Tirzepatide Cost Canada

Introduction#
Tirzepatide has emerged as one of the most consequential advances in metabolic pharmacotherapy in recent years, demonstrating weight loss and glycemic efficacy that surpasses all previously available GLP-1 receptor agonists. Marketed as Mounjaro for type 2 diabetes and Zepbound for chronic weight management, this dual-action peptide developed by Eli Lilly has generated enormous patient demand -- and equally significant questions about affordability and access.
For Canadians, navigating the cost landscape for tirzepatide involves a distinctly different set of considerations than those faced by patients in the United States. Canada's hybrid public-private pharmaceutical coverage system, provincial formulary decision-making processes, and regulatory timeline create a pricing and access environment that requires careful analysis. Following Health Canada's approval of Mounjaro for type 2 diabetes in 2024, patients and prescribers alike have been seeking clarity on what tirzepatide actually costs, who pays for it, and how coverage is evolving.
This guide provides a detailed examination of tirzepatide pricing in the Canadian context, compares costs against alternative GLP-1-based therapies, outlines the current state of insurance coverage, and evaluates what the clinical evidence says about the value proposition of this medication relative to its cost.
What Is Tirzepatide?#
Tirzepatide is a 39-amino acid synthetic peptide that functions as a dual GIP/GLP-1 receptor agonist -- meaning it simultaneously activates receptors for both glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1). This dual-receptor mechanism distinguishes it from earlier incretin-based therapies such as semaglutide (Ozempic, Wegovy) and liraglutide (Victoza, Saxenda), which target only the GLP-1 receptor.
The pharmacological rationale behind engaging both receptors is that GIP and GLP-1 activate partially non-overlapping metabolic pathways. GLP-1 receptor agonism enhances glucose-dependent insulin secretion, suppresses glucagon, delays gastric emptying, and signals satiety through hypothalamic and brainstem pathways. GIP receptor agonism contributes additional appetite-suppressive signaling through distinct central nervous system circuits, modulates adipose tissue metabolism, and supports beta-cell function through complementary mechanisms. The combined effect produces greater glycemic control and weight loss than either pathway achieves alone.
Tirzepatide incorporates a C20 fatty diacid modification that enables albumin binding and extends its plasma half-life to approximately five days, supporting once-weekly subcutaneous administration. It is engineered with approximately 5-fold selectivity for the GIP receptor over the GLP-1 receptor, a design choice reflecting preclinical data suggesting that a GIP-dominant profile optimizes the balance between efficacy and gastrointestinal tolerability.
