Nemifitide vs Rapastinel: Peptide Antidepressants with Rapid Onset
Comparison of nemifitide and rapastinel, two peptide-based antidepressants that showed rapid onset of action in clinical trials but ultimately failed to achieve regulatory approval.
Verdict at a Glance
Both nemifitide and rapastinel represent promising but ultimately unsuccessful attempts to develop rapid-acting peptide antidepressants. Rapastinel had the stronger mechanistic rationale (NMDA modulation, convergent with ketamine's mechanism) and received FDA Breakthrough Therapy designation, but definitively failed in three phase 3 trials. Nemifitide showed intriguing rapid-onset effects in earlier-stage studies but never completed a definitive phase 3 program. Both demonstrated excellent tolerability without the side effects that limit ketamine use. Their clinical failures highlight the challenges of translating rapid-acting antidepressant mechanisms into reliable phase 3 efficacy.
| Best for | Pick | Why |
|---|---|---|
| Understanding NMDA-Based Antidepressant Mechanisms | Rapastinel | Rapastinel provided critical data about NMDA receptor modulation as an antidepressant strategy. Its clean separation of ketamine-like efficacy from ketamine-like side effects advanced the field, even though phase 3 trials failed. It spurred development of next-generation compounds. |
| Rapid Onset with Minimal Side Effects | Nemifitide | Nemifitide showed onset of antidepressant action within 48 hours with essentially no reported side effects in over 430 patients. While efficacy data is less definitive, the tolerability profile was remarkable for any antidepressant. |
| Treatment-Resistant Depression Research | Rapastinel | Rapastinel was specifically developed and granted FDA Breakthrough Therapy designation for treatment-resistant depression. Its mechanism (NMDA modulation) directly addresses the glutamatergic hypothesis of treatment-resistant depression. |
| Simple Self-Administration | Nemifitide | Nemifitide's subcutaneous injection route is simpler than rapastinel's IV infusion requirement. Despite a 15-30 minute half-life, nemifitide produced sustained effects from infrequent subcutaneous dosing, which would have been practical for outpatient use. |
| Historical Antidepressant Research Context | Rapastinel | Rapastinel's clinical program, from breakthrough therapy designation to phase 3 failure, is one of the most instructive case studies in modern antidepressant drug development and the challenges of the placebo response in depression trials. |
| Category | Nemifitide | Rapastinel | Advantage |
|---|---|---|---|
| Mechanism of Action | Synthetic pentapeptide (INN-00835) structurally related to MIF-1 (melanocyte-inhibiting factor). Binds multiple receptors including 5-HT2A (antagonist), NPY1, bombesin, and MC4/MC5 at micromolar concentrations. Crosses the blood-brain barrier. Exact antidepressant mechanism not fully elucidated. | Amidated tetrapeptide (GLYX-13) that acts as a partial agonist at the glycine site of the NMDA receptor. Enhances NMDA receptor-mediated synaptic plasticity without the dissociative, psychotomimetic, or addictive properties of full NMDA modulators like ketamine. Promotes BDNF release and mTOR signaling. | Rapastinel |
| Research Evidence | Completed 12 clinical studies in over 430 patients. Reached phase 3 trials. Showed rapid onset (48 hours to 5-7 days) in open-label and small controlled studies. A phase 2 RCT comparing 30 mg/d and 45 mg/d to placebo showed mixed results. Demonstrated efficacy in treatment-refractory patients in one open-label study. Never approved. | Received FDA Fast Track (2014) and Breakthrough Therapy (2016) designations. Phase 2 trials showed significant antidepressant effects within 24 hours with sustained effects for 7+ days. Three pivotal phase 3 trials (Allergan, 2019) all failed to differentiate from placebo on primary endpoints. Development discontinued. | Comparable |
| Side Effect Profile | Generally well tolerated in clinical trials. Few to no side effects reported in published studies. Very short half-life (15-30 minutes) limits systemic exposure. No serious adverse events consistently reported despite administration to over 430 patients. | Well tolerated without ketamine-like side effects. No dissociative or psychotomimetic symptoms. No cognitive impairment, abuse potential, or dependence. Most common side effects were mild and transient. Significant safety advantage over ketamine-based approaches. | Comparable |
| Administration | Subcutaneous injection only (inactive orally). Despite a very short half-life of 15-30 minutes, sustained antidepressant effects were observed for weeks from infrequent dosing. No implanted device required. Simple subcutaneous delivery. | Intravenous infusion required. Single IV doses produced antidepressant effects lasting 7+ days. No oral formulation available. IV route limits self-administration and requires clinical setting. Next-generation oral compounds (zelquistinel) were being developed. | Nemifitide |

Introduction#
Nemifitide and rapastinel represent two attempts to develop peptide-based antidepressants with rapid onset of action -- a goal that has become increasingly important given that conventional antidepressants (SSRIs, SNRIs) typically require 4-6 weeks for therapeutic effect. Both peptides showed promising rapid antidepressant effects in early clinical studies, and both ultimately failed to achieve regulatory approval, albeit for different reasons and at different stages.
