BPC-157 vs Teduglutide: Gut Healing Peptides Compared
Evidence-based comparison of BPC-157 and teduglutide (Gattex) for gut healing -- a preclinical research peptide with broad tissue repair properties versus an FDA-approved GLP-2 analog for short bowel syndrome.
Verdict at a Glance
BPC-157 and teduglutide address gut healing through fundamentally different approaches with very different evidence bases. Teduglutide is the clear winner for clinical validation -- it is FDA-approved with Phase 3 data for short bowel syndrome, demonstrating a 63% response rate and enabling reduction or elimination of parenteral nutrition. BPC-157 has no published human clinical trials despite extensive preclinical data. However, BPC-157 has broader theoretical applications across multiple tissue types and is far more accessible and affordable. For short bowel syndrome specifically, teduglutide is the proven treatment. For general gut healing, tissue repair, or conditions outside SBS, BPC-157 offers preclinical promise but lacks the clinical evidence to support definitive recommendations.
| Best for | Pick | Why |
|---|---|---|
| Short Bowel Syndrome | Teduglutide | FDA-approved with Phase 3 evidence showing 63% response rate. Proven to reduce parenteral nutrition dependence with up to 3.5 years of long-term data. The only clinically validated treatment for SBS-IF. |
| Evidence-Based Medicine | Teduglutide | Published Phase 3 RCTs, FDA approval, and established safety monitoring protocols. BPC-157 has zero published human clinical trials. |
| General Gut Healing (Ulcers, IBD) | Neither has definitive evidence | BPC-157 has extensive preclinical data for gastric ulcers and IBD models, but no human trials. Teduglutide is only studied in SBS, not IBD or ulcers. Neither is validated for general gut healing in humans. |
| Musculoskeletal or Multi-Tissue Repair | BPC-157 | BPC-157 has preclinical evidence across tendon, ligament, muscle, bone, and nerve healing. Teduglutide is gut-specific with no evidence for musculoskeletal repair. However, BPC-157's evidence is preclinical only. |
| Cost and Accessibility | BPC-157 | BPC-157 costs $30-80 per vial from research suppliers. Teduglutide costs over $300,000 per year and requires a prescription for SBS only. |
| Established Safety Profile | Teduglutide | Teduglutide has systematic safety data from clinical trials and post-marketing surveillance. BPC-157 has no human safety data beyond anecdotal reports. |
| Category | BPC-157 | Teduglutide | Advantage |
|---|---|---|---|
