatrutide in adults with obesity or overweight with weight-related comorbidities. It is the successor to the Phase 2 obesity trial that produced the landmark 24.2% weight loss data and is expected to confirm these results in a larger population over a longer treatment duration.
TRANSCEND-T2D-2 (NCT06260722) -- This Phase 3 trial is particularly noteworthy because it is a head-to-head comparison of retatrutide against semaglutide in adults with type 2 diabetes. Direct comparator trials are the gold standard for establishing therapeutic superiority, and this trial will provide definitive evidence of whether retatrutide's triple-agonist mechanism translates into clinically meaningful advantages over the current standard of care.
TRIUMPH-3 (NCT05882045) -- This cardiovascular outcomes trial evaluates retatrutide's effects on major adverse cardiovascular events (MACE) in patients with established cardiovascular disease or high cardiovascular risk. Cardiovascular outcomes trials are typically required by regulatory agencies for obesity and diabetes therapies, and positive results would substantially strengthen retatrutide's regulatory and clinical positioning.
NCT07357415 -- An additional registered trial contributing to the broader Phase 3 evidence base.
Canadian Trial Sites#
The following Canadian institutions are participating in retatrutide Phase 3 trials:
- University of Calgary (Calgary, Alberta)
- Centricity Research (Brampton, Ontario)
- Hamilton-area clinical sites (Hamilton, Ontario)
- Toronto-area clinical sites (Toronto, Ontario)
- Montreal-area clinical sites (Montreal, Quebec)
- Vancouver-area clinical sites (Vancouver, British Columbia)
- Victoria-area clinical sites (Victoria, British Columbia)
This geographic distribution provides access across multiple provinces, covering major population centers from coast to coast. Canadian residents interested in participating should visit ClinicalTrials.gov and search for "retatrutide" to find actively recruiting sites, or ask their physician to refer them to a participating institution.
What Canadian Patients Should Know#
Several practical considerations are relevant for Canadians following retatrutide's development:
-
Access is trial-only: There is no legal pathway to obtain retatrutide in Canada outside of clinical trial participation. Special Access Programme (SAP) requests to Health Canada are theoretically possible for serious or life-threatening conditions, but retatrutide's investigational status makes SAP access unlikely in practice.
-
Timeline uncertainty: Even if Phase 3 results are positive and a regulatory submission is filed, the Health Canada review process typically takes 12-18 months. Canadians should not expect commercial availability before the regulatory process is complete.
-
Existing alternatives: Semaglutide (Wegovy, approved by Health Canada for chronic weight management) and liraglutide (Saxenda) are currently the approved GLP-1-based obesity therapies in Canada. Tirzepatide (Mounjaro) is approved for type 2 diabetes and has received Health Canada approval for weight management as Zepbound. These represent the current standard of care while retatrutide's development continues.
-
Beware unregulated sources: The high public interest in next-generation weight loss peptides has created a market for unregulated, compounded, or counterfeit products sold online. These products are not verified for purity, potency, or sterility, and purchasing them carries substantial health risks. Retatrutide is not available from legitimate compounding pharmacies in Canada.
How Retatrutide Compares#
Retatrutide vs. Semaglutide#
Semaglutide (Ozempic, Wegovy) is a GLP-1 monoagonist and the current market leader in incretin-based metabolic therapy. The comparison between semaglutide and retatrutide illustrates the incremental benefit of expanding from single- to triple-receptor agonism.
| Parameter | Semaglutide 2.4 mg | Retatrutide 12 mg |
|---|---|---|
| Mechanism | GLP-1 monoagonist | GIP/GLP-1/glucagon triple agonist |
| Half-life | ~7 days | ~6 days |
| Dosing | Once weekly SC | Once weekly SC |
| Weight loss (obesity) | ~15-17% at 68 weeks | 28.7% at 68 weeks (Phase 3 TRIUMPH-4); 24.2% at 48 weeks (Phase 2) |
| HbA1c reduction (T2D) | ~1.8% | Up to 2.02% |
| Liver fat reduction | ~30-40% | Up to 82.4% |
| Regulatory status (Canada) | Approved (Wegovy) | Investigational |
| Phase of development | Marketed | Phase 3 |
The weight loss advantage of retatrutide is substantial: 24.2% at 48 weeks versus approximately 15-17% at 68 weeks for semaglutide. Importantly, retatrutide achieved this at an earlier timepoint, and weight loss curves had not plateaued, suggesting the final difference may be even larger. The TRANSCEND-T2D-2 trial will provide the first direct head-to-head comparison between these compounds.
The liver fat data represent the most dramatic differentiation. Retatrutide's glucagon component drives hepatic fat oxidation directly, producing liver fat reductions approximately double what semaglutide achieves through indirect weight-loss-mediated mechanisms.
Retatrutide vs. Tirzepatide#
Tirzepatide (Mounjaro, Zepbound) is a dual GIP/GLP-1 agonist and retatrutide's most direct comparator, as both compounds share the GIP and GLP-1 receptor targets. The key differentiator is retatrutide's addition of glucagon receptor agonism.
| Parameter | Tirzepatide 15 mg | Retatrutide 12 mg |
|---|---|---|
| Mechanism | GIP/GLP-1 dual agonist | GIP/GLP-1/glucagon triple agonist |
| Half-life | ~5 days | ~6 days |
| Dosing | Once weekly SC | Once weekly SC |
| Weight loss (obesity) | 20.9% at 72 weeks (Phase 3) | 28.7% at 68 weeks (Phase 3 TRIUMPH-4) |
| HbA1c reduction (T2D) | Up to 2.59% | Up to 2.02% |
| Liver fat reduction | ~40-55% | Up to 82.4% |
| Regulatory status (Canada) | Approved (Mounjaro/Zepbound) | Investigational |
| Phase of development | Marketed | Phase 3 |
The weight loss comparison between tirzepatide and retatrutide now has Phase 3 data for both: 20.9% for tirzepatide at 72 weeks versus 28.7% for retatrutide at 68 weeks (TRIUMPH-4). The approximately 8 percentage point advantage for retatrutide is substantial and likely reflects the additional metabolic benefits of glucagon receptor agonism, including increased energy expenditure and hepatic fat catabolism.
Tirzepatide shows a stronger HbA1c reduction (up to 2.59%) than retatrutide (up to 2.02%), potentially reflecting tirzepatide's higher relative GLP-1 potency and the offsetting effect of retatrutide's glucagon component on glucose homeostasis. However, these comparisons are cross-trial and should be interpreted with caution; only direct head-to-head data can provide definitive answers.
The liver fat data again represent retatrutide's clearest differentiation. The glucagon-driven hepatic fat oxidation mechanism produces liver fat reductions (up to 82.4%) that substantially exceed tirzepatide's already impressive results (~40-55%). This positions retatrutide as potentially the strongest pharmacological agent for MASLD/MASH among all incretin-based therapies.
The Broader Competitive Landscape#
Retatrutide enters a rapidly expanding field of metabolic peptide therapeutics. Beyond semaglutide and tirzepatide, other compounds in development include:
- Survodutide (Boehringer Ingelheim): A dual glucagon/GLP-1 agonist showing up to 18.7% weight loss and strong liver fat reduction, positioned particularly for MASH treatment
- CagriSema (Novo Nordisk): A combination of cagrilintide (amylin analog) and semaglutide, targeting an alternative multi-receptor strategy
- Orforglipron (Eli Lilly): An oral non-peptide GLP-1 agonist that could expand access by eliminating the need for injections
The ultimate clinical positioning of retatrutide will depend on Phase 3 efficacy confirmation, long-term safety data, cardiovascular outcomes, pricing, and the practical question of whether the incremental weight loss over tirzepatide justifies a new therapeutic class or whether tirzepatide's established safety record and market presence will be difficult to displace.
Conclusion#
Retatrutide represents the leading edge of multi-receptor metabolic pharmacology. Its triple GIP/GLP-1/glucagon agonist mechanism has produced data that exceed all previously published results for pharmacological weight loss (28.7% at 68 weeks in Phase 3 TRIUMPH-4; 24.2% at 48 weeks in Phase 2), glycemic control in type 2 diabetes (HbA1c reduction of -2.02%), and liver fat reduction in MASLD (up to -82.4%). The addition of glucagon receptor agonism to the established GIP/GLP-1 foundation provides mechanistically distinct benefits -- particularly direct hepatic fat oxidation and increased energy expenditure -- that explain the incremental efficacy over dual-agonist and monoagonist comparators.
For Canadians, the compound is accessible only through Phase 3 clinical trial participation at sites in Calgary, Brampton, Hamilton, Toronto, Montreal, Vancouver, and Victoria. The TRIUMPH-1 obesity trial, TRANSCEND-T2D-2 head-to-head versus semaglutide, and TRIUMPH-3 cardiovascular outcomes trial are the key studies that will determine retatrutide's regulatory future. Health Canada approval, if it occurs, is likely several years away pending completion of these trials and regulatory review.
The transition from Phase 2 to Phase 3 is the most critical juncture in drug development. Phase 2 results, while highly promising, are from smaller patient populations and shorter durations than Phase 3 confirmatory studies. Gastrointestinal tolerability, cardiovascular safety, hepatic enzyme signals, and the durability of weight loss over 52-72 weeks will all require confirmation in larger populations. Patients and clinicians should interpret the current data as strongly encouraging but preliminary.
In the meantime, Canadians seeking pharmacological support for obesity and metabolic disease have access to approved GLP-1 agonists (semaglutide, liraglutide) and the dual GIP/GLP-1 agonist tirzepatide, which represent the current evidence-based standard of care. Retatrutide's Phase 3 results, expected over the next one to two years, will determine whether the triple-agonist approach fulfills its substantial early promise and earns a place in the Canadian therapeutic landscape.
This article reflects data available as of January 2026. Clinical trial results, regulatory decisions, and site availability may change. Consult ClinicalTrials.gov and your healthcare provider for the most current information.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:

