Human Equivalent Dose (HED): How to Convert Animal Study Doses

Introduction#
Many peptides discussed in research communities have only been studied in animals. When human clinical trials have not been conducted, animal study doses are often the only reference point available. But translating a dose from a mouse or rat to a human is not as simple as adjusting for body weight.
The human equivalent dose (HED) is the estimated dose in humans that corresponds to a dose shown to be effective or safe in an animal species. The FDA provides guidance on this calculation using body surface area (BSA) scaling, which accounts for the fact that metabolic rate and drug clearance scale more closely with body surface area than with body weight alone.
This article explains the HED calculation, why it matters, the assumptions behind it, and the important limitations that are often overlooked.
For a quick calculation, use our HED calculator tool. For general peptide dosing information, see our peptide dosing guide.
Why Simple Weight-Based Scaling Is Wrong#
The most common mistake in dose conversion is simple linear scaling by body weight. For example, if a study uses 10 mcg/kg in a 0.025 kg mouse, one might calculate the human dose as simply 10 mcg/kg x 70 kg = 700 mcg for a 70 kg human.
This overestimates the correct dose by approximately 12-fold.
The reason: smaller animals have higher metabolic rates per unit of body weight than larger animals. A mouse's metabolic rate (per gram of body weight) is approximately 7 times higher than a human's. This means a mouse clears drugs faster and requires a proportionally higher dose per kilogram to achieve the same drug exposure.
| Species | Body Weight (kg) | Metabolic Rate Relative to Human |
|---|---|---|
| Mouse | 0.02-0.03 | ~7x higher per kg |
| Rat | 0.15-0.30 | ~4x higher per kg |
| Rabbit | 1.8-4.0 | ~2.5x higher per kg |
| Dog | 8-15 | ~1.5x higher per kg |
| Human | 60-80 | 1x (reference) |
Because of this metabolic scaling relationship, a dose of 10 mg/kg in a mouse does not correspond to 10 mg/kg in a human. It corresponds to a much lower dose in humans.
The FDA HED Formula#
The FDA's guidance document "Estimating the Maximum Safe Starting Dose in Initial Clinical Trials for Therapeutics in Adult Healthy Volunteers" (2005) provides the standard method for dose conversion between species.
The Basic Formula#
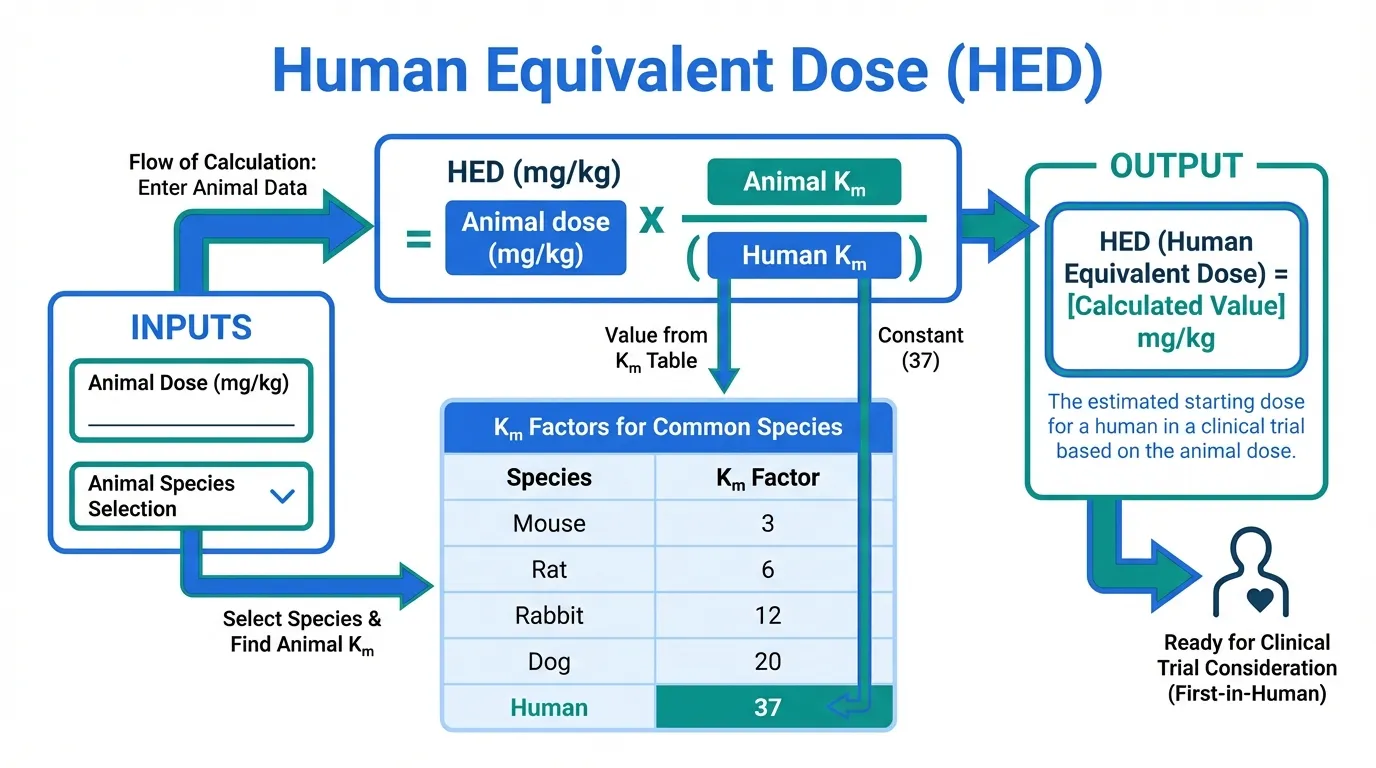
HED (mg/kg) = Animal dose (mg/kg) x (Animal K_m / Human K_m)
Where K_m is a correction factor based on body surface area. The K_m value for each species is:
| Species | Reference Weight (kg) | K_m Factor |
|---|---|---|
| Mouse | 0.02 | 3 |
| Hamster | 0.08 | 5 |
| Rat | 0.15 | 6 |
| Ferret | 0.30 | 7 |
| Guinea pig | 0.40 | 8 |
| Rabbit | 1.8 | 12 |
| Monkey | 3.0 | 12 |
| Dog | 10 | 20 |
| Human | 60 | 37 |
Practical Conversion Factors#
For quick calculations, the ratio of Animal K_m to Human K_m gives a direct conversion multiplier:
