Oral vs Injectable GLP-1 Drugs: The Complete Comparison

Introduction#
The GLP-1 receptor agonist field is undergoing a fundamental shift in drug delivery. For years, these therapies were available only as injectable formulations, requiring weekly or daily subcutaneous injections. Now, a wave of oral formulations is emerging that could make GLP-1 therapy as simple as taking a daily pill.
This comparison examines every oral GLP-1 drug in clinical development against the injectable standard of care, analyzing efficacy, tolerability, convenience, and practical considerations.
Important: Only injectable semaglutide (Wegovy), injectable tirzepatide (Zepbound), and oral semaglutide 25 mg (oral Wegovy) are FDA-approved for weight management. All other agents discussed are investigational.
The Oral vs Injectable Landscape#
Currently Available#
| Drug | Route | Dosing | FDA Approved |
|---|---|---|---|
| Semaglutide (Wegovy) | SC injection | Weekly | Yes (2021) |
| Tirzepatide (Zepbound) | SC injection | Weekly | Yes (2023) |
| Oral semaglutide (Wegovy) | Oral tablet | Daily 25 mg | Yes (2025) |
In Development#
| Drug | Route | Dosing | Phase |
|---|---|---|---|
| Orforglipron | Oral tablet | Daily | Phase 3 |
| Aleniglipron | Oral tablet | Daily | Phase 2 |
| Oral VK2735 | Oral tablet | Daily | Phase 2 |
| Oral amycretin | Oral tablet (SNAC) | Daily | Phase 1 |
| Oral ribupatide | Oral tablet | Daily | Phase 2 |
Head-to-Head Efficacy Comparison#
Oral vs Injectable Weight Loss Data#
| Drug | Route | Weight Loss | Duration | Trial |
|---|---|---|---|---|
| Tirzepatide 15 mg | SC weekly | 20.9% | 72 wk | SURMOUNT-1 |
| Semaglutide 2.4 mg | SC weekly | 14.9% | 68 wk | STEP 1 |
| Oral semaglutide 50 mg | Oral daily | 15.1% | 68 wk | OASIS 1 |
| Oral semaglutide 25 mg | Oral daily | 13.6% | 64 wk | OASIS 4 |
| Aleniglipron 240 mg | Oral daily | 15.3%* | 36 wk | ACCESS II |
| Oral VK2735 | Oral daily | 12.2% | 13 wk | VENTURE-Oral |
| Oral amycretin | Oral daily | 13.1% | 12 wk | Phase 1 |
| Oral ribupatide 50 mg | Oral daily | ~12% | 26 wk | Phase 2 |
| Orforglipron 36 mg | Oral daily | 11.2% | 72 wk | ATTAIN-1 |
*Placebo-adjusted value
The data reveal an important pattern: oral formulations are approaching but have not yet matched the best injectable results at comparable timepoints. However, shorter trial durations for newer oral agents (13-36 weeks) make direct comparisons difficult, as weight loss typically continues beyond these timepoints.
Semaglutide: The Direct Comparison#
Semaglutide is the only GLP-1 drug available in both oral and injectable forms at weight-management doses, enabling direct comparison:
| Parameter | SC Semaglutide 2.4 mg | Oral Semaglutide 50 mg | Oral Semaglutide 25 mg |
|---|---|---|---|
| Weight loss | 14.9% (68 wk) | 15.1% (68 wk) | 13.6% (64 wk) |
| Dosing | Weekly injection | Daily tablet (fasting) | Daily tablet (fasting) |
| Food restriction | None | 30-min fasting | 30-min fasting |
| Formulation | Acylated peptide | SNAC-enhanced peptide | SNAC-enhanced peptide |
| FDA obesity approval | Yes (2021) | No (not approved dose) | Yes (2025) |
The OASIS 1 trial showed that high-dose oral semaglutide (50 mg daily) achieves weight loss comparable to injectable semaglutide (2.4 mg weekly). The approved oral dose (25 mg) provides slightly less weight loss (~13.6%) but eliminates the need for injection.