Rapastinel (GLYX-13) was developed by Allergan and received FDA Breakthrough Therapy designation for treatment-resistant depression based on its NMDA receptor-modulating mechanism -- convergent with ketamine but without dissociative side effects. It failed all three pivotal phase 3 trials in 2019. Nemifitide (INN-00835) was developed by Innapharma/Tetragenex and showed rapid onset in multiple early-phase studies, but its clinical development program never reached a definitive phase 3 conclusion.
Their parallel stories illuminate both the promise and the challenges of developing novel rapid-acting antidepressants.
Mechanism of Action Comparison#
Nemifitide#
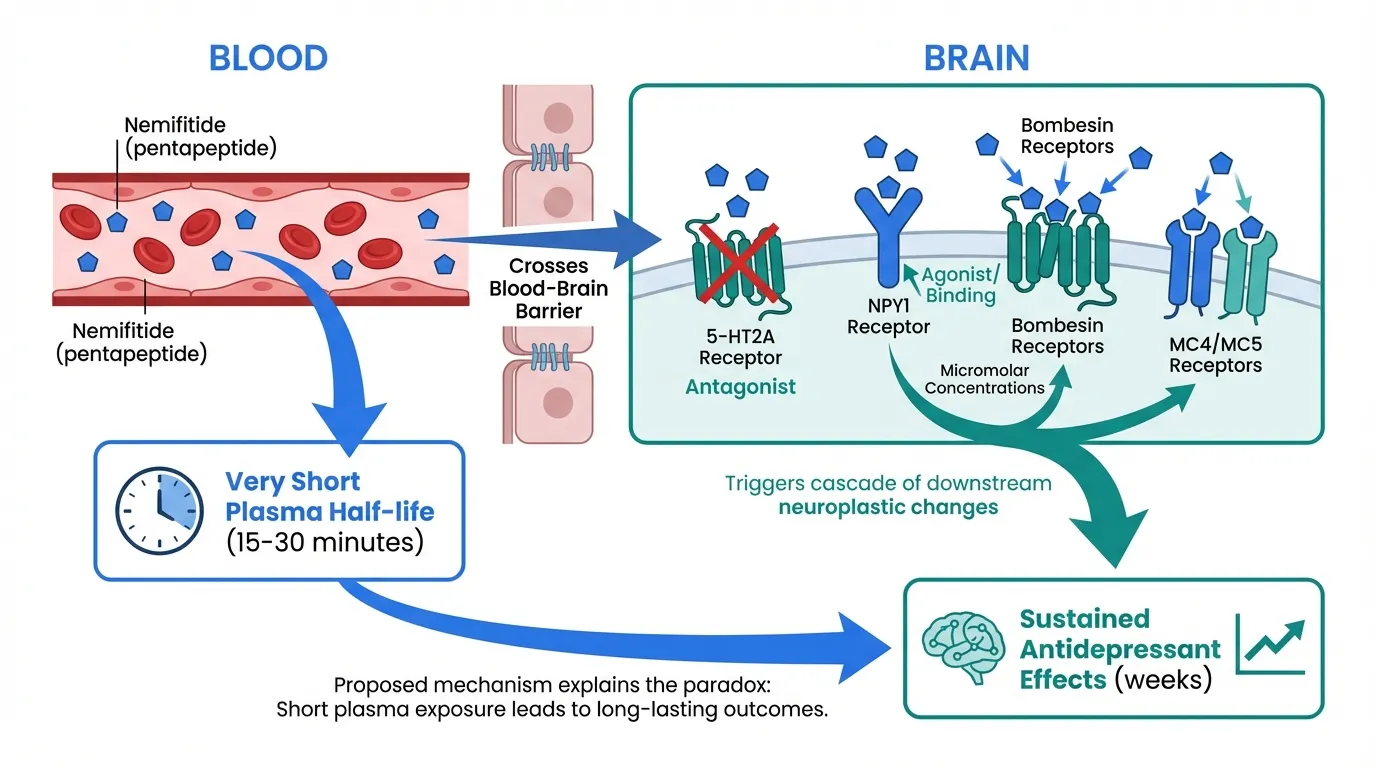
Nemifitide (INN-00835) is a synthetic pentapeptide with the sequence 4-F-Phe-4-OH-Pro-Arg-Gly-Trp-NH2, structurally related to melanocyte-inhibiting factor (MIF-1). Its mechanism of action is not fully elucidated:
- Multi-receptor binding: Binds to 5-HT2A (serotonin receptor, as an antagonist), NPY1 (neuropeptide Y receptor), bombesin receptors, and MC4/MC5 (melanocortin receptors) at micromolar concentrations
- Blood-brain barrier penetration: Crosses the BBB despite being a peptide, enabling central effects
- Very short half-life: Plasma half-life of only 15-30 minutes, yet antidepressant effects persist for weeks
- Structural relationship: Related to MIF-1 and other small peptides with documented CNS activity, but the precise mechanism linking its multi-receptor binding to antidepressant effects remains unclear
The disconnect between nemifitide's very short half-life and its sustained clinical effects suggests it may trigger a cascade of downstream neuroplastic changes rather than requiring continuous receptor occupancy.
Rapastinel#
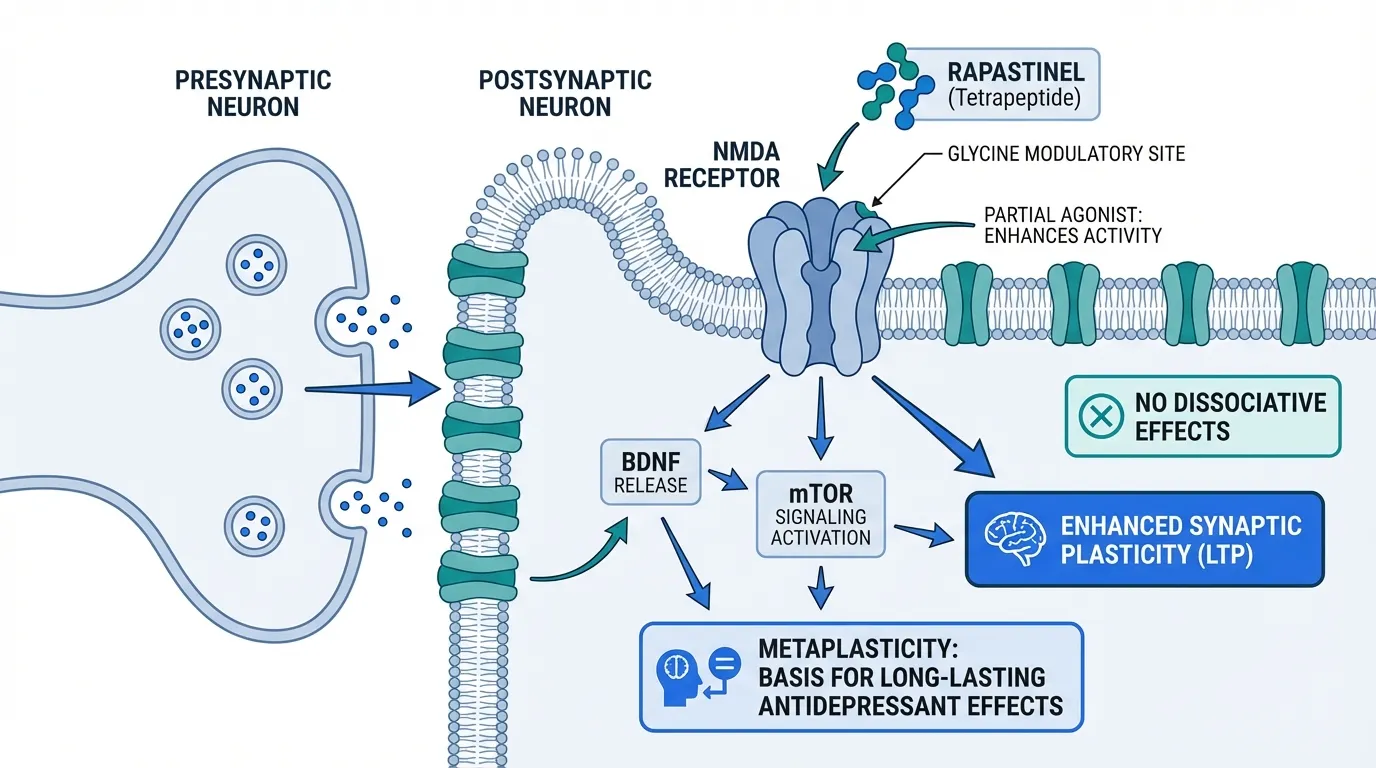
Rapastinel (GLYX-13, threonyl-prolyl-prolyl-threonyl-NH2) is an amidated tetrapeptide that modulates the NMDA receptor:
- Glycine site partial agonist: Enhances NMDA receptor activity at the glycine modulatory site without the excessive activation or blockade associated with ketamine
- Synaptic plasticity: Enhances the magnitude of long-term potentiation (LTP) at excitatory synapses in the medial prefrontal cortex and hippocampus
