BPC-157 vs Ziconotide: Healing Peptide vs Approved Pain Medication
Comparison of BPC-157 and ziconotide, two peptides with very different profiles -- a preclinical healing peptide versus an FDA-approved intrathecal analgesic for severe chronic pain.
Verdict at a Glance
BPC-157 and ziconotide serve fundamentally different purposes and represent opposite ends of the evidence spectrum. Ziconotide is an FDA-approved medication with rigorous clinical trial data, but it is reserved for severe refractory pain requiring intrathecal delivery and carries significant CNS side effects. BPC-157 is a preclinical healing peptide with broad tissue repair properties but essentially no human clinical data. They are not interchangeable or directly competitive. Ziconotide treats pain through neural blockade. BPC-157 aims to heal the underlying tissue damage. They address different aspects of injury and disease.
| Best for | Pick | Why |
|---|---|---|
| Severe Refractory Chronic Pain | Ziconotide | Ziconotide is FDA-approved specifically for chronic severe pain refractory to other treatments. It is the only non-opioid intrathecal analgesic with regulatory approval and is indicated when all other pain management strategies have failed. |
| Tissue Healing Research | BPC-157 | BPC-157 has the broadest preclinical evidence for tissue repair across tendons, ligaments, muscle, bone, and GI mucosa. Its pleiotropic healing mechanism is unique among peptides studied for injury recovery. |
| Non-Addictive Pain Management | Ziconotide | Ziconotide does not bind opioid receptors and produces no tolerance, dependence, or addiction. It is the evidence-based non-opioid option for intractable pain. Development of tolerance is not observed with chronic use. |
