Melanotan Tanning Peptides: Risks and Research Evidence

Introduction#
Melanotan peptides are synthetic analogs of alpha-melanocyte-stimulating hormone (alpha-MSH) that stimulate melanin production in the skin, producing a tan without significant UV exposure. Developed originally at the University of Arizona in the 1990s, these peptides have become some of the most widely used non-prescription peptides globally, particularly in countries with strong tanning cultures.
Despite their popularity, Melanotan peptides carry significant documented risks -- particularly regarding mole changes and potential melanoma implications. They are not approved for cosmetic tanning in any country, though a derivative (Melanotan-1 as afamelanotide) has been approved for a specific medical condition.
This article reviews the science behind Melanotan peptides, the documented risks, and what the current evidence shows.
Understanding the Melanocortin System#
Alpha-MSH and Melanin Production#
The melanocortin system is a group of peptide hormones and receptors that regulate diverse biological functions including skin pigmentation, appetite, sexual function, and inflammation.
Alpha-melanocyte-stimulating hormone (alpha-MSH) is the natural peptide that stimulates melanocytes (pigment-producing cells in the skin) to produce melanin. When alpha-MSH binds to the melanocortin-1 receptor (MC1R) on melanocytes, it triggers a signaling cascade that increases melanin synthesis and distribution, darkening the skin.
This is the same process that occurs naturally during sun exposure -- UV radiation stimulates alpha-MSH release, which then activates melanocytes. Melanotan peptides bypass the UV requirement by directly activating the melanocortin receptors.
The Five Melanocortin Receptors#
The melanocortin system has five receptor subtypes, each mediating different effects:
| Receptor | Primary Location | Function | Melanotan Activity |
|---|---|---|---|
| MC1R | Melanocytes (skin) | Melanin production, tanning | Primary target for tanning |
| MC2R | Adrenal cortex | Cortisol production (ACTH receptor) | Minimal activity |
| MC3R | Brain, gut | Energy homeostasis, appetite | Some activity (MT-2) |
| MC4R | Brain (hypothalamus) | Appetite suppression, sexual function | Significant activity (MT-2) |
| MC5R | Sebaceous glands | Sebum production | Some activity |
The distinction between Melanotan-1 and Melanotan-2 lies largely in their receptor selectivity, which determines their side effect profiles.
Melanotan-1 vs. Melanotan-2#
Melanotan-1 (Afamelanotide)#
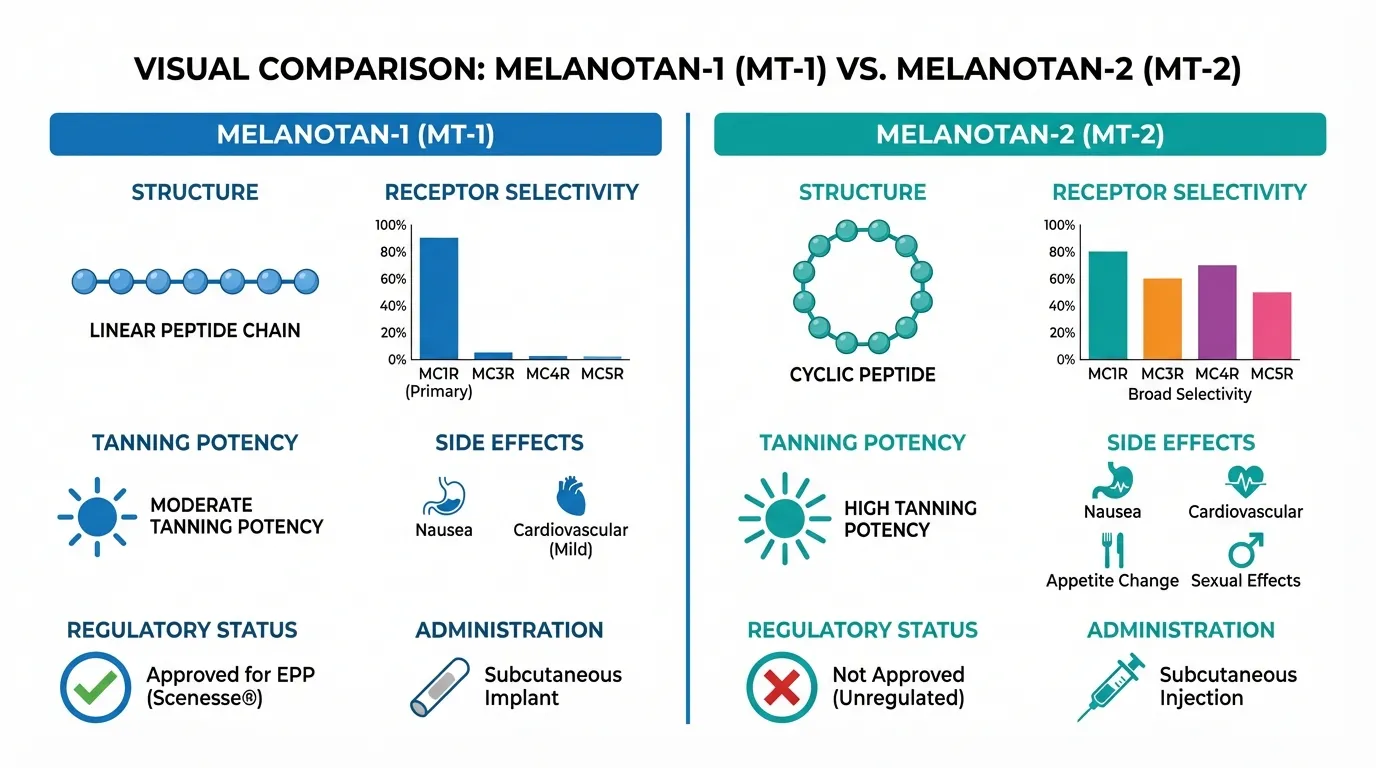
Melanotan-1 is a linear peptide analog of alpha-MSH that is relatively selective for the MC1R receptor.
Key characteristics:
- More selective for MC1R (the pigmentation receptor)
- Fewer off-target effects (less nausea, less sexual stimulation)
- Approved by the EMA (2014) and FDA (October 2019) as Scenesse (afamelanotide) for erythropoietic protoporphyria (EPP), a rare condition causing extreme sun sensitivity
- Administered as a subcutaneous implant (not self-injection)
- Not approved for cosmetic tanning
Melanotan-2#
Melanotan-2 is a cyclic peptide analog of alpha-MSH that activates multiple melanocortin receptors non-selectively.