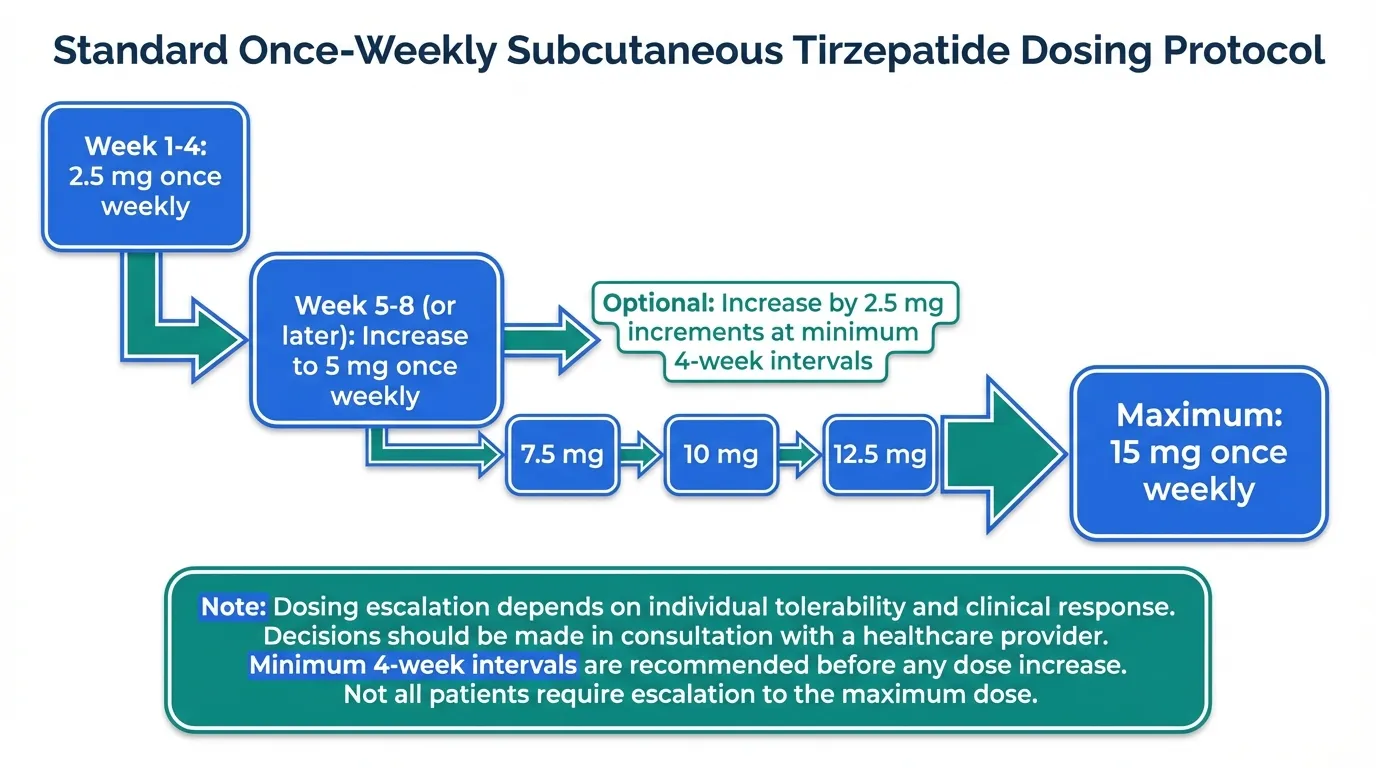
Available formulations and doses: Tirzepatide is supplied as single-dose, pre-filled auto-injector pens for subcutaneous injection. Six dose strengths are available: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, and 15 mg. The standard dosing protocol initiates treatment at 2.5 mg once weekly for four weeks, then increases to 5 mg once weekly. Subsequent dose escalations of 2.5 mg increments occur at minimum four-week intervals, based on individual tolerability and clinical response, up to a maximum of 15 mg weekly.
Regulatory status in Canada: Health Canada approved Mounjaro (tirzepatide) for the treatment of type 2 diabetes mellitus in adults in 2024, making it available by prescription as an adjunct to diet and exercise for glycemic improvement. As of the time of writing, the weight management indication (marketed as Zepbound in the United States) has not yet received separate Health Canada approval, though regulatory review processes are underway. This distinction has important implications for insurance coverage, as discussed below.
Manufacturer: Eli Lilly and Company.
Current Pricing in Canada#
Understanding tirzepatide's cost in Canada requires examining multiple price points, since the amount a patient actually pays depends on their insurance status, province of residence, and the specific indication for which the medication is prescribed.
List Pricing#
The list price for tirzepatide in Canada varies by dose strength. A four-week supply (four auto-injector pens) typically falls in the range of CAD $350-$550 depending on the dose, with lower doses at the lower end and the 15 mg dose at the upper end. On a monthly basis, patients can expect approximate costs in the following ranges:
| Dose | Approximate Monthly Cost (CAD) |
|---|---|
| 2.5 mg (initiation) | $350 - $400 |
| 5 mg | $400 - $450 |
| 7.5 mg | $420 - $470 |
| 10 mg | $450 - $500 |
| 12.5 mg | $480 - $530 |
| 15 mg | $500 - $550 |
These figures represent approximate retail pharmacy pricing and may vary between pharmacies, provinces, and over time as market conditions evolve. Patients should confirm current pricing with their dispensing pharmacy.
Comparison to US Pricing#
The pricing difference between Canada and the United States is substantial. In the US, Mounjaro carries a list price of approximately USD $1,000-$1,200 per month, and Zepbound is priced similarly. Even accounting for the exchange rate, Canadian pricing for tirzepatide represents a meaningful discount relative to US list prices -- a pattern consistent with Canada's Patented Medicine Prices Review Board (PMPRB) regulatory framework, which benchmarks Canadian drug prices against a basket of comparator countries.
