Semaglutide vs Zovaglutide: Weekly vs Monthly GLP-1 Agonists
Evidence-based comparison of semaglutide (Wegovy/Ozempic) and zovaglutide (QL Biopharm), examining weekly vs monthly GLP-1 dosing frequency, STEP vs Phase 2 data, and the clinical implications of once-monthly injection.
Verdict at a Glance
Semaglutide is the proven standard with extensive Phase 3, real-world, and cardiovascular outcomes data across tens of thousands of patients. Zovaglutide offers the compelling advantage of once-monthly dosing (12-13 injections per year vs 52) with early Phase 2 data showing competitive weight loss and low GI side effect rates. However, zovaglutide has only 303 patients studied over 24 weeks, no Phase 3 data, and no long-term safety information. For current treatment decisions, semaglutide is the clear choice. Zovaglutide represents an important advance in dosing convenience if Phase 3 confirms the Phase 2 results.
| Best for | Pick | Why |
|---|---|---|
| Current obesity or diabetes treatment | Semaglutide | FDA-approved with proven efficacy across 10+ Phase 3 trials, CV outcomes data, and 8+ years of post-marketing experience |
| Minimum injection frequency (future) | Zovaglutide | 12-13 injections per year vs 52 with semaglutide; potential for best adherence among GLP-1 agonists if Phase 3 confirms efficacy |
| Cardiovascular risk reduction | Semaglutide | SELECT trial demonstrated 20% MACE reduction; zovaglutide has no cardiovascular outcomes data |
| Oral medication preference | Semaglutide | Rybelsus/oral semaglutide 25 mg available; zovaglutide is injectable only with no oral formulation in development |
| GI tolerability concerns | Zovaglutide | Phase 2 showed only 1.3% GI-related discontinuation, potentially the lowest rate among GLP-1 agonists, though this requires Phase 3 confirmation |
| Category | Semaglutide | Zovaglutide | Advantage |
|---|---|---|---|
| Mechanism of Action | Selective GLP-1 receptor agonist with C18 fatty diacid modification. Half-life of approximately 165 hours (7 days) enables once-weekly dosing. Aib substitution at position 2 confers DPP-4 resistance. Well-characterized pharmacology across injectable and oral formulations. | Selective GLP-1 receptor agonist with dual fatty acid chain modification that enhances albumin binding affinity. Half-life supports once-monthly (Q4W) or twice-monthly (Q2W) administration. Developed by Beijing QL Biopharmaceutical. Longest dosing interval of any GLP-1 agonist in clinical development. | Zovaglutide |
| Weight Loss Efficacy | STEP 1 demonstrated 14.9% mean weight loss at 2.4 mg over 68 weeks. 86.4% achieved 5% or more loss. Proven across 10+ STEP trials with consistent results. Extensively validated in diverse populations. | Phase 2 showed up to 14.4% weight loss at 160 mg monthly over 24 weeks. 89.9-97.1% achieved 5% or more loss across dose groups. Weight loss trajectory not yet plateaued at 24 weeks. Limited to 303 participants over 24 weeks. | Semaglutide |
| Development Stage and Evidence | FDA-approved for T2D (2017), obesity (2021), and CV risk reduction. 10+ completed Phase 3 STEP trials, SELECT CVOT, SUSTAIN program, PIONEER oral trials. Tens of thousands of patients studied. Most extensively validated GLP-1 agonist. | Phase 2 completed (303 patients, 24 weeks). Results presented at EASD 2025. Phase 3 planned but not yet initiated. No approved indications. No long-term safety data. No cardiovascular outcomes trial. Very early development stage. | Semaglutide |
| Dosing Convenience | Once-weekly subcutaneous injection (Wegovy/Ozempic). 52 injections per year. Also available as daily oral tablet (Rybelsus 14 mg for T2D; 25 mg for weight management approved 2025). Multiple formulation options. | Once-monthly (Q4W) subcutaneous injection. 12-13 injections per year (4-fold fewer than weekly semaglutide). Also tested at Q2W (26 injections per year). Fewest injections of any GLP-1 agonist in development. No oral formulation. | Zovaglutide |
| Safety Profile | Well-characterized GI side effects across thousands of patients. 8+ years of post-marketing data. Known risk profile including thyroid C-cell tumors (rodent), pancreatitis, and gallbladder events. Manageable with standard titration protocols. | Phase 2 showed low GI event rates with only 1.3% discontinuation due to GI AEs (lower than typical GLP-1 agonists). Monthly dosing group had fewer GI events than Q2W group. Very limited safety data (303 patients, 24 weeks). Long-term profile unknown. | Semaglutide |

Introduction#
Semaglutide and zovaglutide are both selective GLP-1 receptor agonists, but they represent different approaches to dosing frequency. Semaglutide (Ozempic/Wegovy/Rybelsus) is the current standard-of-care GLP-1 agonist with once-weekly injectable and daily oral formulations. Zovaglutide, developed by Beijing QL Biopharmaceutical, is designed as a potential once-monthly injectable GLP-1 agonist, which would reduce injection frequency by 4-fold compared to weekly semaglutide.