Key characteristics:
- Activates MC1R (tanning), MC3R (appetite), MC4R (sexual function, appetite), and MC5R
- Produces more pronounced tanning than MT-1
- Causes more side effects due to non-selective receptor activation
- Associated with sexual arousal/erections (MC4R effect)
- Causes appetite suppression (MC3R/MC4R effect)
- Not approved for any indication in any country
- Widely available as a research peptide
Comparison Table#
| Feature | Melanotan-1 | Melanotan-2 |
|---|---|---|
| Structure | Linear, 13 amino acids | Cyclic, 7 amino acids |
| MC1R selectivity | Relatively selective | Non-selective |
| Tanning potency | Moderate | High |
| Nausea | Mild | Moderate to severe initially |
| Sexual effects | Minimal | Pronounced (MC4R activation) |
| Appetite effects | Minimal | Appetite suppression |
| Facial flushing | Mild | Common |
| Regulatory status | EMA- and FDA-approved (Scenesse) for EPP | Not approved anywhere |
| Route | Subcutaneous implant (approved form) | Subcutaneous injection (unapproved) |
Documented Risks#
Mole Changes: The Primary Safety Concern#
The most clinically significant risk associated with Melanotan peptides is changes to existing moles (nevi). This is well-documented in the medical literature:
What happens:
- Existing moles can darken significantly
- Moles may increase in size
- New moles can appear
- Irregular or atypical features may develop in previously normal moles
- The changes are often widespread (not limited to sun-exposed areas)
Why it matters: Changes in mole size, shape, color, or symmetry are the primary screening criteria for melanoma. Melanotan-induced mole changes can:
- Mask early melanoma detection: When all moles are changing, it becomes harder to identify which changes are Melanotan-induced and which might represent early melanoma
- Trigger unnecessary biopsies: Dermatologists may recommend biopsies of Melanotan-altered moles, leading to procedures that would otherwise be unnecessary
- Potentially promote melanocyte proliferation: While not proven, the stimulation of melanocyte activity raises theoretical concerns about promoting melanocyte-related cancers
The Melanoma Question#
Does Melanotan cause melanoma? The current evidence does not definitively prove a causal relationship, but several factors warrant serious concern:
Evidence suggesting risk:
- Multiple published case reports of melanoma diagnosed in Melanotan users
- Melanotan stimulates melanocyte proliferation and melanin production -- the same cells and processes involved in melanoma
- MC1R signaling is involved in both melanogenesis and melanocyte survival pathways
- Users with fair skin (the demographic most attracted to tanning peptides) already have the highest baseline melanoma risk
Evidence against a definitive link:
- Case reports cannot establish causation -- Melanotan users also typically use UV tanning, which is a known melanoma risk factor
- No large epidemiological studies have been conducted
- Millions of doses have been used globally with a relatively small number of case reports
- The afamelanotide (MT-1) clinical trial program did not show increased melanoma rates, though the patient population and duration of exposure differ from typical MT-2 use