| Mechanism of Action | BPC-157 (Body Protection Compound-157) is a 15-amino acid synthetic peptide derived from human gastric juice. It promotes tissue healing through multiple pathways including upregulation of growth factors (EGF, VEGF), stimulation of the Egr-1/NAB2 gene pathway, modulation of the nitric oxide system, and enhancement of blood flow to damaged tissues. It does not directly stimulate cell proliferation but creates conditions favorable for healing. | Teduglutide is a GLP-2 analog with a glycine substitution at position 2 that confers DPP-4 resistance, extending half-life from 7 minutes to 2-3 hours. It directly activates the GLP-2 receptor on intestinal subepithelial myofibroblasts, stimulating IGF-1 production and promoting crypt cell proliferation, villus growth, and intestinal adaptation. | Comparable |
| Research Evidence | BPC-157 has over 100 preclinical studies showing tissue-protective effects across gastrointestinal, musculoskeletal, cardiovascular, and neurological systems. However, it has no published human clinical trials. All evidence is from animal models or cell culture. The breadth of claimed effects raises questions about reproducibility and specificity. | Teduglutide has robust Phase 3 clinical evidence from the pivotal STEPS trials (n=169) demonstrating 63% response rate in short bowel syndrome vs 30% placebo. FDA-approved in 2012 for adults and 2019 for children. Long-term data up to 3.5 years shows continued intestinal adaptation. Published in peer-reviewed journals. | Teduglutide |
| Side Effect Profile | BPC-157 has no systematic human safety data. Preclinical studies suggest good tolerability in animal models. Reported side effects from unregulated human use include nausea, dizziness, and injection site reactions. No long-term safety data in humans. Theoretical concern about effects on tumor angiogenesis due to VEGF upregulation. | Well-characterized safety profile from clinical trials. Common side effects include abdominal pain (30%), nausea (18-27%), headache (16%), catheter complications, and injection site reactions. Requires colonoscopy surveillance due to theoretical risk of intestinal polyps from chronic GLP-2R stimulation. Biliary and pancreatic monitoring recommended. | Comparable |
| Scope of Application | BPC-157 is used for a wide range of conditions in preclinical models including gastric ulcers, inflammatory bowel disease, tendon and ligament healing, muscle injuries, bone fractures, peripheral nerve damage, and liver protection. The breadth of applications is both a strength (versatility) and a weakness (lack of focused clinical data for any single indication). | Teduglutide has a single, well-defined indication -- intestinal failure associated with short bowel syndrome. It promotes intestinal adaptation (crypt proliferation, villus growth) to reduce or eliminate dependence on parenteral nutrition. Not used for other GI conditions like IBD, ulcers, or non-SBS intestinal healing. | BPC-157 |
