IGF-1 Peptides: LR3, DES, and MGF — Variants and Research Overview

Introduction#
Insulin-like growth factor 1 (IGF-1) is the primary mediator of growth hormone's anabolic effects in peripheral tissues. When GH is released from the pituitary and reaches the liver, it stimulates the production and secretion of IGF-1 into the bloodstream. This endocrine IGF-1 then acts on tissues throughout the body — driving cell proliferation, protein synthesis, and metabolic regulation through the IGF-1 receptor (IGF-1R).
But the IGF-1 system is far more complex than a single peptide. The IGF-1 gene undergoes alternative splicing to produce multiple variants with different tissue distributions, binding protein affinities, and biological activities. Researchers have developed synthetic analogs of these variants — including IGF-1 LR3, IGF-1 DES, MGF, and PEG-MGF — to exploit specific aspects of IGF-1 signaling.
This article reviews the major IGF-1 variant peptides, their mechanisms, and the current state of preclinical and clinical evidence for each.
The GH-IGF-1 Axis: Upstream Context#
Understanding IGF-1 variants requires understanding the axis that produces them.
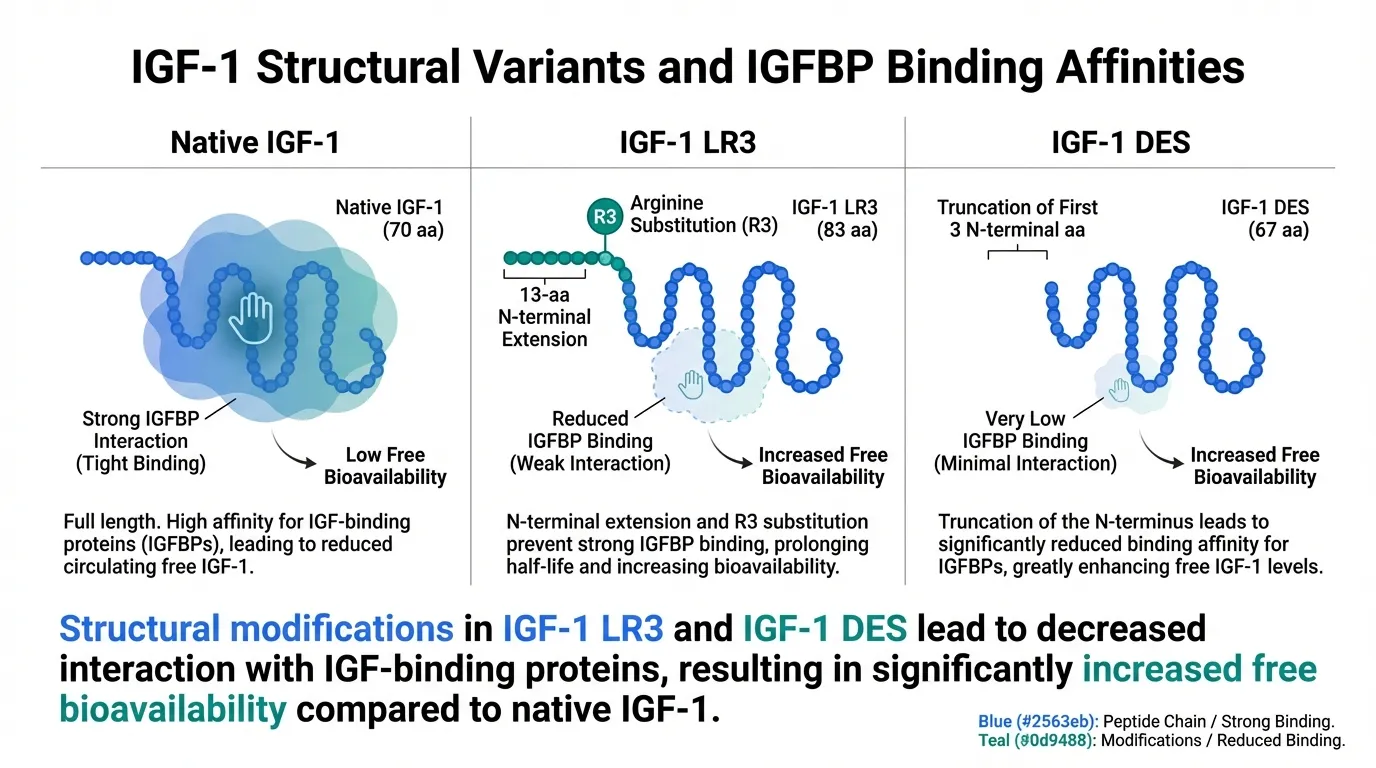
Growth hormone, released from the anterior pituitary in a pulsatile pattern, circulates to the liver where it binds to the GH receptor (GHR). This activates the JAK2-STAT5b signaling pathway, driving transcription of the IGF-1 gene. The resulting IGF-1 protein (a 70-amino acid polypeptide) is secreted into the bloodstream, where approximately 98% circulates bound to one of six IGF-binding proteins (IGFBPs), primarily IGFBP-3 in complex with the acid-labile subunit (ALS).
