Peptides for Depression and Anxiety: From Approved Treatments to Research Compounds

Introduction#
Depression and anxiety disorders are among the most prevalent medical conditions worldwide, yet current treatments have significant limitations. Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) require 4-6 weeks for therapeutic onset, produce sexual dysfunction and other side effects in many patients, and fail to achieve remission in approximately one-third of patients. Benzodiazepines for anxiety provide rapid relief but carry risks of dependence, cognitive impairment, and tolerance.
Peptide-based approaches to depression and anxiety offer fundamentally different mechanisms from conventional monoamine-targeting drugs. From NMDA receptor modulation (rapastinel) to GABA enhancement without sedation (selank) to endogenous stress-resilience pathways (neuropeptide Y), peptides address neural circuits and molecular targets that traditional antidepressants do not reach.
This guide examines peptides with research profiles relevant to depression and anxiety, spanning the spectrum from discontinued clinical candidates to compounds approved in Russia but not the West.
Important note: No peptide in this guide is FDA-approved for depression or anxiety in the United States. Two (selank and semax) are approved in Russia. All applications described are investigational or based on non-US regulatory frameworks.
1. Selank#
Evidence Level: Approved in Russia; limited Western clinical data Primary Mechanism: GABA modulation, serotonin metabolism, anti-inflammatory FDA Status: Not approved in the US; approved in Russia as an anxiolytic
Selank is a synthetic heptapeptide analog of tuftsin (an endogenous immunomodulatory tetrapeptide) developed at the Institute of Molecular Genetics of the Russian Academy of Sciences. It is approved in Russia for generalized anxiety disorder and has been studied for both anxiolytic and nootropic effects.
Mechanism of Action#
Selank's anxiolytic mechanism involves multiple neurotransmitter systems:
- GABAergic enhancement: Modulates GABA-A receptor signaling, enhancing inhibitory neurotransmission without the direct benzodiazepine-site binding that causes sedation and dependence
- Serotonin metabolism: Influences serotonin metabolism and the expression of serotonin-related genes in the brain
- Enkephalin stabilization: Inhibits enkephalinase, the enzyme that degrades endogenous opioid peptides (enkephalins), thereby prolonging the activity of the body's natural anxiolytic system
- Anti-inflammatory: Reduces neuroinflammation through modulation of IL-6, TNF-alpha, and other cytokines -- relevant because neuroinflammation is increasingly recognized as a contributor to depression and anxiety
- BDNF expression: Increases brain-derived neurotrophic factor expression, supporting neuroplasticity
Research Findings#
- Anxiolytic efficacy: Clinical studies in Russia showed anxiolytic effects comparable to low-dose benzodiazepines, without the sedation, cognitive impairment, or dependence risk
- Unpredictable chronic stress model: Selank enhanced the effects of diazepam in reducing anxiety behaviors in chronically stressed rats, suggesting complementary mechanisms
- Cognitive preservation: Unlike benzodiazepines, selank does not impair memory or cognitive function -- it may actually enhance them
- No dependence: No evidence of tolerance, physical dependence, or withdrawal effects in clinical use
- Rapid onset: Anxiolytic effects observed within minutes of intranasal administration
Administration#
- Route: Intranasal spray (0.15% solution)
- Dose: 75-450 mcg per administration, typically 2-3 times daily
- Duration: 14-day courses, repeated as needed
Important Considerations#
Western-standard RCTs for selank are limited. Most clinical data comes from Russian studies, which may not meet Western regulatory standards for methodology and reporting. The peptide is not FDA-approved, and its safety profile, while favorable in Russian clinical experience, has not been validated through FDA-standard trials.
2. Semax#
Evidence Level: Approved in Russia; limited Western clinical data Primary Mechanism: BDNF/NGF modulation, monoaminergic neurotransmission FDA Status: Not approved in the US; approved in Russia for stroke and cognitive enhancement
Semax is a synthetic heptapeptide analog of the ACTH(4-10) fragment that has been approved in Russia since the 1990s. While primarily indicated for stroke recovery and cognitive enhancement, semax's mechanisms are directly relevant to depression and anxiety through neurotrophin modulation and monoaminergic effects.