Bottom line: The absence of proof of causation is not the same as evidence of safety. Given the biological plausibility of the risk and the inability to conduct definitive studies, melanoma risk remains a genuine concern with Melanotan use.
Cardiovascular Effects#
Melanocortin receptors are expressed in the cardiovascular system. Documented effects include:
- Blood pressure changes: Both hypertension and hypotension have been reported
- Facial flushing: Vasodilation causing redness and warmth
- Heart rate changes: Palpitations reported by some users
These effects are generally mild and transient, but individuals with pre-existing cardiovascular conditions should be particularly cautious.
Gastrointestinal Effects#
- Nausea: The most commonly reported side effect, particularly with initial doses of MT-2
- Appetite suppression: Due to MC3R/MC4R activation; may be unwanted
- Abdominal cramping: Reported occasionally
Sexual Effects#
MC4R activation by Melanotan-2 can produce:
- Spontaneous erections in males (common and can occur at inconvenient times)
- Increased libido in both sexes
- Priapism: Prolonged, painful erection; rare but a medical emergency
The sexual effects were actually the pathway through which PT-141 (bremelanotide) was developed as an FDA-approved treatment for hypoactive sexual desire disorder in women. PT-141 is a metabolite of Melanotan-2 that was optimized for MC4R activity.
Other Documented Side Effects#
| Side Effect | Frequency | Notes |
|---|---|---|
| Fatigue and lethargy | Common | Often reported after injection |
| Yawning and stretching | Occasional | Unusual but documented melanocortin effect |
| Dizziness | Occasional | May relate to blood pressure effects |
| Injection site reactions | Common | Standard for any injectable |
| Darkening of existing scars | Occasional | Melanocytes in scar tissue respond |
| Periorbital darkening | Occasional | Dark circles under eyes |
Populations at Higher Risk#
Certain groups should be particularly cautious or should avoid Melanotan peptides entirely:
| Population | Concern |
|---|---|
| Personal or family history of melanoma | Stimulating melanocyte activity could promote tumor growth |
| History of atypical moles or dysplastic nevi | Higher baseline melanoma risk |
| Very fair skin (Fitzpatrick type I) | Highest melanoma susceptibility |
| Cardiovascular disease | Blood pressure and heart rate effects |
| Pregnancy or breastfeeding | No safety data |
| Children and adolescents | No safety data; developing melanocytes may be more susceptible |
Regulatory Status#
Melanotan-2 is not approved for human use in any country. Regulatory agencies worldwide have issued warnings:
- FDA (USA): Warning against use of Melanotan products
- TGA (Australia): Multiple warnings; Melanotan products seized
- EMA (Europe): No approval for cosmetic use
- MHRA (UK): Warnings against unlicensed Melanotan products
Melanotan-1 (as afamelanotide/Scenesse) is approved by the EMA and FDA only for erythropoietic protoporphyria (EPP) -- a rare genetic condition -- not for cosmetic tanning.
For broader regulatory context, see our FDA regulation guide.