This binding protein system serves as a reservoir, extending IGF-1's circulating half-life from minutes (free IGF-1) to approximately 12-16 hours (bound in the ternary complex). IGFBPs also regulate IGF-1 bioavailability — only free IGF-1 can bind to the IGF-1R and activate downstream signaling.
The synthetic IGF-1 variants were designed to manipulate this binding protein relationship. Each variant alters the interaction with IGFBPs in a different way, fundamentally changing the peptide's bioavailability, potency, and tissue distribution.
In addition to endocrine (liver-derived) IGF-1, local tissues — particularly skeletal muscle — produce their own IGF-1 through autocrine and paracrine signaling. This locally produced IGF-1 does not depend on circulating GH levels and includes tissue-specific splice variants like MGF. Exogenous HGH 191aa drives endocrine IGF-1 production, while local mechanical and metabolic signals drive tissue-specific variants.
IGF-1 LR3: The Long-Acting Variant#
Structure and Mechanism#
IGF-1 LR3 (Long R3 IGF-1) is a synthetic analog of human IGF-1 containing 83 amino acids compared to the native 70. It differs from endogenous IGF-1 in two ways:
- Arginine substitution at position 3 — The glutamic acid at position 3 of native IGF-1 is replaced with arginine (hence "R3")
- N-terminal extension — A 13-amino acid peptide is added to the N-terminus (hence "Long")
These modifications dramatically reduce IGF-1 LR3's affinity for IGF-binding proteins. While native IGF-1 is approximately 98% bound to IGFBPs in circulation, IGF-1 LR3 remains largely unbound and therefore bioavailable. The result is a form of IGF-1 that is functionally more potent on a per-molecule basis — not because it binds the IGF-1R more strongly, but because a much higher proportion of each administered dose is free to interact with the receptor.
The half-life of IGF-1 LR3 is estimated at 20-30 hours in preclinical models, compared to approximately 12-16 minutes for free (unbound) native IGF-1. This extended half-life is paradoxical: despite not binding to the protective IGFBP complex, IGF-1 LR3's structural modifications also reduce its susceptibility to proteolytic degradation.
Research Evidence#
IGF-1 LR3 has been studied extensively in cell culture and animal models:
- Cell proliferation studies: IGF-1 LR3 is widely used as a media supplement in cell culture, where its low IGFBP affinity makes it more consistently bioavailable than native IGF-1. It promotes proliferation of multiple cell types including myoblasts, fibroblasts, and epithelial cells.
- Animal growth studies: Administration of IGF-1 LR3 in animal models produces anabolic effects including increased body weight, organ growth, and nitrogen retention. Studies in rodents have demonstrated effects on skeletal muscle hypertrophy when administered systemically.
- Metabolic effects: Like native IGF-1, LR3 has insulin-like metabolic effects including glucose uptake stimulation. The risk of hypoglycemia is a significant safety concern in preclinical studies.