However, it is important to note that US list prices are often offset by manufacturer rebates, insurance negotiations, and patient savings programs that reduce the actual out-of-pocket cost for many American patients. The effective price comparison between the two countries is therefore more nuanced than list prices alone suggest.
The Provincial Variation Factor#
Canada does not have a single national drug price. While federal mechanisms like the PMPRB set ceilings, actual pricing and availability are influenced by provincial pharmaceutical purchasing arrangements. Provinces that participate in the pan-Canadian Pharmaceutical Alliance (pCPA) negotiate prices collectively for publicly funded drug programs, and the negotiated price is typically confidential and lower than the list price.
For patients relying on provincial public drug programs, the relevant question is not the list price but whether the province has listed tirzepatide on its formulary at all -- a coverage question explored in the next section.
Insurance and Coverage Options#
The Canadian pharmaceutical coverage landscape is fragmented across public provincial programs, employer-sponsored private insurance, and individual out-of-pocket payment. Each channel presents different considerations for tirzepatide access.
Provincial Public Drug Programs#
Provincial drug formulary decisions for tirzepatide are evolving. The Canadian Drug Expert Committee (CDEC), which advises the Canadian Agency for Drugs and Technologies in Health (CADTH), reviews submitted evidence and issues reimbursement recommendations that provinces may choose to follow.
As of early 2026, provincial formulary coverage for Mounjaro (tirzepatide for type 2 diabetes) is in various stages across the country:
- Some provinces have initiated coverage for tirzepatide under their public drug programs, typically with clinical criteria restrictions such as documented inadequate glycemic control on metformin or other first-line agents, or specific HbA1c thresholds.
- Other provinces are still completing their review processes or awaiting pCPA pricing negotiations to conclude before making listing decisions.
- Coverage criteria, where they exist, generally require the prescribing physician to demonstrate that the patient meets specific clinical parameters -- often including a minimum HbA1c level, prior trial of metformin or sulfonylurea therapy, and sometimes BMI thresholds when weight-related metabolic benefit is part of the clinical rationale.
Patients should contact their provincial drug plan directly or consult with their pharmacist to determine current formulary status in their jurisdiction. Coverage landscapes in this therapeutic class are shifting relatively rapidly as provinces respond to CADTH recommendations and complete pricing negotiations.
The Weight Management Indication Gap#
A critical distinction for Canadian patients: because only the type 2 diabetes indication (Mounjaro) has received Health Canada approval to date, there is currently no regulatory basis for public formulary coverage of tirzepatide specifically for weight management in individuals without diabetes. Patients seeking tirzepatide primarily for obesity treatment face the following landscape:
- Provincial programs generally do not cover medications for indications that lack Health Canada approval
- Off-label prescribing is legally permissible at physician discretion, but public drug program reimbursement for off-label use is uncommon
- Some private insurers may cover off-label use based on supporting clinical evidence, but this is plan-dependent and often requires prior authorization
This gap means that, for the time being, the majority of Canadian patients using tirzepatide for weight management without a concurrent type 2 diabetes diagnosis will likely pay out of pocket unless they have private insurance that covers the off-label use or the prescriber documents a covered indication.
Private Insurance Coverage#
Employer-sponsored and individual private drug plans in Canada represent the most variable component of the coverage landscape. Coverage for tirzepatide through private insurance depends on:
- Formulary inclusion: Whether the specific plan has added tirzepatide to its covered medication list
- Prior authorization requirements: Many plans require documentation of prior therapy failure, specific diagnostic criteria, or specialist involvement before approving coverage
- Tiered coverage: Some plans cover tirzepatide but at a higher cost-sharing tier, meaning greater co-pays or co-insurance for the patient
- Annual or lifetime maximums: Some plans cap specialty medication spending, which can affect long-term tirzepatide affordability
Patients with private coverage should request a pre-determination or prior authorization before filling their first prescription to understand their actual out-of-pocket exposure. Pharmacists and prescribers can assist with the documentation required for these submissions.