| Species | Multiply Animal Dose (mg/kg) by: | To Get HED (mg/kg) |
|---|---|---|
| Mouse | 0.081 (3/37) | For a 60 kg human |
| Rat | 0.162 (6/37) | For a 60 kg human |
| Rabbit | 0.324 (12/37) | For a 60 kg human |
| Dog | 0.541 (20/37) | For a 60 kg human |
| Monkey | 0.324 (12/37) | For a 60 kg human |
Worked Example: BPC-157#
A commonly cited BPC-157 study uses a dose of 10 mcg/kg in rats for tendon healing.
Step 1: Apply the rat conversion factor
HED = 10 mcg/kg x (6/37) = 10 x 0.162 = 1.62 mcg/kg
Step 2: Calculate for a 70 kg human
Total dose = 1.62 mcg/kg x 70 kg = 113 mcg (approximately 110-115 mcg)
This is substantially lower than the simple weight-based calculation of 700 mcg (10 mcg/kg x 70 kg). The BSA-corrected dose is roughly 6 times lower for rat-to-human conversion.
Another Example: Mouse Study Conversion#
If a mouse study uses 50 mcg/kg:
HED = 50 mcg/kg x (3/37) = 50 x 0.081 = 4.05 mcg/kg
For a 70 kg human: 4.05 x 70 = 284 mcg
The simple weight-based calculation would give 3,500 mcg (50 x 70) -- more than 12 times higher.
Important Limitations#
The HED Is a Starting Point, Not a Dose Recommendation#
The HED calculation is designed to estimate a maximum safe starting dose for first-in-human clinical trials. It is not designed to predict the therapeutically effective dose in humans. The actual effective dose in humans may be higher, lower, or the same as the HED.
In pharmaceutical development, the HED provides the starting point for Phase 1 dose-escalation studies that then systematically determine the safe and effective dose range in humans.
BSA Scaling Has Known Limitations#
The BSA method makes several assumptions that may not hold for all compounds:
| Assumption | Reality |
|---|---|
| Drug clearance scales with BSA | True for many but not all drugs |
| Pharmacokinetics are similar across species | Often significantly different |
| Receptor density and sensitivity are comparable | Can vary greatly between species |
| Route of administration is the same | Different routes have different bioavailability |
| Linear pharmacokinetics | Many peptides have non-linear PK |
For some peptides, the actual human effective dose may differ substantially from the BSA-calculated HED because of species-specific differences in receptor expression, binding affinity, or metabolic pathways.
Peptide-Specific Considerations#
Peptides present additional challenges for HED calculations:
Short half-lives: Many peptides are rapidly degraded. If a peptide is cleared faster in one species than another, the HED based on BSA alone may not accurately predict exposure.
Route-dependent bioavailability: A peptide given intraperitoneally in a mouse study (a common route in animal research) will have different bioavailability than the same peptide given subcutaneously in humans.
Receptor differences: The affinity of a peptide for its target receptor may differ between species. A dose that saturates the receptor in a mouse may not produce the same receptor occupancy in a human.