| Regulatory Status and Access | BPC-157 is not FDA-approved for any indication. Available from research peptide suppliers and some compounding pharmacies. No prescription required from research sources. Quality varies between suppliers. Affordable (typically $30-80 per vial). | FDA-approved (2012) as Gattex for short bowel syndrome in adults; 2019 for children aged 1+. Available by prescription only. Manufactured by Takeda under GMP standards. Expensive (approximately $300,000+ per year at 0.05 mg/kg/day). | Comparable |

Introduction#
BPC-157 and teduglutide represent two fundamentally different approaches to gut healing: BPC-157 is a research peptide with broad preclinical evidence for tissue repair across multiple organ systems but no human clinical trials, while teduglutide (Gattex) is an FDA-approved GLP-2 analog with specific, proven efficacy for short bowel syndrome. Their comparison illustrates the gap between preclinical promise and clinical validation in peptide therapeutics.
Both peptides are derived from naturally occurring gut-related proteins -- BPC-157 from human gastric juice, teduglutide from the intestinal hormone GLP-2 -- but they differ in mechanism, specificity, evidence quality, and regulatory status. This comparison examines the scientific evidence, mechanisms, and practical considerations for each.
Mechanism of Action Comparison#
BPC-157#
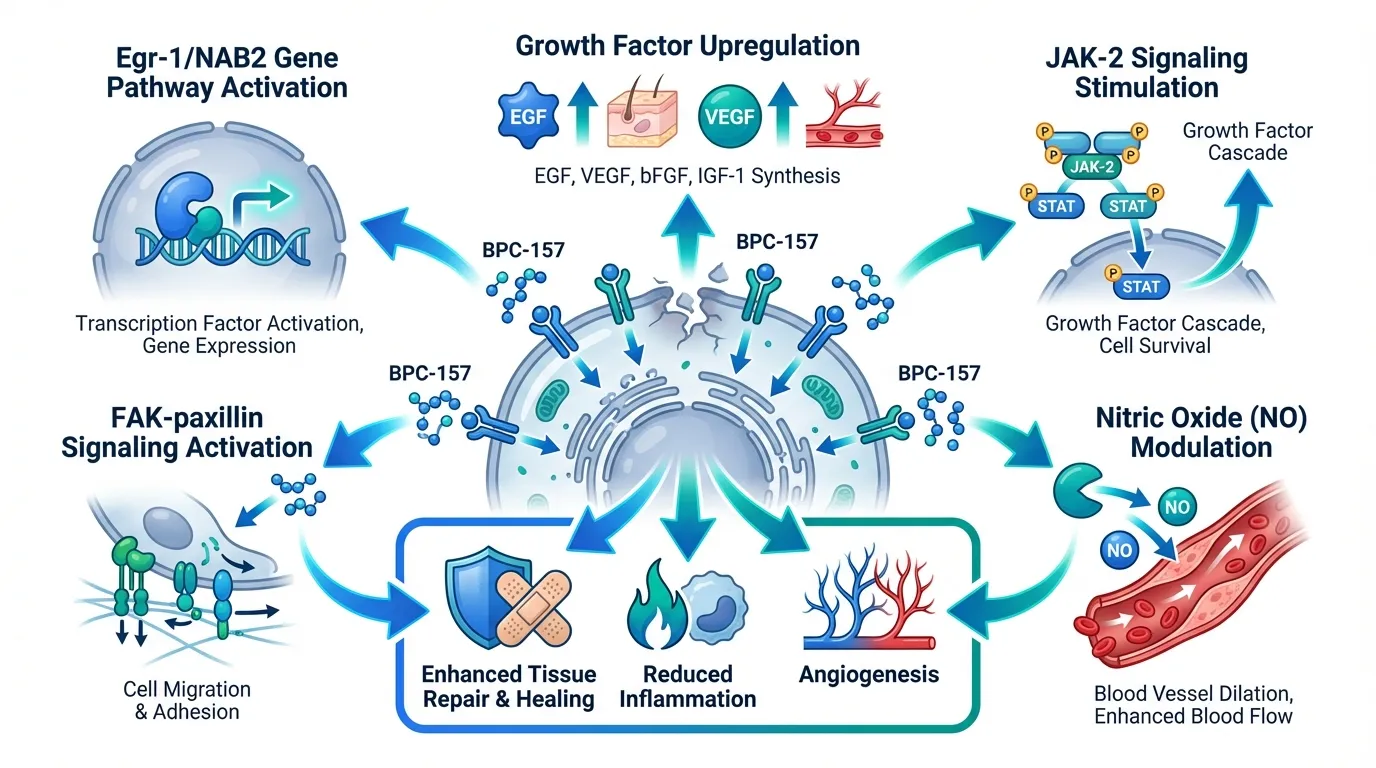
BPC-157 (Body Protection Compound-157) is a synthetic 15-amino acid peptide (GEPPPGKPADDAGLV) derived from a protein found in human gastric juice. Its mechanism involves multiple pathways:
- Egr-1/NAB2 gene pathway: Stimulates early growth response protein 1, a transcription factor involved in wound healing, angiogenesis, and tissue repair
- FAK-paxillin signaling: Activates focal adhesion kinase pathways important for cell migration and wound closure
- JAK-2 signaling: Stimulates janus kinase 2 pathway involved in growth factor signaling
- Nitric oxide modulation: Interacts with the NO system to enhance blood flow to damaged tissues
- Growth factor upregulation: Increases EGF, VEGF, and other growth factors at injury sites
BPC-157 does not directly stimulate cell proliferation. Instead, it creates an environment conducive to healing by enhancing blood flow, modulating inflammation, and upregulating repair pathways.
Teduglutide#
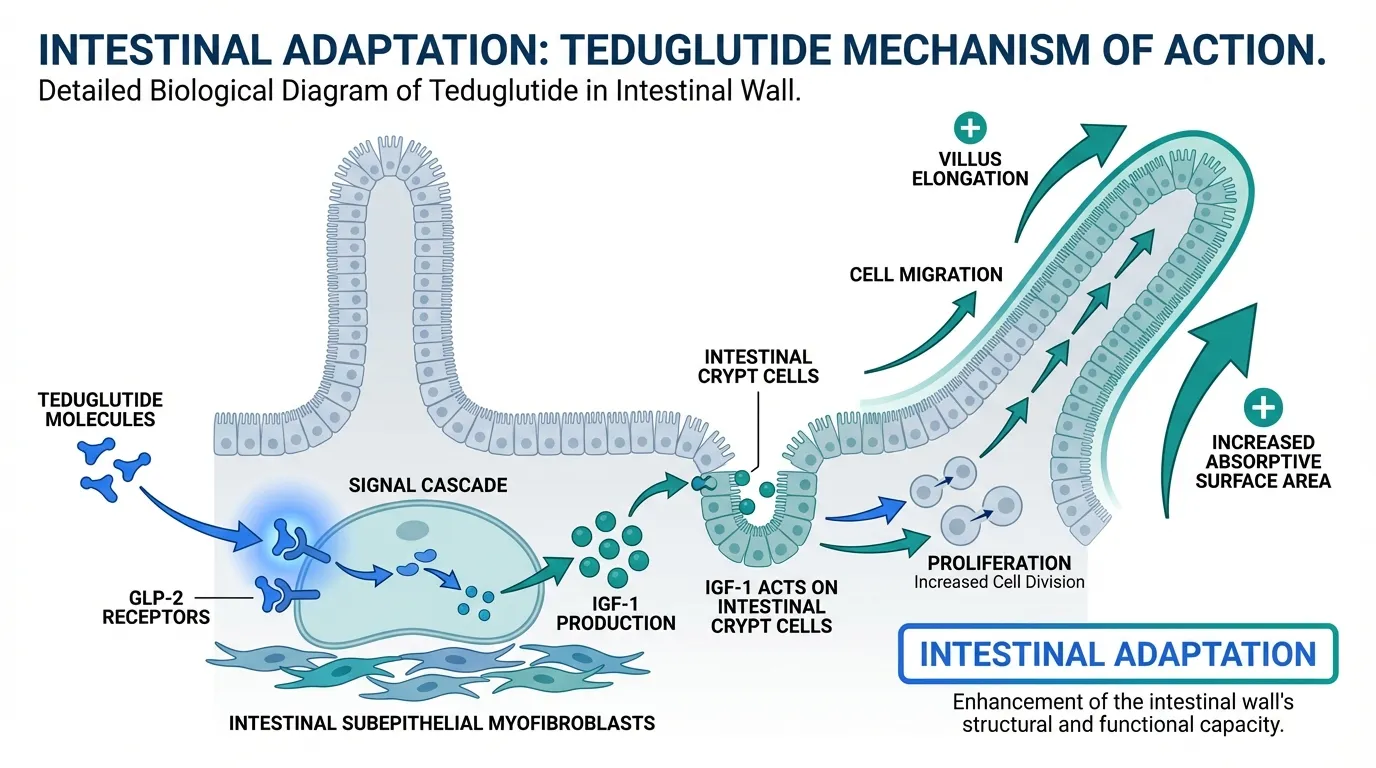
Teduglutide is a 33-amino acid GLP-2 analog ([Gly2]-GLP-2) with a well-defined, single-target mechanism:
- GLP-2 receptor activation: Directly binds and activates the GLP-2 receptor on intestinal subepithelial myofibroblasts
- IGF-1 stimulation: GLP-2R activation stimulates production of insulin-like growth factor 1 in the intestinal wall
- Crypt cell proliferation: IGF-1 drives proliferation of intestinal crypt cells, expanding the stem cell compartment
- Villus growth: Increased crypt cell production leads to villus elongation and greater absorptive surface area