Manufacturer Patient Support Programs#
Eli Lilly operates patient support programs in Canada that may provide financial assistance, co-pay support, or other access mechanisms for eligible patients. These programs typically have eligibility criteria based on insurance status and income, and the specific benefits available can change over time. Patients and prescribers can contact Eli Lilly's Canadian patient support services for current program details.
How Tirzepatide Compares on Cost (vs Ozempic, Wegovy)#
Placing tirzepatide's cost in context requires comparison against the primary alternative GLP-1-based therapies available in Canada: semaglutide, marketed as Ozempic for type 2 diabetes and Wegovy for chronic weight management.
Direct Cost Comparison#
| Medication | Indication | Approximate Monthly Cost (CAD) | Receptor Target |
|---|---|---|---|
| Mounjaro (tirzepatide) 5-15 mg | Type 2 Diabetes | $400 - $550 | Dual GIP/GLP-1 |
| Ozempic (semaglutide) 0.5-2 mg | Type 2 Diabetes | $250 - $350 | GLP-1 |
| Wegovy (semaglutide) 2.4 mg | Weight Management | $400 - $500 | GLP-1 |
| Saxenda (liraglutide) 3 mg | Weight Management | $350 - $450 | GLP-1 |
On a straightforward monthly cost basis, tirzepatide at its maintenance doses is priced at a premium relative to Ozempic, though the differential narrows when compared against Wegovy. This pricing reflects tirzepatide's positioning as a next-generation therapy with demonstrated superiority over semaglutide in head-to-head clinical trials.
Cost-Per-Unit-of-Efficacy Considerations#
Raw monthly cost comparisons do not capture the full economic picture. When evaluated on a cost-per-percentage-point-of-weight-loss or cost-per-unit-of-HbA1c-reduction basis, the calculus shifts:
- Tirzepatide 15 mg produces approximately 20.9% body weight loss at 72 weeks (SURMOUNT-1), compared to semaglutide 2.4 mg producing approximately 15-17% (STEP trials). This represents roughly 30-50% greater weight loss efficacy.
- Tirzepatide produces HbA1c reductions of 2.0-2.3% versus semaglutide 1 mg producing approximately 1.8% (SURPASS-2). In that same head-to-head trial, tirzepatide 15 mg achieved a 2.46% HbA1c reduction compared to semaglutide 1 mg at 1.86%.
If the monthly cost premium for tirzepatide over Ozempic is in the range of 40-60%, but the efficacy advantage is 30-50% for weight loss and roughly 25-30% for glycemic control, the cost-effectiveness ratio narrows considerably. For patients who require greater metabolic improvement than semaglutide alone provides, tirzepatide may represent comparable or even superior value per dollar of therapeutic benefit.
Formulary and Coverage Parity#
An additional practical consideration is that Ozempic has been available in Canada longer than Mounjaro and has more established provincial formulary coverage and private insurance inclusion. This means that, independent of list price, Ozempic may have lower actual out-of-pocket cost for many patients simply because coverage infrastructure is more mature. As tirzepatide formulary decisions progress, this accessibility gap is expected to narrow.
Clinical Efficacy (What You Get for the Cost)#
Evaluating the value proposition of any medication requires understanding what clinical benefit the expenditure delivers. Tirzepatide's evidence base is extensive and derived from two major Phase 3 clinical trial programs.
Weight Loss: The SURMOUNT Program#
The SURMOUNT clinical trial program evaluated tirzepatide for chronic weight management in adults with obesity or overweight with at least one weight-related comorbidity:
- SURMOUNT-1: The landmark trial enrolled 2,539 adults without diabetes. At 72 weeks, the 15 mg dose produced a mean body weight reduction of 20.9% from baseline (approximately 24 kg in a participant weighing 105 kg at baseline). The 10 mg dose achieved 21.4%, and the 5 mg dose achieved 16.0%. These results exceeded anything previously demonstrated in pharmacological obesity treatment trials.