This comparison examines the clinical evidence, pharmacological differences, and the tradeoffs between semaglutide's proven track record and zovaglutide's convenience-focused development. It is important to note the substantial asymmetry in evidence: semaglutide has data from tens of thousands of patients across Phase 3 and real-world settings, while zovaglutide has only Phase 2 data from 303 patients over 24 weeks.
Mechanism of Action Comparison#
Semaglutide#
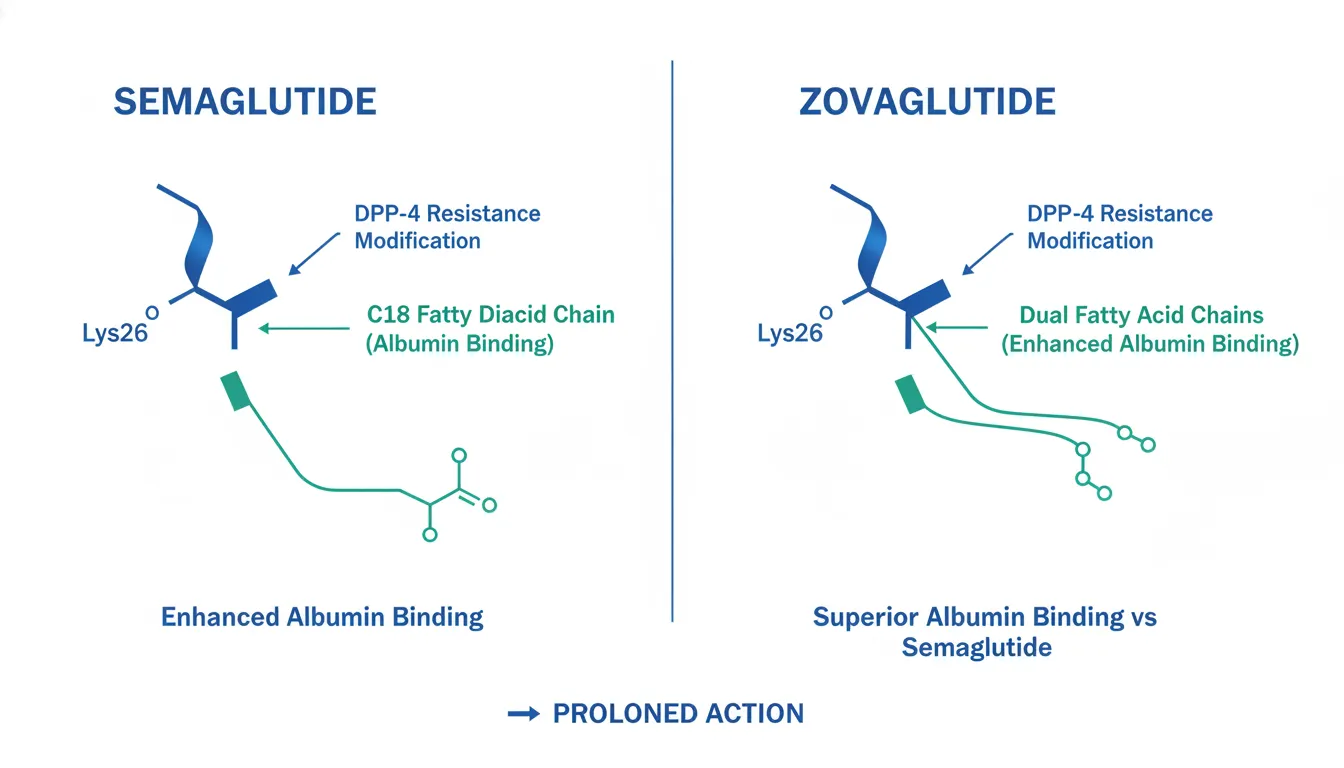
Semaglutide is a 31-amino acid human GLP-1 analog with three key modifications: an Aib substitution at position 2 for DPP-4 resistance, a C18 fatty diacid at Lys26 for albumin binding, and an Arg substitution at position 34 to prevent mis-acylation. These produce a half-life of approximately 165 hours (7 days), enabling true once-weekly pharmacokinetics from molecular design alone.