| Musculoskeletal Injury Recovery | BPC-157 | Preclinical data specifically in tendon transection, ligament repair, and muscle healing models is extensive. BPC-157 promoted tendon outgrowth, cell survival, and migration in multiple injury models and enhanced growth hormone receptor expression in tendon fibroblasts. |
| Regulatory-Approved Treatment | Ziconotide | Ziconotide (Prialt) is the only option with FDA approval, phase 3 trial data, established manufacturing standards, and ongoing post-marketing surveillance. BPC-157 has no regulatory approval anywhere. |
| Category | BPC-157 | Ziconotide | Advantage |
|---|---|---|---|
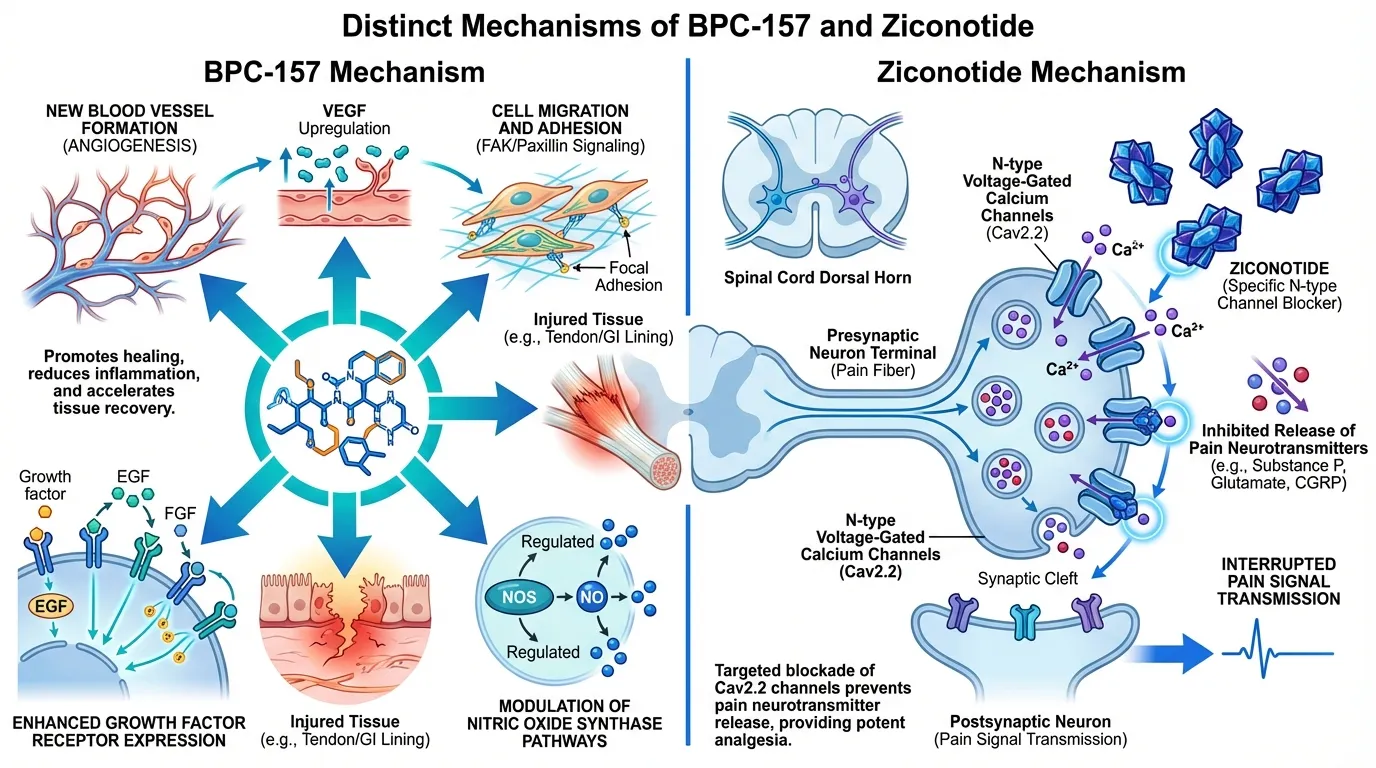
| Mechanism of Action | Pentadecapeptide (15 amino acids) derived from human gastric juice. Pleiotropic healing mechanism involving upregulation of VEGF (angiogenesis), FAK/paxillin (cell adhesion), growth hormone receptor expression, and NOS pathways. Promotes tissue repair across multiple organ systems including tendons, ligaments, muscle, and GI mucosa. | Synthetic 25-amino acid conopeptide (derived from Conus magus cone snail venom). Selectively blocks N-type voltage-gated calcium channels (Cav2.2) in the spinal cord dorsal horn. Inhibits neurotransmitter release (substance P, glutamate) from nociceptive afferents. Purely analgesic mechanism with no tissue-healing properties. | Comparable |
| Research Evidence | Extensive preclinical data across dozens of animal models of tissue injury. Virtually no human clinical trial data. One small pilot study in chronic knee pain (7/12 patients with 6+ month relief). Systematic reviews note promising preclinical evidence but absence of rigorous human RCTs. | FDA-approved (2004) based on multiple randomized, double-blind, placebo-controlled trials. Demonstrated significant pain reduction in both cancer/AIDS-related pain and noncancer chronic pain. Phase 3 data available. Post-marketing surveillance ongoing. | Ziconotide |