- SURMOUNT-2: Evaluated tirzepatide in 938 adults with obesity and type 2 diabetes, demonstrating 14.7% weight loss at the 15 mg dose over 72 weeks -- a population that historically shows less weight loss response due to metabolic adaptations associated with diabetes and concurrent glucose-lowering medications.
- SURMOUNT-3 and SURMOUNT-4: Examined tirzepatide following intensive lifestyle intervention and the effects of treatment continuation versus discontinuation, respectively, further characterizing the durability and clinical context of weight loss benefits.
The clinical significance of these weight loss magnitudes is substantial. Weight reductions exceeding 10-15% are associated with improvements in or resolution of obesity-related comorbidities including obstructive sleep apnea, osteoarthritis symptoms, cardiovascular risk factors, and non-alcoholic fatty liver disease. The 20.9% mean reduction observed with tirzepatide 15 mg approaches the range historically achievable only through bariatric surgery.
Glycemic Control: The SURPASS Program#
For type 2 diabetes, the SURPASS program provided comprehensive evidence across multiple comparator arms:
- SURPASS-1: Tirzepatide monotherapy versus placebo demonstrated HbA1c reductions of 1.87-2.07% across dose groups
- SURPASS-2: The pivotal head-to-head comparison against semaglutide 1 mg showed tirzepatide superiority at all three doses, with the 15 mg dose achieving a 2.46% HbA1c reduction versus 1.86% for semaglutide -- a statistically significant and clinically meaningful difference
- SURPASS-3: Tirzepatide versus insulin degludec demonstrated superior glycemic control with weight loss rather than weight gain
- SURPASS-4: Tirzepatide versus insulin glargine in patients with increased cardiovascular risk showed superior HbA1c reduction and cardiovascular safety
- SURPASS-5: Tirzepatide as add-on to insulin glargine demonstrated additional glycemic benefit
Across the SURPASS program, tirzepatide consistently achieved HbA1c reductions in the range of 2.0-2.3% at the 10 mg and 15 mg doses, placing it at the top of available non-insulin glucose-lowering therapies. A substantial proportion of patients achieved HbA1c targets below 7.0% and even below 5.7% (the normal range), outcomes that had been uncommon with previous pharmacological approaches.
Safety and Tolerability Profile#
The most common adverse effects with tirzepatide are gastrointestinal in nature: nausea, diarrhea, decreased appetite, vomiting, and constipation. These events are typically mild to moderate, occur most frequently during dose escalation periods, and diminish over time as patients reach their maintenance dose. The four-week dose escalation protocol is specifically designed to mitigate these effects.
Notably, despite producing greater weight loss than semaglutide, tirzepatide's gastrointestinal tolerability in clinical trials was broadly comparable -- a finding attributed to the dual-receptor mechanism distributing appetite-suppressive signaling across GIP and GLP-1 pathways rather than relying solely on GLP-1-mediated effects.
Serious adverse events are uncommon but include the class-wide warnings applicable to all GLP-1-based therapies: risk of pancreatitis, gallbladder events, and a precautionary contraindication in patients with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2.
Access and Availability#
Beyond cost and insurance coverage, practical access to tirzepatide in Canada involves several additional considerations.
Prescription Requirements#
Tirzepatide requires a prescription from a licensed physician or, in provinces where applicable, a nurse practitioner with prescribing authority. There is no over-the-counter or direct-to-consumer pathway. Most prescriptions originate from:
- Family physicians and general practitioners: Increasingly comfortable prescribing GLP-1 and dual-agonist therapies for type 2 diabetes management
- Endocrinologists: Commonly involved when patients have complex diabetes management needs or have not achieved adequate control with first-line therapies
- Obesity medicine specialists: For weight management indications, where available and where the regulatory landscape permits
Pharmacy Supply and Distribution#
Tirzepatide is a cold-chain medication requiring refrigeration prior to first use (auto-injector pens may be kept at room temperature for up to 21 days once in use). It is dispensed through community pharmacies and specialty pharmacies across Canada. During periods of high demand, supply constraints have occasionally affected availability of specific dose strengths -- a pattern observed with other medications in this therapeutic class, most notably semaglutide.
Patients initiating therapy should discuss supply continuity with their pharmacist, particularly during the dose escalation phase where interruptions could disrupt the titration schedule.