Mechanism of Action#
- BDNF and NGF upregulation: Increases expression of brain-derived neurotrophic factor and nerve growth factor, both of which are implicated in depression pathophysiology (BDNF is reduced in depressed patients and increased by effective antidepressants)
- Dopaminergic modulation: Enhances dopaminergic neurotransmission, relevant to anhedonia (loss of pleasure) in depression
- Serotonergic effects: Modulates serotonin pathways, though the mechanism differs from SSRIs
- Neuroprotection: Reduces oxidative stress and neuroinflammation in brain tissue
- No cortisol stimulation: Despite being derived from ACTH, semax does not stimulate adrenal cortisol production -- critical for psychiatric applications where HPA axis dysfunction is common
Research Findings#
- Default mode network: Functional MRI studies showed increased activation in the brain's default mode network in semax-treated groups, suggesting effects on the neural circuits involved in mood and self-referential processing
- Stress resilience: Animal studies demonstrated antidepressant-like effects and reduced behavioral responses to chronic stress
- Cognitive-mood interaction: Semax's cognitive-enhancing effects may indirectly benefit depression through improved executive function and attention
- Decades of clinical use: Widespread use in Russian clinical practice for neurological and cognitive indications
Administration#
- Route: Intranasal spray (0.1% and 1% solutions)
- Dose: 200-600 mcg daily, divided into 2-3 administrations
- Duration: Typically 10-14 day courses
Important Considerations#
Semax is not specifically approved or extensively studied for depression as a primary indication, even in Russia. Its antidepressant-relevant mechanisms (BDNF upregulation, monoaminergic modulation) are inferred from its broader neurological profile. Western clinical data is limited. For a direct comparison with another nootropic peptide, see Dihexa vs Semax.
3. Rapastinel (GLYX-13) -- Discontinued#
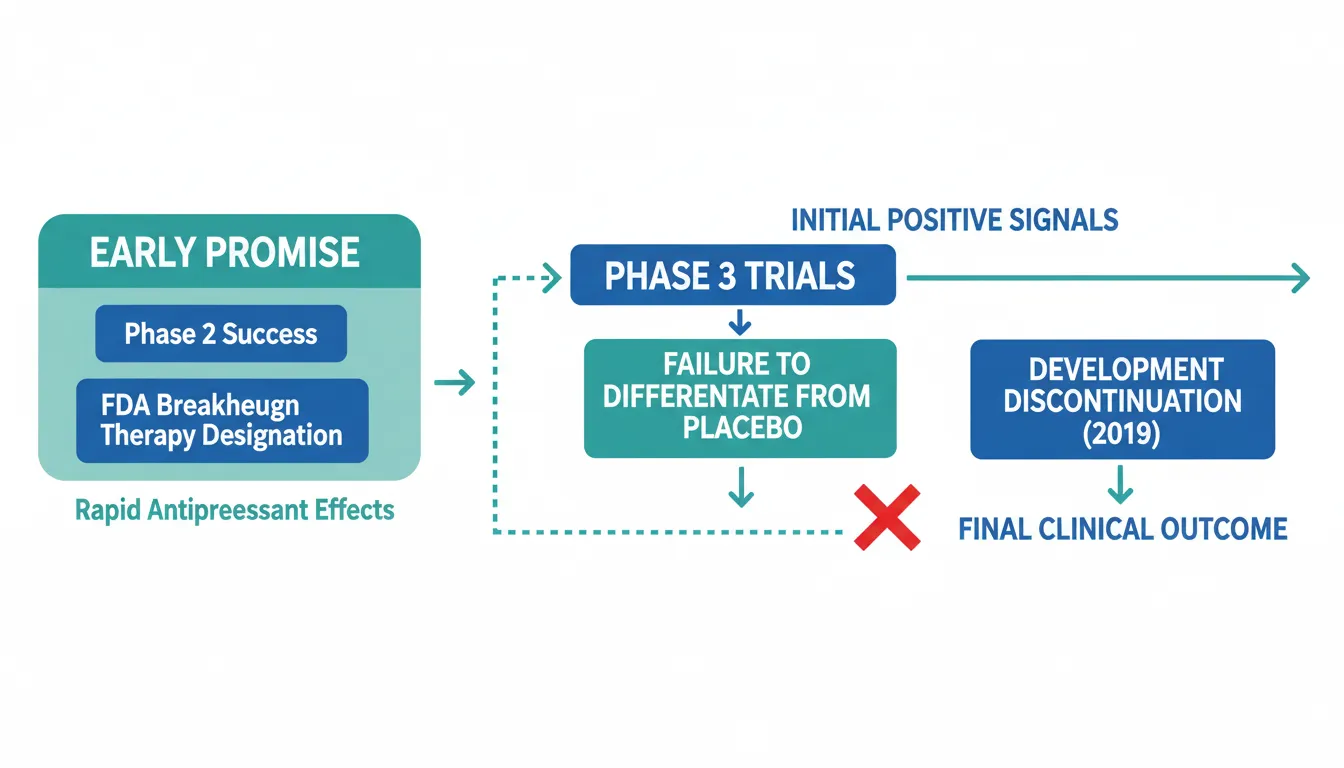
Evidence Level: Phase 3 (failed); FDA Breakthrough Therapy designation Primary Mechanism: NMDA glycine-site partial agonist FDA Status: Development discontinued after phase 3 failure (2019)
Rapastinel represents one of the most instructive stories in peptide antidepressant development. This amidated tetrapeptide modulates the NMDA receptor -- the same target class as ketamine -- and received FDA Breakthrough Therapy designation based on promising phase 2 data showing rapid-onset antidepressant effects without ketamine's dissociative side effects.