Limitations#
IGF-1 LR3 has no published human clinical trials. Its evidence base is entirely preclinical and in vitro. The peptide's increased potency relative to native IGF-1 (due to IGFBP evasion) also means it carries greater risk of IGF-1R-mediated side effects, including hypoglycemia and potential mitogenic effects. The long-term safety profile in any species is poorly characterized. IGF-1 LR3 is not approved for any clinical use and remains an investigational research compound.
IGF-1 DES: The Truncated Potent Variant#
Structure and Mechanism#
IGF-1 DES (des(1-3) IGF-1) is a naturally occurring truncated form of IGF-1 lacking the first three N-terminal amino acids (Gly-Pro-Glu). This N-terminal tripeptide is cleaved from circulating IGF-1 by proteases in various tissues, particularly in the brain, where IGF-1 DES was first isolated.
The removal of these three amino acids has two significant consequences:
- Dramatically reduced IGFBP binding — The N-terminal region of IGF-1 is critical for IGFBP interaction. Without it, IGF-1 DES has approximately 100-fold lower affinity for IGFBP-3. Like IGF-1 LR3, this means a higher proportion remains free and bioavailable.
- Preserved or enhanced IGF-1R affinity — Despite the truncation, IGF-1 DES retains full binding affinity for the IGF-1 receptor. Some in vitro studies suggest it may have modestly enhanced receptor activation compared to native IGF-1, possibly due to the absence of IGFBP-mediated sequestration at the receptor surface.
The result is a variant that is approximately 10-fold more potent than native IGF-1 in standard cell proliferation assays — again, primarily due to its IGFBP evasion rather than enhanced intrinsic receptor affinity.
Unlike IGF-1 LR3, IGF-1 DES has a very short half-life (estimated at 20-30 minutes), as the loss of IGFBP binding removes the protective reservoir effect without the structural modifications that extend LR3's duration. This makes IGF-1 DES a rapidly acting but short-duration variant.
Research Evidence#
- Brain tissue: IGF-1 DES was originally characterized in brain extracts, where it is thought to be produced locally by protease cleavage of full-length IGF-1. Research has explored its neurotrophic and neuroprotective properties in cell culture and animal models.
- Cell culture: Widely studied in proliferation assays. IGF-1 DES consistently shows higher mitogenic potency than equimolar native IGF-1 in cells expressing IGF-1R.
- Wound healing: Preclinical studies have examined topical and local IGF-1 DES administration for wound healing, where its local potency and short half-life create a transient but intense IGF-1R signal.
- Muscle research: Animal studies have examined local IGF-1 DES administration for muscle hypertrophy, particularly in comparison to systemic IGF-1 approaches.
Limitations#
Like IGF-1 LR3, IGF-1 DES has no human clinical trial data. Its extremely short half-life requires frequent administration for any sustained effect. The enhanced mitogenic potency raises theoretical concerns about proliferative effects, though these have not been systematically evaluated in long-term studies. It remains a research-only compound.
MGF: The Muscle-Specific Splice Variant#
Structure and Mechanism#
Mechano growth factor (MGF) is a splice variant of the IGF-1 gene that is expressed specifically in skeletal muscle in response to mechanical loading (exercise, stretch, or damage). It is encoded by exons 4, 5, and 6 of the IGF-1 gene, with exon 5 (also called the Eb domain in rodents or Ec domain in humans) providing the unique C-terminal peptide that distinguishes MGF from systemic IGF-1 isoforms.
The MGF peptide differs from endocrine IGF-1 in a critical way: it acts locally within muscle tissue through autocrine and paracrine signaling rather than entering systemic circulation. Its primary biological role appears to be the activation of satellite cells — the resident stem cells of skeletal muscle that are essential for muscle repair and hypertrophy.