- BDNF/mTOR signaling: Promotes BDNF release and activates mTOR signaling, mechanisms shared with ketamine's rapid antidepressant effects
- Metaplasticity: Produces long-lasting antidepressant effects through metaplasticity -- changes in the capacity for future synaptic plasticity -- rather than simple acute receptor modulation
- No dissociative effects: Unlike ketamine (an NMDA antagonist), rapastinel does not produce dissociation, psychotomimetic effects, or cognitive impairment
Mechanistic Comparison#
| Feature | Nemifitide | Rapastinel |
|---|---|---|
| Structure | Pentapeptide (5 AA) | Tetrapeptide (4 AA) |
| Primary target | Multi-receptor (5-HT2A, NPY1, MC4/5) | NMDA glycine site (partial agonist) |
| Mechanism clarity | Poorly understood | Well characterized |
| Relationship to ketamine | None | Convergent downstream pathway |
| Onset of action | 48 hours to 5-7 days | Within 24 hours |
| Duration of effect | Weeks from single/few doses | 7+ days from single IV dose |
| BBB penetration | Yes | Yes |
| Half-life | 15-30 minutes | Not well characterized (IV bolus) |
Dosing Comparison#
Nemifitide Dosing#
Based on clinical trial protocols:
- Route: Subcutaneous injection (inactive orally)
- Phase 2 doses: 30 mg/day and 45 mg/day studied in RCT
- Frequency: Daily injection during treatment periods, though sustained effects from infrequent dosing observed
- Onset: 48 hours to peak effect at approximately 1 week
- Duration of effect: Efficacy sustained during 4-week follow-up periods after treatment cessation
Rapastinel Dosing#
Based on clinical trial protocols:
- Route: Intravenous infusion
- Phase 2 dose: Single IV dose of 1, 5, 10, or 30 mg/kg studied
- Efficacious dose: 5 and 10 mg/kg showed significant antidepressant effects in phase 2
- Frequency: Single dose or weekly IV infusions
- Onset: Within 24 hours of single IV administration
- Duration of effect: Antidepressant effects sustained for 7+ days after single dose
Side Effects Comparison#
Nemifitide Side Effects#
Remarkably well tolerated across clinical studies:
- No consistent side effects: Published studies report "few to no side effects" in over 430 patients across 12 clinical trials
- No serious adverse events: No serious adverse events consistently attributed to nemifitide