Mechanism of Action#
- NMDA glycine-site partial agonism: Enhances NMDA receptor activity at the glycine modulatory site, increasing synaptic plasticity
- BDNF/mTOR signaling: Activates the same downstream pathways as ketamine (BDNF release, mTOR activation) that are thought to underlie rapid antidepressant effects
- Metaplasticity: Produces long-lasting changes in the capacity for synaptic plasticity in the prefrontal cortex and hippocampus
- No dissociation: Unlike ketamine, rapastinel does not produce dissociative, psychotomimetic, or cognitive-impairing effects
Research Findings#
- Phase 2 success: Single IV doses of 5-10 mg/kg produced significant antidepressant effects within 24 hours as adjunctive therapy, sustained for 7+ days
- Phase 3 failure: All three pivotal phase 3 trials (2019) failed to differentiate from placebo on primary endpoints, likely due to high placebo response rates
- Safety profile: Remarkably well tolerated -- no dissociation, no abuse potential, no cognitive impairment
- Legacy: Spurred development of next-generation NMDA modulators including zelquistinel (an oral compound)
Lessons Learned#
Rapastinel's story highlights two critical challenges in depression drug development: (1) the placebo response problem, where placebo response rates in depression trials can reach 30-40%, making it difficult for active drugs to achieve statistical separation; and (2) the translation gap between early-phase efficacy signals and definitive phase 3 proof. For a detailed comparison, see Nemifitide vs Rapastinel.
4. Nemifitide (INN-00835) -- Stalled Development#
Evidence Level: Phase 2/3 (mixed results); development stalled Primary Mechanism: Multi-receptor binding (5-HT2A, NPY1, MC4/5) FDA Status: Not approved; development by Tetragenex/Innapharma stalled
Nemifitide is a synthetic pentapeptide structurally related to melanocyte-inhibiting factor (MIF-1) that showed rapid-onset antidepressant effects in early clinical studies. It has been administered to over 430 patients across 12 clinical trials.
Mechanism of Action#
- Multi-receptor binding: Antagonist at 5-HT2A receptors, plus binding to NPY1, bombesin, and MC4/MC5 receptors at micromolar concentrations
- Blood-brain barrier penetration: Crosses the BBB despite being a peptide
- Very short half-life with sustained effects: Plasma half-life of only 15-30 minutes, yet antidepressant effects persist for weeks -- suggesting induction of neuroplastic changes rather than continuous receptor occupancy
- Exact mechanism unclear: The precise pathway linking its multi-receptor binding to antidepressant effects has not been fully elucidated
Research Findings#
- Rapid onset: Antidepressant effects observed within 48 hours, with peak effect at approximately 1 week
- Treatment-refractory depression: Open-label study showed meaningful response in severely depressed, treatment-refractory patients
- Excellent tolerability: Few to no side effects reported across 430+ patients
- Mixed controlled data: Phase 2 RCT comparing 30 mg/d and 45 mg/d to placebo showed mixed results
- No definitive phase 3: Never completed a definitive phase 3 program
Important Considerations#
Nemifitide's development has been stalled for years. The compound remains scientifically interesting -- particularly its very short half-life producing sustained effects -- but the lack of a definitive phase 3 trial means its efficacy cannot be reliably assessed. The company (Tetragenex) does not appear to be actively pursuing development.