Zovaglutide#
Zovaglutide is a GLP-1 receptor agonist featuring a dual fatty acid chain modification that enhances binding affinity to serum albumin beyond what single-chain modifications achieve. This produces a substantially longer half-life than semaglutide, supporting once-monthly (every 4 weeks, Q4W) administration. The molecule was also tested at a twice-monthly (Q2W) dosing interval.
Pharmacokinetic Comparison#
| Property | Semaglutide | Zovaglutide |
|---|---|---|
| Receptor target | GLP-1R | GLP-1R |
| Half-life extension | C18 fatty diacid (single chain) | Dual fatty acid chain |
| Half-life | ~165 hours (7 days) | Supports Q4W dosing |
| Dosing interval | Once weekly | Once monthly (Q4W) or Q2W |
| Injections per year | 52 | 12-13 (Q4W) or 26 (Q2W) |
| Oral formulation | Yes (Rybelsus/oral 25 mg) | No |
Weight Loss Efficacy#
Semaglutide (STEP Program)#
Semaglutide's obesity efficacy is established across multiple large Phase 3 trials:
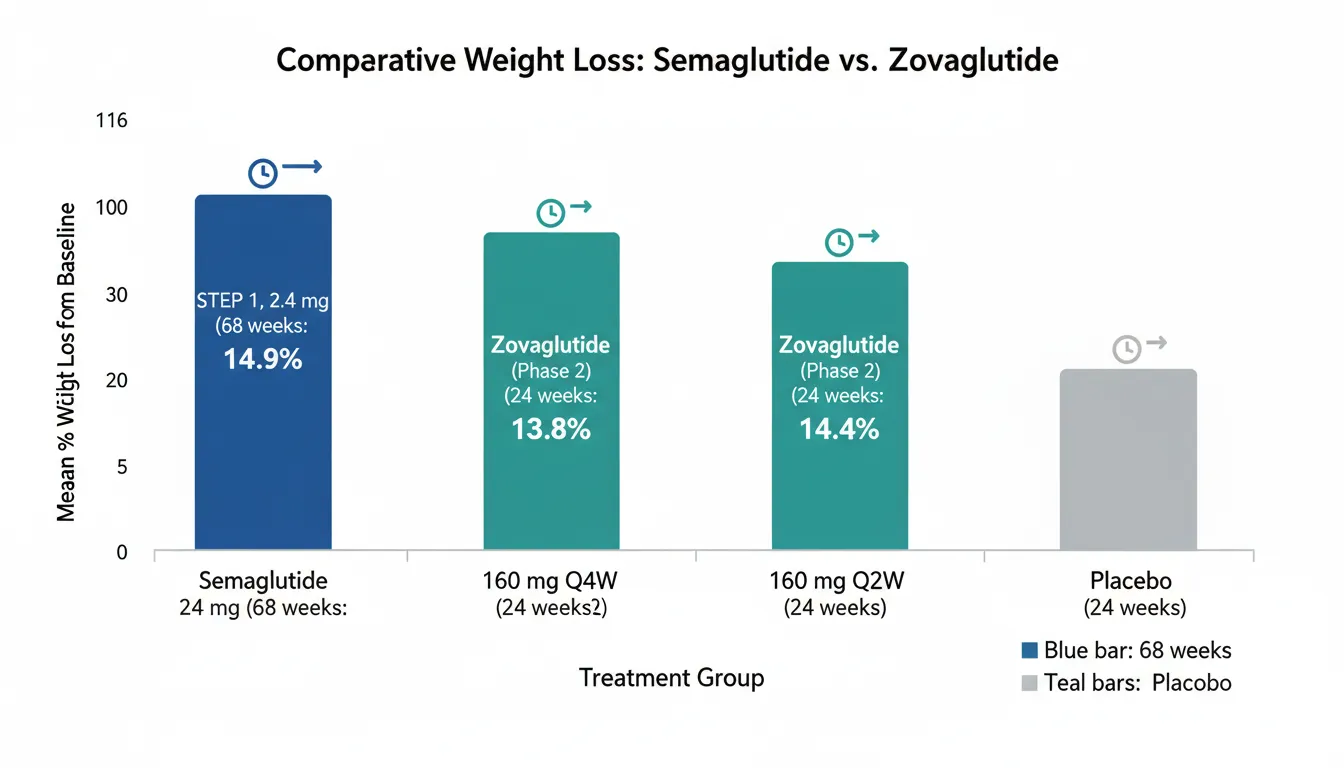
- STEP 1 (1,961 adults without T2D): 14.9% mean weight loss at 2.4 mg over 68 weeks; 86.4% achieved 5% or more; 50.5% achieved 15% or more
- STEP 2 (1,210 adults with T2D): 9.6% mean weight loss
- STEP 3 (with behavioral therapy): 16.0% mean weight loss
- STEP 5 (2-year data): 15.2% sustained weight loss at 104 weeks
Zovaglutide (Phase 2)#
Zovaglutide Phase 2 results (presented at EASD 2025) enrolled 303 overweight or obese adults across five dose arms over 24 weeks:
| Dose Group | Weight Loss | Achieved 5% or More |
|---|---|---|
| 80 mg Q4W (monthly) | 10.6% | 89.9% |
| 160 mg Q4W (monthly) | 13.8% | 93.9% |
| 80 mg Q2W (biweekly) | 12.5% | 97.1% |
| 160 mg Q2W (biweekly) | 14.4% | 93.6% |
| Placebo | 2.4% | 13.0% |
Cross-Trial Comparison (Important Caveats)#
Zovaglutide's Phase 2 results (10.6-14.4% at 24 weeks) suggest a competitive weight loss trajectory, but several critical differences preclude direct comparison:
- Duration: 24 weeks (zovaglutide) vs 68 weeks (semaglutide STEP 1). Weight loss typically continues beyond 24 weeks.