- Short systemic exposure: The 15-30 minute half-life means minimal sustained systemic exposure
- No withdrawal effects: No evidence of dependence or withdrawal
- No sexual dysfunction: Unlike SSRIs, no sexual side effects reported
Rapastinel Side Effects#
Also well tolerated, with a clean separation from ketamine's side effects:
- No dissociation: Unlike ketamine, rapastinel did not produce dissociative symptoms
- No psychotomimetic effects: No hallucinations, perceptual disturbances, or psychosis
- No cognitive impairment: No acute cognitive impairment or memory disruption
- No abuse potential: No evidence of reinforcing effects or addiction liability
- Common adverse events: Mild and transient -- headache, dizziness, and somnolence most reported
- No respiratory depression: Unlike ketamine, no respiratory concerns
Research Evidence Comparison#
Nemifitide Research#
- Phase 1/PK studies: Established pharmacokinetic profile and demonstrated BBB penetration and subcutaneous bioavailability
- Open-label studies: Showed rapid onset (48 hours) with peak effect at approximately 1 week. Efficacy sustained for 4+ weeks after treatment cessation
- Phase 2 RCT: 30 mg/d and 45 mg/d compared to placebo in major depressive disorder. Results described as mixed, with some evidence of efficacy but not uniformly positive
- Treatment-refractory study: Open-label study in severely depressed, treatment-refractory patients showed meaningful response
- Re-treatment: Follow-up re-treatment study showed comparable or improved response compared to initial treatment
- Overall: 12 clinical studies, 430+ patients. Never completed a definitive phase 3 program
Evidence level: Low -- multiple phase 1/2 studies with intriguing results, but no definitive phase 3 RCT. Mixed controlled trial results.
Rapastinel Research#
- Phase 2 (Preskorn et al., 2015): Single IV dose of rapastinel (1, 5, 10, or 30 mg/kg) as adjunctive therapy showed significant antidepressant effects at 5 and 10 mg/kg within 24 hours, sustained for 7+ days
- FDA designations: Fast Track (2014) and Breakthrough Therapy (2016) designations based on phase 2 data
- Phase 3 failure (2019): All three pivotal phase 3 trials failed to differentiate rapastinel from placebo on primary and key secondary endpoints