- Intestinal adaptation: The combined effect promotes structural adaptation of the remaining bowel in SBS patients
Mechanistic Comparison#
| Feature | BPC-157 | Teduglutide |
|---|---|---|
| Source | Human gastric juice (synthetic) | GLP-2 analog (synthetic) |
| Size | 15 amino acids (~1,419 Da) | 33 amino acids (~3,766 Da) |
| Primary mechanism | Multi-pathway tissue repair | GLP-2 receptor agonism |
| Target specificity | Broad (multiple tissues) | Narrow (intestinal GLP-2R) |
| Cell proliferation | Indirect (growth factor upregulation) | Direct (crypt cell proliferation) |
| Angiogenesis | Yes (VEGF upregulation) | Minimal |
| Intestinal adaptation | Not specifically studied | Proven (villus growth, crypt depth) |
| Half-life | Not fully characterized | 2-3 hours (vs 7 min for native GLP-2) |
Dosing Comparison#
BPC-157 Dosing#
| Parameter | Details |
|---|---|
| Route | Subcutaneous injection or oral |
| Research dose | 200-800 mcg/day (human-equivalent from animal studies) |
| Frequency | Once or twice daily |
| Duration | Typically 4-8 weeks in research use |
| Oral bioavailability | Some evidence for oral activity (unusual for peptides) |
| Reconstitution | Required (lyophilized powder) |
| Stability | Stable in gastric acid (derives from gastric protein) |
Teduglutide Dosing#
| Parameter | Details |
|---|---|
| Route | Subcutaneous injection |
| Approved dose | 0.05 mg/kg once daily |
| Frequency | Once daily |
| Duration | Chronic (long-term treatment) |
| Oral bioavailability | None (must be injected) |
| Reconstitution | Required (lyophilized powder with prefilled syringe diluent) |
| Administration | Patient self-injection after training |
Side Effects Comparison#
BPC-157 Side Effects#
No systematic human safety data exists. Reported effects from preclinical and unregulated human use:
- Nausea (anecdotal, from community reports)
- Dizziness (rare, anecdotal)
- Injection site reactions (bruising, redness)
- Headache (rare)
- Theoretical concern about VEGF-mediated tumor angiogenesis
Teduglutide Side Effects#
Well-characterized from clinical trials:
| Side Effect | Teduglutide (0.05 mg/kg) | Placebo | Notes |
|---|---|---|---|
| Abdominal pain | 30% | 25% | Most common GI effect |
| Nausea | 18-27% | 14% | Usually transient |
| Headache | 16% | 12% | Mild |
| Injection site reactions | 22% | 5% | Erythema, bruising |
| Catheter complications | 14% | 10% | Related to CVC for PN |
| Upper respiratory infection | 12% | 10% | Not clearly treatment-related |
Monitoring requirements: Teduglutide requires colonoscopy within 6 months of starting and then every 5 years due to theoretical risk of intestinal polyps or neoplasia from chronic intestinal proliferation. Pancreatic and biliary monitoring is also recommended.