| Side Effect Profile | No systematic human safety data. Preclinical studies report excellent tolerance with no observed toxicity. As a gastric peptide fragment, it is expected to have low systemic toxicity. However, the lack of human safety trials means the side effect profile is truly unknown. | Narrow therapeutic window with significant CNS side effects including dizziness, nausea, confusion, memory impairment, and nystagmus. Serious psychiatric effects (hallucinations, psychosis, suicidal ideation) reported. Requires careful slow titration. FDA black box warning for severe psychiatric symptoms. | BPC-157 |
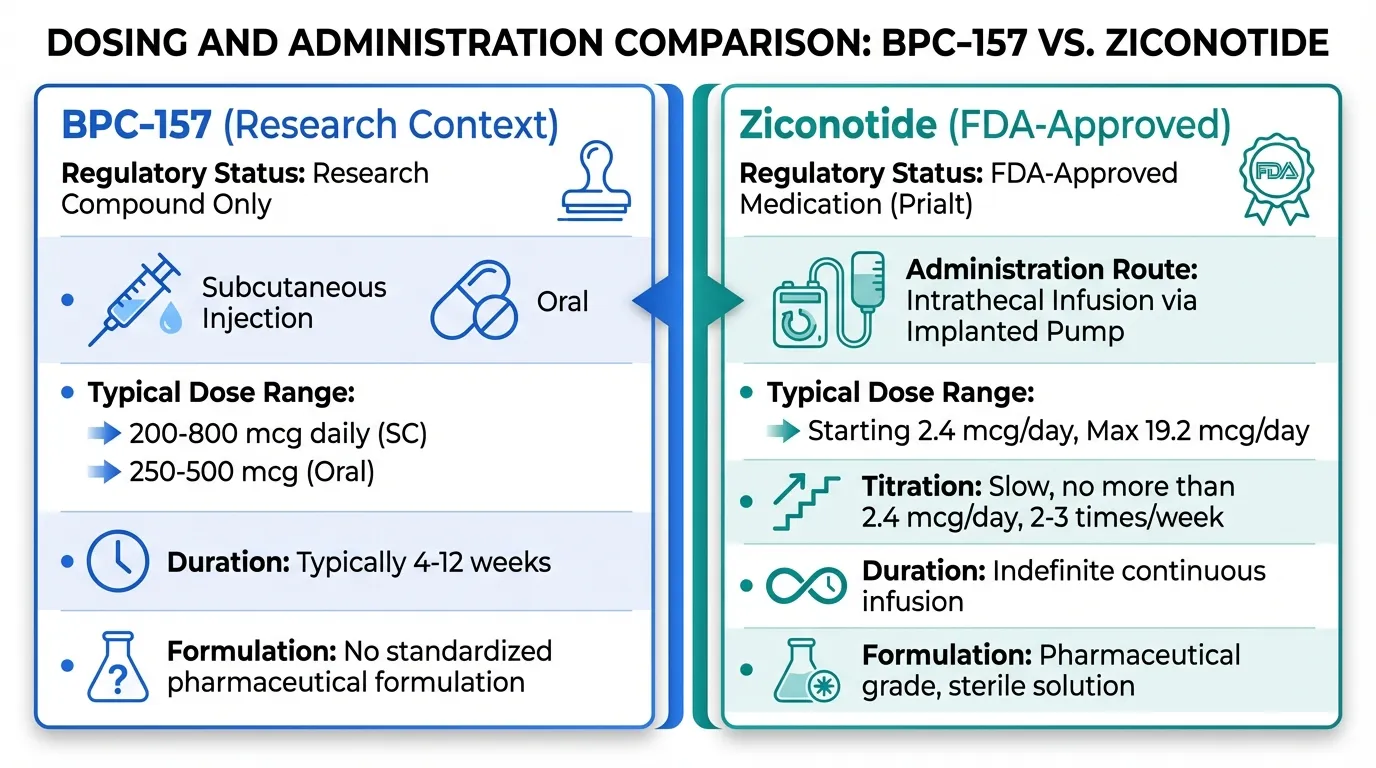
| Administration | Subcutaneous or intramuscular injection (most common research route). Oral administration studied in GI applications. No implanted device required. Simple self-administration. Research chemical without standardized pharmaceutical formulation. | Requires intrathecal delivery via surgically implanted programmable pump (SynchroMed system) or external microinfusion catheter. Cannot be given orally, subcutaneously, or intravenously. The most invasive peptide delivery route in clinical medicine. | BPC-157 |

Introduction#
BPC-157 and ziconotide represent two vastly different peptide approaches that intersect only in the broadest sense -- both are peptides investigated for conditions involving pain or tissue injury. Beyond that surface similarity, they differ in virtually every dimension: mechanism, evidence level, regulatory status, administration route, and therapeutic intent.
Ziconotide (Prialt) is an FDA-approved synthetic conopeptide that blocks N-type calcium channels in the spinal cord to provide potent analgesia for severe, refractory chronic pain. It requires intrathecal delivery via an implanted pump and has significant CNS side effects. BPC-157 is a preclinical gastric pentadecapeptide with broad tissue-healing properties demonstrated in dozens of animal models but virtually no human clinical data.