- OCD proof of concept: Small study showed potential benefit in obsessive-compulsive disorder
- PTSD potential: Preclinical data suggested efficacy in PTSD models
- Legacy: Spurred development of next-generation NMDA modulators including apimostinel (NRX-1074) and zelquistinel (AGN-241751), an oral compound
Evidence level: Low -- promising phase 2 data but definitive phase 3 failure. Development discontinued by Allergan.
Key Differences Summary#
- Mechanism: Nemifitide has a poorly understood multi-receptor mechanism. Rapastinel has a well-characterized NMDA glycine site mechanism.
- Clinical stage: Nemifitide completed multiple phase 1/2 studies but never had a definitive phase 3. Rapastinel reached and failed phase 3.
- Administration: Nemifitide uses subcutaneous injection. Rapastinel requires IV infusion.
- FDA recognition: Rapastinel received Fast Track and Breakthrough Therapy designations. Nemifitide received no FDA designations.
- Onset: Both showed rapid onset (nemifitide 48 hours, rapastinel 24 hours), dramatically faster than conventional antidepressants.
- Tolerability: Both were remarkably well tolerated with no significant or dose-limiting adverse effects in clinical trials.
- Development status: Both are effectively discontinued. Rapastinel's mechanism inspired next-generation compounds.
Conclusion#
Nemifitide and rapastinel share a common narrative: rapid-acting peptide antidepressants with excellent tolerability that ultimately could not demonstrate reliable efficacy in definitive clinical trials. Both showed genuine promise in early-phase studies, suggesting that peptide-based approaches to depression can achieve rapid onset without the side effects that limit existing rapid-acting treatments (ketamine, esketamine).
Rapastinel's story is more instructive because its well-characterized mechanism and phase 3 program provide clearer lessons. The phase 3 failure was attributed primarily to unusually high placebo response rates -- a well-known challenge in depression clinical trials -- rather than to a fundamental flaw in the NMDA modulation approach. Its mechanism has been validated by the success of ketamine/esketamine and continues to be pursued through next-generation oral compounds.