5. Neuropeptide Y (NPY)#
Evidence Level: Well-characterized biology; limited therapeutic development Primary Mechanism: Endogenous stress-resilience peptide; anxiolytic via Y1 and Y5 receptors FDA Status: Not approved as a therapeutic
Neuropeptide Y is a 36-amino acid endogenous peptide that is one of the most abundant neuropeptides in the brain and a well-established regulator of stress responses, anxiety, and resilience. While not developed as a drug, NPY biology provides critical insights into peptide-based approaches to anxiety and PTSD.
Mechanism of Action#
- Y1 receptor agonism: Anxiolytic effects mediated primarily through Y1 receptors in the amygdala, reducing fear and anxiety responses
- Y5 receptor effects: Contributes to anxiolytic and antidepressant-like effects
- HPA axis modulation: Reduces hypothalamic-pituitary-adrenal axis overactivity associated with chronic stress and anxiety disorders
- Stress buffering: Acts as an endogenous buffer against the effects of corticotropin-releasing factor (CRF), the primary stress-activating peptide
- Resilience marker: Higher NPY levels are associated with stress resilience in military populations
Research Findings#
- PTSD biomarker: Combat veterans with PTSD have significantly lower plasma NPY levels than combat-exposed veterans without PTSD
- Resilience correlation: Special forces soldiers showed higher NPY levels during extreme stress training compared to general military personnel
- Intranasal delivery: Intranasal NPY has been explored in preliminary studies for anxiety and PTSD, with some evidence of anxiolytic effects
- Amygdala regulation: NPY infusion into the amygdala produces potent anxiolytic effects in animal models, comparable to benzodiazepines
- Chronic stress: NPY expression is reduced by chronic stress, suggesting a depletion model for anxiety disorders
Important Considerations#
NPY has not been developed as a therapeutic drug due to challenges with delivery (poor BBB penetration, rapid degradation) and the complexity of its receptor system (Y1-Y5 receptors with opposing effects). The research primarily establishes NPY as a key endogenous anxiolytic system and a potential therapeutic target, rather than as a peptide drug itself. Development of small-molecule NPY receptor agonists is ongoing.
Other Peptides with Mood-Relevant Research#
Several additional peptides have indirect evidence for mood effects:
- Oxytocin: Intranasal oxytocin has been studied for social anxiety and PTSD. Results are mixed, with modest effects on social cognition and anxiety in some studies but inconsistent replication
- Cortistatin: Endogenous peptide with anxiolytic properties in animal models through somatostatin receptor activation. Very early-stage research
- DSIP: Delta sleep-inducing peptide has been anecdotally associated with anxiolytic effects, though evidence is very limited and the mechanism is poorly understood
- Pinealon: Short peptide with preclinical data suggesting neuroprotective and mood-stabilizing effects. No clinical evidence
Comparison Summary#
| Peptide | Primary Mood Effect | Evidence Level | Route | Status |
|---|---|---|---|---|
| Selank | Anxiolytic | Russian approval; limited Western data | Intranasal | Approved (Russia) |
| Semax | Antidepressant-relevant (BDNF) | Russian approval; limited Western data | Intranasal | Approved (Russia) |
| Rapastinel | Rapid antidepressant | Phase 3 (failed) | IV | Discontinued |
| Nemifitide | Rapid antidepressant | Phase 2 (mixed) | Subcutaneous | Stalled |
| NPY | Anxiolytic/stress resilience | Well-characterized biology | Research only | Not developed |
The Evidence Gap in Peptide Psychiatry#
A striking pattern in peptide approaches to depression and anxiety is the gap between promising mechanisms and clinical validation:
- Selank and semax have regulatory approval in Russia and decades of clinical use, but lack Western-standard phase 3 RCTs
- Rapastinel had the most advanced Western clinical program (FDA Breakthrough Therapy) but failed at the phase 3 stage
- Nemifitide showed intriguing rapid-onset signals but never achieved a definitive trial
- NPY has the best-characterized biology as an endogenous anxiolytic but has not been developed as a drug
This pattern reflects both the difficulty of antidepressant drug development (high placebo response rates, heterogeneous patient populations) and the specific challenges of peptide therapeutics (BBB penetration, stability, delivery).