Research Evidence Comparison#
BPC-157 Research#
BPC-157 has extensive preclinical data but no published human trials:
GI healing studies (animal models):
- Gastric ulcer healing in rat models with multiple induction methods
- Inflammatory bowel disease models showing reduced inflammation and mucosal healing
- Esophagitis, duodenal ulcer, and fistula healing in rodents
- Liver protection in hepatotoxicity models
Non-GI healing studies (animal models):
- Tendon and ligament repair (Achilles tendon, MCL models)
- Muscle healing after crush injury
- Bone fracture healing
- Peripheral nerve regeneration
- Brain-gut axis modulation
Evidence level: Low -- extensive preclinical data, no human clinical trials.
Teduglutide Research#
Teduglutide has a strong clinical evidence base:
STEPS Phase 3 trial (n=86): Randomized, placebo-controlled. 63% of teduglutide patients achieved the primary endpoint (>=20% reduction in PN volume) vs 30% placebo. Mean PN volume reduction of 4.4 L/week vs 2.3 L with placebo at 24 weeks.
Long-term extension (up to 3.5 years): Continued intestinal adaptation with progressive reductions in PN requirements. Some patients achieved complete independence from PN.
Pediatric Phase 3: Led to 2019 FDA approval for children aged 1 year and older with SBS.
Evidence level: High -- Phase 3 RCTs, FDA-approved, long-term data available.
Evidence Comparison Table#
| Feature | BPC-157 | Teduglutide |
|---|---|---|
| Human RCTs | None | Multiple Phase 3 |
| FDA approval | No | Yes (2012 adults, 2019 children) |
| Total human trial subjects | 0 (published) | >300 across trials |
| Long-term data | None (human) | Up to 3.5 years |
| Peer-reviewed publications | >100 (preclinical) | Multiple (clinical) |
| Evidence quality | Low (preclinical only) | High (Phase 3 RCTs) |
Key Differences Summary#
- Evidence quality: Teduglutide has Phase 3 RCTs and FDA approval; BPC-157 has no human clinical trials.
- Mechanism: Teduglutide directly stimulates intestinal growth through the GLP-2 receptor; BPC-157 modulates multiple healing pathways indirectly.
- Specificity: Teduglutide is intestine-specific; BPC-157 shows preclinical activity across multiple tissues.
- Regulatory status: Teduglutide is FDA-approved for SBS; BPC-157 is an unregulated research peptide.
- Cost: Teduglutide costs >$300,000/year; BPC-157 costs $30-80 per vial from research suppliers.
- Oral availability: BPC-157 may have oral activity (unusual for peptides); teduglutide requires injection.
- Monitoring: Teduglutide requires colonoscopy and pancreatic/biliary surveillance; BPC-157 has no established monitoring protocol.
- Indication breadth: BPC-157 is explored for GI, musculoskeletal, neurological, and cardiovascular conditions; teduglutide is only for SBS-IF.