- Population size: 303 (zovaglutide) vs 1,961 (STEP 1). Smaller trials often show larger effect sizes.
- Trial phase: Phase 2 vs Phase 3. Phase 2 results often do not fully replicate in Phase 3.
- Population: May differ in baseline BMI, demographics, and other characteristics.
The weight loss trajectory of zovaglutide at 24 weeks appears comparable to semaglutide's trajectory at the same time point in STEP 1, but longer-duration Phase 3 data are needed to confirm this.
Cardiovascular and Long-Term Evidence#
Semaglutide#
- SELECT trial (17,604 patients, 39.8 months): 20% MACE reduction in overweight/obese adults without diabetes (HR 0.80, p<0.001)
- SUSTAIN 6 (3,297 patients): 26% MACE reduction in T2D
- STEP 5: 15.2% weight loss sustained at 2 years
- STEP 4: Weight regain of approximately two-thirds after drug withdrawal
- Extensive post-marketing real-world data (8+ years)
Zovaglutide#
- No cardiovascular outcomes trial completed or planned
- No data beyond 24 weeks
- No real-world post-marketing experience
- Phase 3 planned but not yet initiated
The evidence gap is substantial. Semaglutide's cardiovascular outcomes data and multi-year safety experience cannot be replicated quickly; zovaglutide would require years of Phase 3 trials and post-marketing surveillance to approach comparable evidence maturity.
Dosing and Administration#
Semaglutide#
- Wegovy (obesity): 0.25 mg weekly, titrate monthly to 2.4 mg over 16 weeks
- Ozempic (T2D): 0.25 mg weekly, titrate to 0.5 mg, max 2.0 mg
- Rybelsus (T2D): 3 mg daily oral, escalate to 7 mg, max 14 mg
- Oral semaglutide 25 mg (approved 2025): Oral for weight management
- 52 injections per year (injectable) or daily oral
Zovaglutide#
- Phase 2 tested 80 mg and 160 mg at Q4W (monthly) and Q2W (biweekly) intervals
- Monthly dosing (Q4W): 12-13 injections per year
- Biweekly dosing (Q2W): 26 injections per year
- Final dose and schedule will be determined by Phase 3
- No oral formulation
The monthly dosing proposition is zovaglutide's most compelling differentiator. Reducing injections from 52 to 12-13 per year could meaningfully improve long-term adherence, particularly for patients who find weekly injections burdensome.
Safety Comparison#
Semaglutide#
Well-characterized safety profile across thousands of patients:
- GI adverse events: 50-70% (mostly mild-moderate, dose-escalation related)
- Discontinuation due to AEs: ~7% (STEP 1)
- Boxed warning: Thyroid C-cell tumors (rodent data)
- Post-marketing signals: Pancreatitis, gallbladder events, ileus (rare)
- 8+ years of post-marketing surveillance
Zovaglutide#
Phase 2 safety data (303 patients, 24 weeks):
- GI adverse events: Present but low severity
- Discontinuation due to GI AEs: 1.3% (notably low for GLP-1 class)
- Monthly dosing showed fewer GI events than biweekly dosing
- No long-term safety data available
- No post-marketing experience
The 1.3% GI-related discontinuation rate is notably lower than typical GLP-1 agonists (5-10%). If confirmed in Phase 3, this could represent a meaningful tolerability advantage. The monthly dosing interval may inherently reduce GI side effects by avoiding the peak-trough fluctuations associated with more frequent dosing.