Compounding and Grey Market Considerations#
The high cost and access barriers for branded tirzepatide have created demand for compounded or imported alternatives. It is important for Canadian patients to be aware that:
- Health Canada regulates pharmaceutical imports, and purchasing prescription medications from unregulated international sources carries safety and legal risks
- Compounded tirzepatide from non-Eli Lilly sources has not been evaluated for purity, potency, or sterility through the same regulatory processes as the approved product
- Patients should discuss all medication sourcing with their prescribing physician and dispensing pharmacist
Looking Ahead: Anticipated Developments#
Several developments may affect tirzepatide access and cost in Canada over the coming months and years:
- Weight management approval: A separate Health Canada approval for the weight management indication would open pathways for formulary coverage specific to obesity treatment
- Expanding provincial coverage: As pCPA negotiations conclude and provinces implement coverage decisions, public drug program access is expected to broaden
- Biosimilar and competitive dynamics: While tirzepatide patent protection extends for several more years, the growing competitive landscape of dual and triple receptor agonists may exert downward pricing pressure over time
- Oral formulations: Eli Lilly has oral tirzepatide in clinical development, which could alter the cost and convenience profile if approved
Conclusion#
Tirzepatide represents a genuine advance in metabolic therapeutics, offering weight loss efficacy that approaches surgical outcomes and glycemic control that surpasses all previously available non-insulin medications. For Canadian patients, the question is not whether this medication is clinically valuable -- the SURPASS and SURMOUNT trial data leave little doubt on that point -- but whether the current cost and coverage landscape makes it accessible.
At approximately CAD $400-$550 per month at maintenance doses, tirzepatide is priced at a premium over established alternatives like semaglutide (Ozempic), though the differential is partially offset by its superior efficacy profile. Provincial formulary coverage is expanding but remains incomplete, and the absence of a Health Canada weight management approval creates a significant access gap for patients seeking tirzepatide primarily for obesity treatment.
Patients considering tirzepatide should engage proactively with their healthcare providers and pharmacists to understand their specific coverage situation, explore manufacturer patient support programs, and evaluate whether the clinical benefits justify the out-of-pocket cost relative to available alternatives. As the Canadian coverage landscape continues to evolve, access is expected to improve -- but for many patients, affordability remains the primary barrier to what is otherwise one of the most effective metabolic medications currently available.
This article is intended for informational purposes only and does not constitute medical or financial advice. Drug pricing, insurance coverage, and formulary status are subject to change. Patients should consult with their healthcare provider and pharmacist for personalized guidance.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:

{kind=link}
Frequently Asked Questions About Tirzepatide Cost Canada
What does this article cover?
How Much Does Tirzepatide Cost in Canada? — part of the GLP-1 Pricing & Access content cluster. This article is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Tirzepatide. Key context: Tirzepatide (Referenced in cluster "GLP-1 Pricing & Access"). Each peptide is discussed based on available research evidence.
Is this article based on research evidence?
This article draws on published research data and publicly available information about the peptides discussed. It is intended for educational purposes only. Pricing and availability may vary by region and change over time.
What is Tirzepatide and why is it significant?
Tirzepatide is a peptide discussed in this article because: Referenced in cluster "GLP-1 Pricing & Access". For a complete profile of Tirzepatide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Compounded Semaglutide Cost Guide 2026: Prices, Pharmacies & What to Expect
A deep dive into compounded semaglutide pricing in 2026, covering 503A and 503B pharmacy costs, telehealth platform pricing, dose-by-dose monthly breakdowns, and how to evaluate compounding pharmacy quality.

Semaglutide Vs Tirzepatide Cost
Semaglutide vs Tirzepatide: Cost Comparison — part of the GLP-1 Pricing & Access content cluster.

Living on GLP-1 Medications: Diet, Exercise, and Lifestyle Adjustments
Practical lifestyle guidance for people on GLP-1 receptor agonist medications, covering diet optimization, exercise strategies, managing reduced appetite, protein intake, hydration, and building sustainable habits while on semaglutide, tirzepatide, or liraglutide.
You Might Also Like
Related content you may find interesting