Conclusion#
BPC-157 and teduglutide occupy opposite ends of the evidence spectrum for gut healing peptides. Teduglutide is the only clinically validated peptide therapy for intestinal repair, with Phase 3 data and FDA approval for short bowel syndrome demonstrating its ability to promote intestinal adaptation and reduce parenteral nutrition dependence. For SBS patients, it is the proven, standard-of-care treatment.
BPC-157 has a compelling preclinical profile suggesting broad tissue-protective and healing effects across the gastrointestinal tract and beyond. Its potential oral bioavailability and multi-tissue activity make it a uniquely interesting research peptide. However, the complete absence of published human clinical trials is a significant limitation. The gap between extensive animal data and zero human validation remains BPC-157's fundamental weakness.
For patients with short bowel syndrome, teduglutide is the clear choice. For individuals exploring general gut healing, tissue repair, or conditions not addressed by teduglutide, BPC-157 represents an intriguing preclinical option that awaits the human clinical data needed to establish its place in evidence-based medicine.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Short Bowel Syndrome
Teduglutide
FDA-approved with Phase 3 evidence showing 63% response rate. Proven to reduce parenteral nutrition dependence with up to 3.5 years of long-term data. The only clinically validated treatment for SBS-IF.
Evidence-Based Medicine
Teduglutide
Published Phase 3 RCTs, FDA approval, and established safety monitoring protocols. BPC-157 has zero published human clinical trials.
General Gut Healing (Ulcers, IBD)
Neither has definitive evidence
BPC-157 has extensive preclinical data for gastric ulcers and IBD models, but no human trials. Teduglutide is only studied in SBS, not IBD or ulcers. Neither is validated for general gut healing in humans.
Musculoskeletal or Multi-Tissue Repair
BPC-157
BPC-157 has preclinical evidence across tendon, ligament, muscle, bone, and nerve healing. Teduglutide is gut-specific with no evidence for musculoskeletal repair. However, BPC-157's evidence is preclinical only.
Cost and Accessibility
BPC-157
BPC-157 costs $30-80 per vial from research suppliers. Teduglutide costs over $300,000 per year and requires a prescription for SBS only.
Established Safety Profile
Teduglutide
Teduglutide has systematic safety data from clinical trials and post-marketing surveillance. BPC-157 has no human safety data beyond anecdotal reports.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About BPC-157 vs Teduglutide: Gut Healing Peptides Compared
Which is better, BPC-157 or Teduglutide?
BPC-157 and teduglutide address gut healing through fundamentally different approaches with very different evidence bases. Teduglutide is the clear winner for clinical validation -- it is FDA-approved with Phase 3 data for short bowel syndrome, demonstrating a 63% response rate and enabling reduction or elimination of parenteral nutrition. BPC-157 has no published human clinical trials despite extensive preclinical data. However, BPC-157 has broader theoretical applications across multiple ti... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between BPC-157 and Teduglutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to Teduglutide; Side Effect Profile: advantage goes to neither (tie). 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Teduglutide over BPC-157?
For the scenario of "Short Bowel Syndrome," research data suggests Teduglutide may be more relevant. FDA-approved with Phase 3 evidence showing 63% response rate. Proven to reduce parenteral nutrition dependence with up to 3.5 years of long-term data. The only clinically validated treatment for SB.... This is based on currently available evidence and individual circumstances may differ.
How do BPC-157 and Teduglutide differ in their mechanisms of action?
BPC-157: BPC-157 (Body Protection Compound-157) is a 15-amino acid synthetic peptide derived from human gastric juice. It promotes tissue healing through multiple pathways including upregulation of growth f.... Teduglutide: Teduglutide is a GLP-2 analog with a glycine substitution at position 2 that confers DPP-4 resistance, extending half-life from 7 minutes to 2-3 hours. It directly activates the GLP-2 receptor on i....
Which has fewer side effects, BPC-157 or Teduglutide?
In terms of side effects and tolerability, the advantage goes to neither (comparable). BPC-157: BPC-157 has no systematic human safety data. Preclinical studies suggest good tolerability in animal models. Reported side effects from unregulated.... Teduglutide: Well-characterized safety profile from clinical trials. Common side effects include abdominal pain (30%), nausea (18-27%), headache (16%), catheter....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.