This comparison illustrates a useful contrast in peptide pharmacology: a thoroughly validated but narrowly applicable analgesic versus a broadly promising but clinically unvalidated healing peptide.
Mechanism of Action Comparison#
BPC-157#
BPC-157 (Body Protection Compound-157) is a 15-amino acid peptide derived from human gastric juice (a fragment of the protein BPC). Its mechanism involves multiple tissue repair pathways:
- Angiogenesis: Upregulates VEGF (vascular endothelial growth factor), promoting new blood vessel formation at injury sites
- Cell adhesion and migration: Activates FAK/paxillin signaling, promoting cell adhesion, spreading, and migration to wound sites
- Growth factor signaling: Enhances growth hormone receptor expression in tendon fibroblasts and other repair cells
- NOS modulation: Modulates nitric oxide synthase pathways for cytoprotection and vasodilation
- KRAS/MAPK: Activates cell proliferation pathways necessary for tissue regeneration
- GI protection: Protects and heals gastric and intestinal mucosa, consistent with its origin from gastric juice
BPC-157's mechanism is notable for its breadth -- it promotes healing across tendons, ligaments, muscle, bone, skin, GI tract, and even neural tissue in preclinical models. This pleiotropic activity suggests it acts on fundamental repair pathways rather than tissue-specific targets.
Ziconotide#
Ziconotide is a synthetic 25-amino acid peptide that is identical to omega-conotoxin MVIIA, a venom peptide from the cone snail Conus magus. Its mechanism is highly specific:
- N-type calcium channel blockade: Selectively antagonizes Cav2.2 (N-type) voltage-gated calcium channels located on presynaptic terminals of nociceptive neurons in the dorsal horn of the spinal cord
- Neurotransmitter inhibition: Blocks depolarization-evoked release of substance P, glutamate, and calcitonin gene-related peptide (CGRP) from pain-signaling afferents
- Spinal-level analgesia: Produces analgesia at the spinal cord level by interrupting pain signal transmission before it reaches the brain
- Non-opioid: Does not interact with opioid receptors, mu or otherwise. Produces no tolerance, physical dependence, or respiratory depression
Mechanistic Comparison#
| Feature | BPC-157 | Ziconotide |
|---|---|---|
| Origin | Human gastric juice fragment | Cone snail venom peptide |
| Size | 15 amino acids | 25 amino acids (3 disulfide bonds) |
| Mechanism | Multi-pathway tissue repair | Selective Cav2.2 calcium channel blockade |
| Target | Repair cells (fibroblasts, endothelium) | Nociceptive neurons in spinal dorsal horn |
| Effect | Tissue healing and regeneration | Pain signal blockade |
| Specificity | Broad/pleiotropic | Highly specific |
| Opioid interaction | None | None |
| Tolerance development | Not characterized | None observed |
Dosing Comparison#
BPC-157 Dosing#
No standardized human dosing exists. Research contexts include:
- Subcutaneous injection: Typically 200-800 mcg daily in research protocols, often near the site of injury
- Oral: Studied for GI applications. Animal doses extrapolate to roughly 250-500 mcg in humans
- Duration: Typically 4-12 weeks in research protocols
- No pharmaceutical formulation: Available only through research chemical suppliers without standardized quality
Ziconotide Dosing#
Established pharmaceutical dosing with FDA-approved labeling:
- Intrathecal infusion: Starting dose 2.4 mcg/day (0.1 mcg/hour), titrated slowly upward
- Maximum recommended dose: 19.2 mcg/day (0.8 mcg/hour)
- Titration: Increases of no more than 2.4 mcg/day, no more frequently than 2-3 times per week
- Delivery: Continuous infusion via SynchroMed programmable intrathecal pump or external microinfusion catheter
- Duration: Indefinite continuous infusion for chronic pain management
Side Effects Comparison#
BPC-157 Side Effects#
No systematic human safety data exists. Based on preclinical evidence:
- Animal tolerance: Excellent tolerance across species and dose ranges in preclinical studies. No dose-limiting toxicities reported in published literature
- Endogenous origin: As a fragment of a naturally occurring gastric protein, theoretical toxicity risk is considered low