The proposed mechanism involves:
- Mechanical damage or loading triggers MGF gene expression in the stretched or damaged muscle fibers
- MGF peptide is released locally and acts on nearby satellite cells
- Satellite cell activation — MGF promotes satellite cell proliferation (expanding the pool of repair-competent cells) without immediately driving their differentiation into mature myofibers
- Subsequent IGF-1Ea expression — After the initial MGF pulse, the same muscle tissue shifts to producing the IGF-1Ea isoform (systemic-type IGF-1), which drives satellite cell differentiation and fusion into existing or new muscle fibers
This temporal sequence — MGF first (proliferation), then IGF-1Ea (differentiation) — represents an elegant biological program for muscle repair. MGF expands the progenitor cell pool, and IGF-1Ea then directs those cells to become functional muscle tissue.
Research Evidence#
MGF has been studied primarily in preclinical and in vitro models:
- Satellite cell activation: Cell culture studies have demonstrated that MGF promotes the proliferation of C2C12 myoblasts (a mouse muscle cell line) and primary human satellite cells without inducing premature differentiation. This is consistent with its proposed role as an early-phase repair signal.
- Mechanical loading models: Animal studies have shown that MGF mRNA expression increases rapidly (within hours) after resistance exercise or muscle damage, peaking before the systemic IGF-1Ea isoform. This temporal pattern supports the sequential activation model.
- Cardiac muscle: Research has explored MGF's role in cardiac tissue, where it is also expressed after mechanical stress. Studies in rodent models of myocardial infarction have suggested cardioprotective effects, including reduced apoptosis and improved functional recovery.
- Age-related decline: Studies have documented that MGF expression in response to exercise declines with age in both rodent and human muscle biopsies, suggesting that impaired MGF signaling may contribute to the age-related decline in muscle regenerative capacity (sarcopenia).
The Synthetic MGF Peptide#
The synthetic MGF peptide used in research typically consists of the 24-amino acid C-terminal Ec domain peptide that distinguishes MGF from other IGF-1 splice variants. This peptide has a very short half-life in circulation — estimated at only a few minutes — because it lacks the structural features that protect full-length IGF-1 from degradation.
This rapid degradation is not necessarily a limitation in the physiological context, where MGF acts locally within muscle tissue. However, it presents a challenge for research protocols involving systemic administration, as the peptide is largely degraded before reaching target tissues. This limitation led to the development of PEG-MGF.
PEG-MGF: Extended-Duration Mechano Growth Factor#
Structure and Mechanism#
PEG-MGF is the pegylated form of MGF — the same C-terminal Ec domain peptide conjugated to a polyethylene glycol (PEG) chain. Pegylation is a well-established pharmaceutical strategy for extending peptide half-life by:
- Increasing molecular size — The PEG chain increases the hydrodynamic radius, reducing renal clearance
- Steric shielding — The PEG moiety physically shields the peptide from proteolytic enzymes
- Reducing immunogenicity — PEG conjugation can mask immunogenic epitopes
The result is a form of MGF with a significantly extended circulating half-life — estimated at several hours compared to minutes for unmodified MGF. This allows systemic administration to produce meaningful tissue exposure.
Research Evidence#
PEG-MGF has been studied primarily in animal models:
- Systemic bioavailability: Studies comparing PEG-MGF to unmodified MGF have confirmed significantly higher and more sustained plasma levels after subcutaneous or intramuscular injection.
- Muscle hypertrophy: Animal studies have examined PEG-MGF's effects on muscle growth. Intramuscular injection of PEG-MGF in rodent models has produced localized hypertrophy in the injected muscle, consistent with enhanced satellite cell activation.
- Cardiac repair: Preclinical cardiac studies have explored PEG-MGF as a potential cardioprotective agent following myocardial infarction, leveraging MGF's anti-apoptotic properties with improved delivery pharmacokinetics.
The PEG Trade-Off#
While pegylation solves the half-life problem, it introduces a pharmacological trade-off. Native MGF's extremely short half-life is part of its physiological role — it acts as a brief, local signal within muscle tissue. By extending its duration and enabling systemic distribution, PEG-MGF fundamentally changes the signaling dynamics. Whether this extended, systemic exposure replicates or improves upon the brief, local MGF pulse remains an open research question.