Conclusion#
Peptide approaches to depression and anxiety target fundamentally different molecular systems than conventional monoamine-based antidepressants, offering the potential for rapid onset, novel mechanisms, and reduced side effects. The GABAergic modulation of selank, the BDNF upregulation of semax, the NMDA plasticity of rapastinel, and the endogenous stress-resilience of NPY each represent distinct therapeutic strategies that go beyond serotonin and norepinephrine.
However, the clinical evidence base remains limited by Western regulatory standards. The Russian approval of selank and semax provides real-world safety data but not the controlled trial evidence that FDA approval requires. The failure of rapastinel in phase 3 -- despite FDA Breakthrough Therapy designation -- illustrates the challenges that even well-characterized peptide mechanisms face in depression clinical trials.
For researchers and clinicians interested in this space, selank has the most practical evidence for anxiety (via Russian clinical experience), while the NMDA-modulation approach pioneered by rapastinel continues through next-generation oral compounds. The field remains active and the therapeutic need remains urgent.
For peptide comparisons relevant to this topic, see Nemifitide vs Rapastinel and Dihexa vs Semax.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Selank Overview and Research Guide
- Selank Dosing Protocols
- Selank Side Effects and Safety
- Semax Overview and Research Guide
- Semax Dosing Protocols
- Semax Side Effects and Safety
- Rapastinel Overview and Research Guide
- Rapastinel Dosing Protocols
- Rapastinel Side Effects and Safety
- Nemifitide Overview and Research Guide
- Nemifitide Dosing Protocols
- Nemifitide Side Effects and Safety
- Neuropeptide Y Overview and Research Guide
- Neuropeptide Y Dosing Protocols
- Neuropeptide Y Side Effects and Safety

{kind=link}
Frequently Asked Questions About Peptides for Depression and Anxiety: From Approved Treatments to Research Compounds
What does this article cover?
Peptides for depression and anxiety -- selank, semax, rapastinel, nemifitide, and neuropeptide Y reviewed with mechanisms, evidence levels, and the current landscape of peptide-based approaches to mental health. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Selank, Semax, Rapastinel, Nemifitide, Neuropeptide Y. Key context: Selank (Synthetic tuftsin analog approved in Russia as an anxiolytic, with GABA modulation and anti-anxie...); Semax (ACTH(4-10) analog approved in Russia for neuroprotection that modulates BDNF and monoaminergic ne...); Rapastinel (NMDA glycine-site modulator that showed rapid antidepressant effects in phase 2 but failed phase ...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Peptides for Depression and Anxiety: From Approved Treatments to Research Compounds." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: Synthetic tuftsin analog approved in Russia as an anxiolytic, with GABA modulation and anti-anxie.... ACTH(4-10) analog approved in Russia for neuroprotection that modulates BDNF and monoaminergic ne.... NMDA glycine-site modulator that showed rapid antidepressant effects in phase 2 but failed phase .... These takeaways are based on the research data available at the time of publication.
What is Selank and why is it significant?
Selank is a peptide discussed in this article because: Synthetic tuftsin analog approved in Russia as an anxiolytic, with GABA modulation and anti-anxiety effects comparable to benzodiazepines without sedation. For a complete profile of Selank, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Peptide Therapy for Brain Health: Neuroprotection, Cognition, and Recovery
Comprehensive guide to peptides for brain health covering neurotrophic factors, neuroprotective agents, anxiolytics, and experimental cognitive enhancers. Includes cerebrolysin, semax, selank, BPC-157, dihexa, pinealon, SS-31, and rapastinel.

FDA Peptide Categories Explained: Category 1 vs Category 2 (2026)
Understand the FDA peptide classification system. Learn the difference between Category 1, Category 2, and Category 3 peptides and what the 2024-2026 regulatory changes mean for researchers.
Peptide Stacking Guide 2026: Best Combinations by Goal
The definitive 2026 guide to peptide stacking organized by goal. Fat loss, muscle growth, healing, anti-aging, and cognitive stacks with evidence levels, dosing timing, and safety considerations.
You Might Also Like
Related content you may find interesting