{kind=link}
Frequently Asked Questions About Retatrutide Canada Guide
What does this article cover?
Retatrutide in Canada: Everything You Need to Know — part of the Next-Gen Weight Loss content cluster. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Retatrutide. Key context: Retatrutide (Referenced in cluster "Next-Gen Weight Loss"). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Retatrutide Canada Guide." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What is Retatrutide and why is it significant?
Retatrutide is a peptide discussed in this article because: Referenced in cluster "Next-Gen Weight Loss". For a complete profile of Retatrutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

The Evolution of GLP-1 Receptor Agonists: From Single-Target to Multi-Receptor Metabolic Therapeutics
A research review tracing the evolution of GLP-1 receptor agonists from semaglutide through tirzepatide, retatrutide, and survodutide, examining how multi-receptor approaches have progressively expanded efficacy in obesity and metabolic disease.

Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained
A comprehensive guide to every GLP-1 receptor agonist drug, from FDA-approved semaglutide and tirzepatide to pipeline therapies like retatrutide, amycretin, MariTide, and oral orforglipron.

Cagrilintide + Semaglutide (CagriSema): Dual-Agonist Weight Management Research
A comprehensive review of the cagrilintide and semaglutide combination (CagriSema), covering the REDEFINE Phase 3 trial results, dual amylin-GLP-1 mechanisms, weight loss efficacy data, and regulatory status.
You Might Also Like
Related content you may find interesting