Comparing IGF-1 Variants#
| Feature | Native IGF-1 | IGF-1 LR3 | IGF-1 DES | MGF | PEG-MGF |
|---|---|---|---|---|---|
| Amino acids | 70 | 83 | 67 | 24 (Ec domain) | 24 + PEG |
| IGFBP binding | High (98% bound) | Very low | Very low | N/A | N/A |
| IGF-1R affinity | Reference | Similar | Similar or slightly enhanced | Distinct mechanism | Distinct mechanism |
| Half-life | 12-16 hrs (bound) / ~15 min (free) | ~20-30 hrs | ~20-30 min | Minutes | Hours |
| Primary action | Systemic anabolic | Systemic anabolic (enhanced) | Local/rapid anabolic | Satellite cell activation | Satellite cell activation (extended) |
| Human clinical data | Yes (recombinant IGF-1) | No | No | No | No |
| Tissue specificity | Systemic | Systemic | Variable | Muscle-specific | Modified muscle-specific |
The Evidence Gap: Preclinical vs Clinical#
A critical point for evaluating these peptides is the significant gap between preclinical evidence and clinical validation. While native IGF-1 (as recombinant mecasermin, brand name Increlex) has been FDA-approved for the treatment of severe primary IGF-1 deficiency, none of the variant peptides discussed in this article have undergone rigorous human clinical trials.
The preclinical evidence base for IGF-1 LR3, IGF-1 DES, MGF, and PEG-MGF consists primarily of:
- Cell culture proliferation and differentiation assays
- Rodent models of muscle hypertrophy, injury, and repair
- Rodent models of cardiac injury and repair
- Pharmacokinetic studies in animal models
These studies provide mechanistic insight and proof-of-concept evidence, but they do not establish safety or efficacy in humans. Cell culture conditions differ dramatically from in vivo physiology, and peptide pharmacokinetics in rodents do not directly translate to humans. The absence of dose-finding studies, pharmacokinetic characterization, and controlled efficacy trials in human subjects means that the therapeutic potential of these variants remains speculative.
Safety Considerations#
Shared Concerns Across IGF-1 Variants#
All IGF-1-related peptides carry theoretical safety concerns related to IGF-1R signaling:
- Hypoglycemia — IGF-1 activates the insulin receptor (with lower affinity than insulin) and enhances insulin sensitivity. The IGFBP-evading variants (LR3 and DES) may carry elevated hypoglycemia risk due to their higher effective bioavailability.
- Mitogenic potential — IGF-1R signaling is mitogenic (promotes cell division). Epidemiological studies have associated elevated circulating IGF-1 levels with increased risk of certain cancers, though causality is debated. Variants with enhanced bioavailability or potency could theoretically amplify this concern.
- Organ growth — Systemic IGF-1R activation can promote growth of multiple organ systems. Preclinical studies with IGF-1 LR3 have demonstrated organomegaly at higher doses.
- Interaction with GH axis — Exogenous IGF-1 administration suppresses endogenous GH secretion through negative feedback at the hypothalamus and pituitary. This is relevant for protocols combining IGF-1 variants with GH secretagogues.
Variant-Specific Considerations#
- IGF-1 LR3: Extended half-life means prolonged exposure and more sustained IGF-1R activation, potentially amplifying both desired and undesired effects
- IGF-1 DES: Short half-life limits systemic exposure but the enhanced per-molecule potency creates intensity concerns during the active window
- MGF/PEG-MGF: These act through mechanisms partially distinct from canonical IGF-1R signaling (satellite cell activation), but the long-term effects of exogenous satellite cell stimulation are unknown
Relationship to GH Secretagogues#
IGF-1 variant peptides occupy a fundamentally different position in the GH axis compared to GH secretagogues like Sermorelin, CJC-1295, Ipamorelin, or GHRP-6. Secretagogues act upstream — stimulating the pituitary to release GH, which then drives endogenous IGF-1 production through the natural axis. IGF-1 variants act downstream — bypassing GH entirely to deliver IGF-1-like signaling directly to target tissues.