Key Differences Summary#
| Feature | Semaglutide | Zovaglutide |
|---|---|---|
| Regulatory status | FDA-approved (T2D, obesity, CV) | Phase 2 completed |
| Dosing interval | Weekly (injection) or daily (oral) | Monthly (Q4W) |
| Injections per year | 52 | 12-13 |
| Weight loss (max) | 14.9% at 68 weeks (STEP 1) | 14.4% at 24 weeks (Phase 2) |
| CV outcomes | 20% MACE reduction (SELECT) | No data |
| Total patients studied | Tens of thousands | 303 |
| GI discontinuation rate | ~7% | 1.3% |
| Oral formulation | Yes | No |
| Estimated availability | Currently available | Years away (Phase 3 not started) |
| Developer | Novo Nordisk | QL Biopharmaceutical (China) |
Conclusion#
Semaglutide is the proven standard-of-care with decades of clinical trial data, cardiovascular outcomes evidence, real-world validation, and multiple formulation options. Zovaglutide's once-monthly dosing represents a genuine advancement in patient convenience that could improve long-term adherence if Phase 3 trials confirm the promising Phase 2 results. The 1.3% GI discontinuation rate is encouragingly low. However, zovaglutide is years away from potential approval, has only 303 patients studied over 24 weeks, and lacks any long-term safety or cardiovascular outcomes data. For current treatment decisions, semaglutide is the clear choice. Zovaglutide should be watched as a potentially important next-generation option for patients who prioritize minimal injection frequency.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Current obesity or diabetes treatment
Semaglutide
FDA-approved with proven efficacy across 10+ Phase 3 trials, CV outcomes data, and 8+ years of post-marketing experience
Minimum injection frequency (future)
Zovaglutide
12-13 injections per year vs 52 with semaglutide; potential for best adherence among GLP-1 agonists if Phase 3 confirms efficacy
Cardiovascular risk reduction
Semaglutide
SELECT trial demonstrated 20% MACE reduction; zovaglutide has no cardiovascular outcomes data
Oral medication preference
Semaglutide
Rybelsus/oral semaglutide 25 mg available; zovaglutide is injectable only with no oral formulation in development
GI tolerability concerns
Zovaglutide
Phase 2 showed only 1.3% GI-related discontinuation, potentially the lowest rate among GLP-1 agonists, though this requires Phase 3 confirmation
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Semaglutide vs Zovaglutide: Weekly vs Monthly GLP-1 Agonists
Which is better, Semaglutide or Zovaglutide?
Semaglutide is the proven standard with extensive Phase 3, real-world, and cardiovascular outcomes data across tens of thousands of patients. Zovaglutide offers the compelling advantage of once-monthly dosing (12-13 injections per year vs 52) with early Phase 2 data showing competitive weight loss and low GI side effect rates. However, zovaglutide has only 303 patients studied over 24 weeks, no Phase 3 data, and no long-term safety information. For current treatment decisions, semaglutide is ... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Semaglutide and Zovaglutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Zovaglutide; Weight Loss Efficacy: advantage goes to Semaglutide; Development Stage and Evidence: advantage goes to Semaglutide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Semaglutide over Zovaglutide?
For the scenario of "Current obesity or diabetes treatment," research data suggests Semaglutide may be more relevant. FDA-approved with proven efficacy across 10+ Phase 3 trials, CV outcomes data, and 8+ years of post-marketing experience. This is based on currently available evidence and individual circumstances may differ.
How do Semaglutide and Zovaglutide differ in their mechanisms of action?
Semaglutide: Selective GLP-1 receptor agonist with C18 fatty diacid modification. Half-life of approximately 165 hours (7 days) enables once-weekly dosing. Aib substitution at position 2 confers DPP-4 resistanc.... Zovaglutide: Selective GLP-1 receptor agonist with dual fatty acid chain modification that enhances albumin binding affinity. Half-life supports once-monthly (Q4W) or twice-monthly (Q2W) administration. Develop....
Which has fewer side effects, Semaglutide or Zovaglutide?
In terms of side effects and tolerability, the advantage goes to Semaglutide. Semaglutide: Well-characterized GI side effects across thousands of patients. 8+ years of post-marketing data. Known risk profile including thyroid C-cell tumor.... Zovaglutide: Phase 2 showed low GI event rates with only 1.3% discontinuation due to GI AEs (lower than typical GLP-1 agonists). Monthly dosing group had fewer ....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.