- Unknown in humans: True side effect profile is completely unknown. No human safety trials have been conducted
- Theoretical concerns: Effects on tumor angiogenesis (VEGF upregulation) have been raised as a theoretical concern, though not demonstrated
Ziconotide Side Effects#
Well-characterized through clinical trials and post-marketing surveillance:
- Common CNS effects: Dizziness (47%), nausea (30%), confusion (33%), headache (15%), somnolence, nystagmus, abnormal gait, memory impairment
- Serious psychiatric effects: Depression, cognitive impairment, hallucinations, psychosis, suicidal ideation. FDA black box warning for severe psychiatric symptoms and neurological impairment
- Elevated CK: Creatine kinase elevation is common and should be monitored
- Meningitis risk: Intrathecal catheter carries infection risk
- Narrow therapeutic window: Effective doses are close to doses causing intolerable side effects
- Slow onset/offset: Both analgesia and adverse effects have a lag time, complicating dose titration
Research Evidence Comparison#
BPC-157 Research#
- Tendon healing: Multiple studies showing promotion of tendon outgrowth, cell survival, and migration. Enhanced growth hormone receptor expression in tendon fibroblasts. Restored biomechanics and motor function in eight tendon/ligament transection models
- GI protection: Extensive preclinical data in inflammatory bowel disease models, gastric ulcer healing, and mucosal protection
- Muscle/bone healing: Acceleration of fracture healing and muscle repair in animal models
- CNS effects: Neuroprotective and anxiolytic effects reported in preclinical studies
- Systematic reviews (2025): Reviews in orthopaedic sports medicine conclude "promising preclinical evidence but insufficient human data to recommend clinical use"
- Human data: One small study (n=12) in chronic knee pain showed 7/12 patients with relief lasting 6+ months after a single injection. No RCTs
Evidence level: Very low -- extensive animal data, virtually no human clinical evidence.
Ziconotide Research#
- Phase 3 trials: Multiple RCTs demonstrating significant pain reduction versus placebo in both cancer/AIDS-related pain and noncancer chronic pain
- Cancer pain (Staats et al., 2004): 53% of ziconotide patients achieved moderate-to-complete pain relief vs 18% placebo
- Chronic pain (Rauck et al., 2006): Significant pain reduction in noncancer chronic pain patients refractory to intrathecal morphine
- Long-term data: Extended follow-up studies confirm sustained efficacy without tolerance development
- FDA approval (2004): Approved as Prialt for intrathecal management of severe chronic pain in patients intolerant or refractory to other therapies
- No tolerance or dependence: Unlike opioids, chronic ziconotide use does not produce tolerance, physical dependence, or withdrawal
Evidence level: High -- FDA-approved with multiple phase 3 RCTs and post-marketing surveillance.
Key Differences Summary#
- Evidence level: Ziconotide is FDA-approved with phase 3 trial data. BPC-157 is preclinical with virtually no human evidence.
- Therapeutic intent: Ziconotide blocks pain signals. BPC-157 aims to heal damaged tissue.
- Administration: Ziconotide requires intrathecal delivery via implanted pump. BPC-157 uses simple subcutaneous injection.
- Side effects: Ziconotide has significant, well-characterized CNS side effects including psychiatric symptoms. BPC-157's side effects are unknown.
- Specificity: Ziconotide has a single, highly specific target (Cav2.2). BPC-157 has a broad, pleiotropic mechanism.
- Patient population: Ziconotide is reserved for severe refractory pain as a last-resort treatment. BPC-157 is investigated for common musculoskeletal injuries.
- Addictive potential: Neither has addictive potential. Ziconotide's non-opioid mechanism is a key clinical advantage.
Conclusion#
BPC-157 and ziconotide are not competing options for the same condition. They represent fundamentally different therapeutic strategies in peptide medicine -- tissue healing versus pain signal blockade -- with vastly different evidence levels and clinical contexts.