This distinction matters for several reasons. GH secretagogues preserve the body's feedback systems: the pituitary controls how much GH is released, and the liver modulates how much IGF-1 is produced. IGF-1 variants bypass these regulatory checkpoints. HGH 191aa sits in between — it bypasses pituitary regulation but still relies on the liver's IGF-1 production machinery.
For researchers interested in the GH-IGF-1 axis, the choice between upstream (secretagogue) and downstream (IGF-1 variant) approaches depends on whether the goal is to enhance the entire axis physiologically or to deliver targeted IGF-1R signaling to specific tissues.
Conclusion#
The IGF-1 variant peptides — IGF-1 LR3, IGF-1 DES, MGF, and PEG-MGF — represent different strategies for modifying IGF-1 signaling. LR3 and DES evade binding proteins to increase bioavailability. MGF and PEG-MGF target the muscle satellite cell activation pathway specifically. Each has a distinct pharmacokinetic profile and proposed mechanism, but all share the critical limitation of minimal or absent human clinical data.
The mechanistic rationale for these variants is scientifically sound — IGFBP evasion, tissue-specific splice variant signaling, and pegylation for half-life extension are well-established pharmacological strategies. However, mechanistic rationale alone does not establish clinical utility or safety. Researchers evaluating these peptides should weigh the preclinical evidence carefully against the absence of controlled human studies and the inherent safety concerns of enhanced IGF-1R signaling.
For broader context on growth hormone peptides and the upstream signals that drive IGF-1 production, see our GHRH vs GHRP guide and the Growth Hormone Secretagogues Compared overview.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:

{kind=link}
Frequently Asked Questions About IGF-1 Peptides: LR3, DES, and MGF — Variants and Research Overview
What does this article cover?
Research overview of IGF-1 variant peptides — IGF-1 LR3, IGF-1 DES, MGF, and PEG-MGF — covering mechanisms, the GH-IGF-1 axis, and preclinical evidence. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers HGH 191aa, MGF, PEG-MGF. Key context: HGH 191aa (Recombinant human growth hormone that drives IGF-1 production through the GH-IGF-1 axis, the upst...); MGF (Mechano growth factor, a splice variant of IGF-1 produced locally in muscle tissue in response to...); PEG-MGF (Pegylated version of MGF with extended half-life designed to enhance systemic stability of the me...). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: Recombinant human growth hormone that drives IGF-1 production through the GH-IGF-1 axis, the upst.... Mechano growth factor, a splice variant of IGF-1 produced locally in muscle tissue in response to.... Pegylated version of MGF with extended half-life designed to enhance systemic stability of the me.... These takeaways are based on the research data available at the time of publication.
What is HGH 191aa and why is it significant?
HGH 191aa is a peptide discussed in this article because: Recombinant human growth hormone that drives IGF-1 production through the GH-IGF-1 axis, the upstream signal for all IGF-1 variants. For a complete profile of HGH 191aa, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Top 10 Peptides for Muscle Recovery and Growth: Evidence-Based Research Guide
The 10 most studied peptides for muscle recovery and growth, including BPC-157, TB-500, IGF-1 LR3, ipamorelin, and follistatin, with mechanisms, evidence levels, and key research data.
Best Growth Hormone Peptides Ranked: 2026 Evidence-Based Guide
A ranked comparison of 8 growth hormone secretagogues and related peptides — from FDA-approved tesamorelin to IGF-1 LR3 — evaluating each on mechanism of action, clinical evidence strength, key advantages, and known drawbacks.

The Science of Peptide-Enhanced Muscle Recovery: From GH Secretagogues to BPC-157
Research review of peptides for muscle recovery including BPC-157, TB-500, ipamorelin, sermorelin, and MGF with mechanisms, evidence levels, and clinical data analysis.
You Might Also Like
Related content you may find interesting