Local vs. systemic effects: For peptides like BPC-157 that are often injected locally near an injury, the local tissue concentration may matter more than the systemic dose, making whole-body HED calculations less relevant.
When HED Is Not Available: What Peptide Communities Actually Do#
For many research peptides, the community-used doses are not derived from formal HED calculations. Instead, they often come from:
- Direct weight-based scaling from animal studies (often resulting in higher-than-HED doses)
- Anecdotal titration -- users start at a dose and adjust based on subjective effects
- Copying doses shared in forums and communities without understanding their origin
- Manufacturer suggestions that may have no pharmacological basis
This means that for many commonly used research peptides, there is genuine uncertainty about whether the doses used are optimal, subtherapeutic, or potentially excessive.
HED in Context: Comparing Calculated vs. Actual Clinical Doses#
For peptides that have both animal research and human clinical data, we can compare HED calculations to actual clinical doses:
| Peptide | Animal Dose (Species) | HED Calculation | Actual Clinical Dose | Match? |
|---|---|---|---|---|
| Ipamorelin | 100-300 mcg/kg (rat) | ~16-49 mcg/kg | ~1-3 mcg/kg | HED overestimates |
| Semaglutide | Various (monkey studies) | Varies | 0.035 mg/kg/week (2.4 mg/week at 70 kg) | Roughly comparable |
| Exenatide | 0.1-10 mcg/kg (rat) | 0.016-1.6 mcg/kg | ~0.14 mcg/kg (10 mcg BID at 70 kg) | Within range |
The comparison shows that HED calculations sometimes approximate clinical doses but can also significantly over- or underestimate them. This reinforces that HED is a tool for estimating starting points, not for predicting therapeutic doses.
Using the HED Calculator#
Our HED calculator tool automates the BSA scaling calculation. To use it:
- Enter the animal species used in the study
- Enter the animal dose (in mg/kg or mcg/kg)
- Enter your body weight (or use the default 70 kg)
- The calculator will output the HED in both mg/kg and total dose
The calculator applies the standard FDA K_m conversion factors. Remember that the output is an estimate, not a prescription.
For additional dosing tools, see our dosing calculator for reconstitution and measurement calculations.
Key Takeaways#
-
Simple weight-based scaling from animals to humans overestimates doses by approximately 6x (rat) to 12x (mouse) because it ignores metabolic rate differences.
-
The FDA's BSA scaling method using K_m factors is the standard approach for converting animal doses to human equivalent doses.
-
HED calculations estimate a safe starting dose, not the therapeutically effective dose. The actual effective dose in humans must be determined through clinical trials.
-
For most research peptides, the community-used doses are not formally derived from HED calculations. There is genuine uncertainty about whether these doses are optimal.
-
Peptides present additional challenges for dose conversion beyond standard BSA scaling, including species-specific receptor differences, route-dependent bioavailability, and local vs. systemic effects.
-
When reading animal studies, always apply BSA correction before extrapolating to human-relevant doses. Our HED calculator can help with this conversion.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:

{kind=link}
Frequently Asked Questions About Human Equivalent Dose (HED): How to Convert Animal Study Doses
What does this article cover?
Calculate human equivalent doses from animal studies using FDA body surface area scaling. Covers the HED formula and common mistakes. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers BPC-157, Ipamorelin. Key context: BPC-157 (One of the most commonly cited examples of extrapolating peptide doses from animal studies, as it...); Ipamorelin (GH secretagogue with some human clinical data, useful for illustrating how HED calculations compa...). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: One of the most commonly cited examples of extrapolating peptide doses from animal studies, as it.... GH secretagogue with some human clinical data, useful for illustrating how HED calculations compa.... These takeaways are based on the research data available at the time of publication.
What is BPC-157 and why is it significant?
BPC-157 is a peptide discussed in this article because: One of the most commonly cited examples of extrapolating peptide doses from animal studies, as it lacks human dose-finding trials. For a complete profile of BPC-157, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

The History of Peptide Research: From Insulin to Modern Therapeutics
History of peptide research from insulin's 1921 discovery to modern GLP-1 agonists. Key milestones in synthesis and therapeutics.
Core Peptides Review 2026: COAs, Finnrick Controversy, and Whether the Score Holds Up
An honest 2026 review of Core Peptides covering product range, payment flexibility, shipping, COA transparency, and how the Finnrick Analytics controversy should change how you read vendor ratings. Includes 8-dimension scoring.
How to Reconstitute Peptides: A Complete Step-by-Step Guide
A detailed guide to peptide reconstitution covering bacteriostatic water vs sterile water, step-by-step mixing technique, post-reconstitution dosing calculations, proper storage, and the most common mistakes to avoid.
You Might Also Like
Related content you may find interesting