Nemifitide's story is more enigmatic. Its multi-receptor binding, very short half-life with sustained effects, and limited but intriguing clinical data raise questions that were never fully answered by a definitive trial program. The mechanistic basis for its antidepressant activity remains unclear.
Both peptides contributed to the growing understanding that rapid-acting antidepressant mechanisms exist beyond monoamine modulation, and that peptide-based approaches can achieve central nervous system effects with favorable safety profiles. Their failures underscore the difficulty of translating early-phase antidepressant promise into phase 3 success.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Understanding NMDA-Based Antidepressant Mechanisms
Rapastinel
Rapastinel provided critical data about NMDA receptor modulation as an antidepressant strategy. Its clean separation of ketamine-like efficacy from ketamine-like side effects advanced the field, even though phase 3 trials failed. It spurred development of next-generation compounds.
Rapid Onset with Minimal Side Effects
Nemifitide
Nemifitide showed onset of antidepressant action within 48 hours with essentially no reported side effects in over 430 patients. While efficacy data is less definitive, the tolerability profile was remarkable for any antidepressant.
Treatment-Resistant Depression Research
Rapastinel
Rapastinel was specifically developed and granted FDA Breakthrough Therapy designation for treatment-resistant depression. Its mechanism (NMDA modulation) directly addresses the glutamatergic hypothesis of treatment-resistant depression.
Simple Self-Administration
Nemifitide
Nemifitide's subcutaneous injection route is simpler than rapastinel's IV infusion requirement. Despite a 15-30 minute half-life, nemifitide produced sustained effects from infrequent subcutaneous dosing, which would have been practical for outpatient use.
Historical Antidepressant Research Context
Rapastinel
Rapastinel's clinical program, from breakthrough therapy designation to phase 3 failure, is one of the most instructive case studies in modern antidepressant drug development and the challenges of the placebo response in depression trials.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Nemifitide vs Rapastinel: Peptide Antidepressants with Rapid Onset
Which is better, Nemifitide or Rapastinel?
Both nemifitide and rapastinel represent promising but ultimately unsuccessful attempts to develop rapid-acting peptide antidepressants. Rapastinel had the stronger mechanistic rationale (NMDA modulation, convergent with ketamine's mechanism) and received FDA Breakthrough Therapy designation, but definitively failed in three phase 3 trials. Nemifitide showed intriguing rapid-onset effects in earlier-stage studies but never completed a definitive phase 3 program. Both demonstrated excellent to... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Nemifitide and Rapastinel?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Rapastinel; Research Evidence: advantage goes to neither (tie); Side Effect Profile: advantage goes to neither (tie). 1 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Rapastinel over Nemifitide?
For the scenario of "Understanding NMDA-Based Antidepressant Mechanisms," research data suggests Rapastinel may be more relevant. Rapastinel provided critical data about NMDA receptor modulation as an antidepressant strategy. Its clean separation of ketamine-like efficacy from ketamine-like side effects advanced the field, ev.... This is based on currently available evidence and individual circumstances may differ.
How do Nemifitide and Rapastinel differ in their mechanisms of action?
Nemifitide: Synthetic pentapeptide (INN-00835) structurally related to MIF-1 (melanocyte-inhibiting factor). Binds multiple receptors including 5-HT2A (antagonist), NPY1, bombesin, and MC4/MC5 at micromolar co.... Rapastinel: Amidated tetrapeptide (GLYX-13) that acts as a partial agonist at the glycine site of the NMDA receptor. Enhances NMDA receptor-mediated synaptic plasticity without the dissociative, psychotomimeti....
Which has fewer side effects, Nemifitide or Rapastinel?
In terms of side effects and tolerability, the advantage goes to neither (comparable). Nemifitide: Generally well tolerated in clinical trials. Few to no side effects reported in published studies. Very short half-life (15-30 minutes) limits syst.... Rapastinel: Well tolerated without ketamine-like side effects. No dissociative or psychotomimetic symptoms. No cognitive impairment, abuse potential, or depend....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.