Ziconotide is a validated, FDA-approved analgesic that fills a critical niche for patients with severe, refractory chronic pain who have exhausted other options. Its significant side effect profile and invasive intrathecal delivery limit its use to the most severe cases, but for those patients, it provides non-addictive, tolerance-free pain relief that no opioid can match.
BPC-157 is a scientifically intriguing healing peptide with broad preclinical promise. Its ability to promote tissue repair across multiple organ systems through pleiotropic mechanisms is unique among investigated peptides. However, it remains a research compound without human safety or efficacy data sufficient to support clinical recommendations.
The two peptides illustrate the spectrum of peptide therapeutics development: from FDA-approved specialty medication (ziconotide) to promising preclinical research compound (BPC-157).
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Severe Refractory Chronic Pain
Ziconotide
Ziconotide is FDA-approved specifically for chronic severe pain refractory to other treatments. It is the only non-opioid intrathecal analgesic with regulatory approval and is indicated when all other pain management strategies have failed.
Tissue Healing Research
BPC-157
BPC-157 has the broadest preclinical evidence for tissue repair across tendons, ligaments, muscle, bone, and GI mucosa. Its pleiotropic healing mechanism is unique among peptides studied for injury recovery.
Non-Addictive Pain Management
Ziconotide
Ziconotide does not bind opioid receptors and produces no tolerance, dependence, or addiction. It is the evidence-based non-opioid option for intractable pain. Development of tolerance is not observed with chronic use.
Musculoskeletal Injury Recovery
BPC-157
Preclinical data specifically in tendon transection, ligament repair, and muscle healing models is extensive. BPC-157 promoted tendon outgrowth, cell survival, and migration in multiple injury models and enhanced growth hormone receptor expression in tendon fibroblasts.
Regulatory-Approved Treatment
Ziconotide
Ziconotide (Prialt) is the only option with FDA approval, phase 3 trial data, established manufacturing standards, and ongoing post-marketing surveillance. BPC-157 has no regulatory approval anywhere.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About BPC-157 vs Ziconotide: Healing Peptide vs Approved Pain Medication
Which is better, BPC-157 or Ziconotide?
BPC-157 and ziconotide serve fundamentally different purposes and represent opposite ends of the evidence spectrum. Ziconotide is an FDA-approved medication with rigorous clinical trial data, but it is reserved for severe refractory pain requiring intrathecal delivery and carries significant CNS side effects. BPC-157 is a preclinical healing peptide with broad tissue repair properties but essentially no human clinical data. They are not interchangeable or directly competitive. Ziconotide trea... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between BPC-157 and Ziconotide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to Ziconotide; Side Effect Profile: advantage goes to BPC-157. 1 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Ziconotide over BPC-157?
For the scenario of "Severe Refractory Chronic Pain," research data suggests Ziconotide may be more relevant. Ziconotide is FDA-approved specifically for chronic severe pain refractory to other treatments. It is the only non-opioid intrathecal analgesic with regulatory approval and is indicated when all ot.... This is based on currently available evidence and individual circumstances may differ.
How do BPC-157 and Ziconotide differ in their mechanisms of action?
BPC-157: Pentadecapeptide (15 amino acids) derived from human gastric juice. Pleiotropic healing mechanism involving upregulation of VEGF (angiogenesis), FAK/paxillin (cell adhesion), growth hormone recepto.... Ziconotide: Synthetic 25-amino acid conopeptide (derived from Conus magus cone snail venom). Selectively blocks N-type voltage-gated calcium channels (Cav2.2) in the spinal cord dorsal horn. Inhibits neurotran....
Which has fewer side effects, BPC-157 or Ziconotide?
In terms of side effects and tolerability, the advantage goes to BPC-157. BPC-157: No systematic human safety data. Preclinical studies report excellent tolerance with no observed toxicity. As a gastric peptide fragment, it is exp.... Ziconotide: Narrow therapeutic window with significant CNS side effects including dizziness, nausea, confusion, memory impairment, and nystagmus. Serious psych....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.