UV Exposure and Melanotan#
An important consideration: Melanotan does not eliminate the need for UV exposure. Most users still use some UV exposure (sun or tanning beds) alongside Melanotan to activate the melanin that Melanotan stimulates melanocytes to produce.
This means that Melanotan users often combine two risk factors for skin cancer: melanocortin stimulation of melanocytes plus UV radiation damage to DNA. The claim that Melanotan is "safer than tanning" because it reduces UV exposure needed is not substantiated by any clinical study.
Harm Reduction Considerations#
For those who choose to use Melanotan peptides despite the risks, the following harm reduction approaches are commonly discussed:
- Regular dermatological monitoring: Full-body skin checks at least annually, more frequently if mole changes are noticed
- Baseline mole mapping: Photograph all moles before starting to enable comparison
- Self-monitoring: Regular self-examination using the ABCDE criteria (Asymmetry, Border irregularity, Color variation, Diameter >6mm, Evolution/change)
- Minimize UV exposure: The less UV exposure combined with Melanotan, the lower the combined skin cancer risk
- Quality considerations: Research peptide quality varies; see our quality guide
- Start with low doses: To assess individual tolerance before increasing
Key Takeaways#
-
Melanotan peptides produce tanning by directly activating melanocortin receptors, bypassing the normal UV-mediated pathway. Melanotan-2 is non-selective, causing side effects beyond tanning.
-
Mole changes are the primary safety concern. Existing moles can darken, new moles can appear, and these changes can complicate melanoma screening.
-
A causal link between Melanotan and melanoma has not been proven, but the biological plausibility is concerning. Multiple case reports and the mechanism of action warrant serious caution.
-
Melanotan-2 is not approved for human use in any country. Only Melanotan-1 (as afamelanotide) is approved, and only for the rare condition EPP.
-
Melanotan does not eliminate UV exposure needs or skin cancer risk. Most users still use UV alongside Melanotan, combining two risk factors.
-
Fair-skinned individuals are both the most attracted to Melanotan and the most vulnerable to its potential risks, creating an inherent tension between the cosmetic benefit and the safety concern.
For a direct comparison, see Melanotan-1 vs Melanotan-2 and Melanotan-2 vs PT-141. To compare half-lives of melanocortin peptides, use the half-life comparison tool.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:

{kind=link}
Frequently Asked Questions About Melanotan Tanning Peptides: Risks and Research Evidence
What does this article cover?
Melanotan-1 and Melanotan-2 tanning peptide review — how they work, documented risks including mole changes, side effects, and legal status. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Melanotan-2, Melanotan-1, PT-141. Key context: Melanotan-2 (The most widely used tanning peptide, with documented risks including mole changes, nausea, and m...); Melanotan-1 (The more selective melanocortin agonist approved in some countries as afamelanotide for erythropo...); PT-141 (Derived from Melanotan-2, illustrating how melanocortin peptides can be developed toward specific...). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: The most widely used tanning peptide, with documented risks including mole changes, nausea, and m.... The more selective melanocortin agonist approved in some countries as afamelanotide for erythropo.... Derived from Melanotan-2, illustrating how melanocortin peptides can be developed toward specific.... These takeaways are based on the research data available at the time of publication.
What is Melanotan-2 and why is it significant?
Melanotan-2 is a peptide discussed in this article because: The most widely used tanning peptide, with documented risks including mole changes, nausea, and melanocortin-mediated side effects. For a complete profile of Melanotan-2, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Peptides for Sexual Health: PT-141, Kisspeptin, and Beyond
Peptides for sexual health — PT-141, kisspeptin, Melanotan-2, and oxytocin — covering mechanisms, clinical evidence, and safety data.

8 Peptides for Skin Health and Rejuvenation: Research Guide
Peptides for skin health — GHK-Cu, SNAP-8, Melanotan-1, BPC-157, and Glutathione reviewed with evidence levels and mechanisms of action.

Reproductive Health Peptides: A Research Roundup
Peptides for reproductive health — kisspeptin, gonadorelin, HCG, HMG, triptorelin, and PT-141 — with evidence levels and clinical status.
You Might Also Like
Related content you may find interesting