Oral Small Molecules vs Oral Peptides#
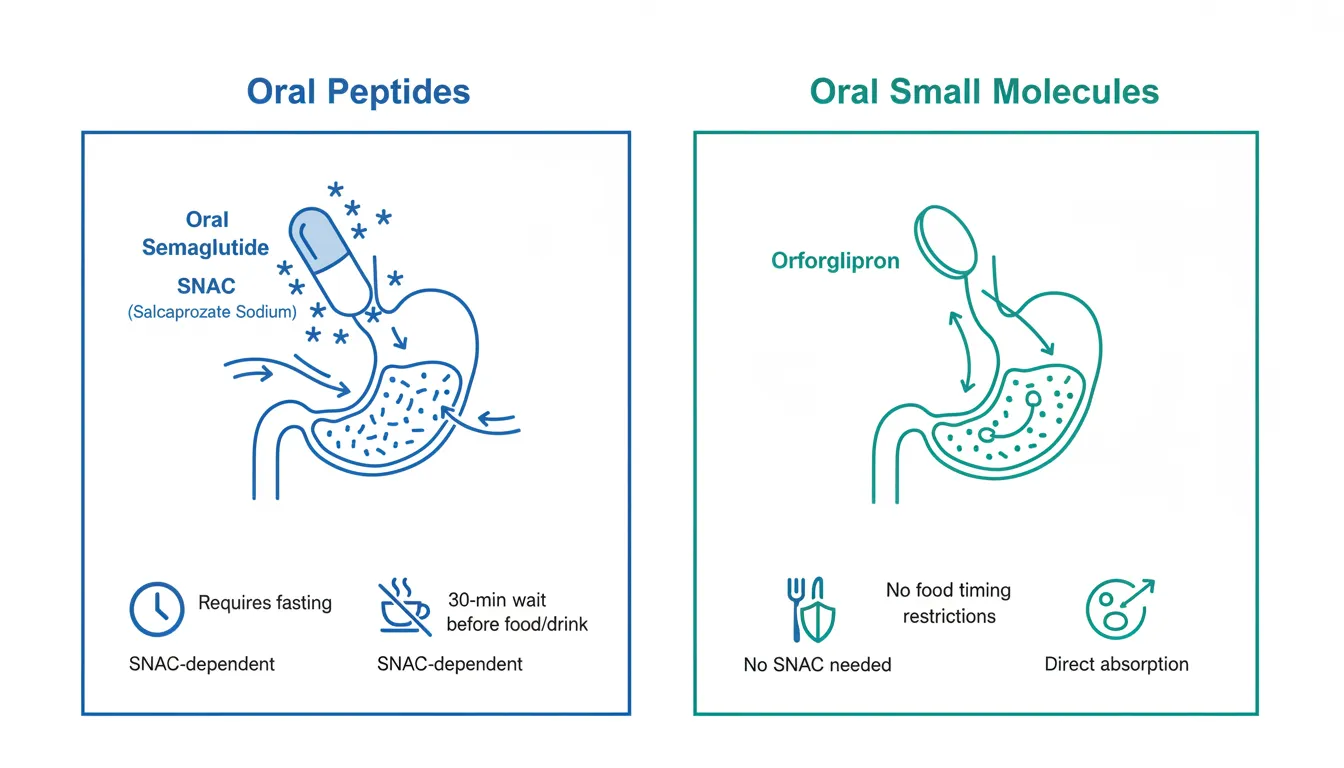
A critical distinction exists between oral peptides (which require absorption enhancers like SNAC) and oral small molecules (which do not):
Oral Peptides (SNAC-dependent)#
- Oral semaglutide: Requires SNAC, 30-minute fasting window, taken on empty stomach
- Oral amycretin: Uses SNAC, similar fasting requirements expected
Oral Small Molecules (No SNAC)#
- Orforglipron: No food timing restrictions, no SNAC needed
- Aleniglipron: No food timing restrictions, no SNAC needed
Oral Dual Agonist Peptides#
- Oral VK2735: Absorption mechanism not fully disclosed
- Oral ribupatide: Absorption mechanism not fully disclosed
The practical difference is significant. SNAC-dependent oral peptides require patients to take the drug first thing in the morning on an empty stomach and wait 30 minutes before eating or drinking. Small molecules like orforglipron and aleniglipron can be taken at any time, with or without food.
Advantages of Oral GLP-1 Drugs#
Patient Preference and Adherence#
Surveys consistently show that most patients prefer oral medications over injections. Needle phobia, injection technique anxiety, and the social visibility of injections are all barriers that oral formulations eliminate.
Simplified Logistics#
| Factor | Injectable | Oral |
|---|---|---|
| Cold chain | Required (2-8 C) | Not required |
| Needle disposal | Sharp container needed | Not needed |
| Training | Injection technique | None |
| Travel | Cooler bag, needles | Pill bottle |
| Storage | Refrigerator | Room temperature |
| Supply chain | Specialty pharmacy | Standard pharmacy |
Cost and Access Potential#
Oral small molecules (orforglipron, aleniglipron) have simpler manufacturing processes than injectable peptides. This could translate to lower production costs and potentially more accessible pricing. Oral semaglutide 25 mg launched at $149/month in the US, significantly below the $1,350/month list price for injectable Wegovy.
Advantages of Injectable GLP-1 Drugs#
Higher Peak Efficacy#
Injectable formulations currently deliver higher peak weight loss:
- Best injectable: Tirzepatide at 20.9% (72 wk), retatrutide at 28.7% (68 wk)
- Best oral: Oral semaglutide 50 mg at 15.1% (68 wk), aleniglipron at 15.3% (36 wk, placebo-adjusted)
For patients seeking maximum weight loss, injectables remain the more potent option as of early 2026.
Established Multi-Receptor Options#
All approved and late-stage dual and triple agonists are injectable: tirzepatide (GIP/GLP-1), retatrutide (GIP/GLP-1/glucagon), CagriSema (amylin/GLP-1), and survodutide (GLP-1/glucagon). Oral dual agonists (VK2735, ribupatide) are in earlier development stages.
No Food Timing Restrictions#
Weekly injectable semaglutide and tirzepatide have no food or fasting requirements. Ironically, some oral formulations (SNAC-dependent) have stricter food timing requirements than their injectable counterparts.
Less Frequent Dosing#
Weekly injections require dosing just 52 times per year, versus 365 times for daily oral pills. Monthly MariTide reduces this to 12 doses per year. Some patients may find weekly or monthly dosing more manageable than a daily pill.
Drug-by-Drug Oral Comparison#
Orforglipron (Eli Lilly) -- Phase 3#
The most advanced oral small molecule, orforglipron showed 11.2% weight loss at 72 weeks in ATTAIN-1. While this is lower than injectable semaglutide or tirzepatide, orforglipron offers:
- No food timing restrictions
- No SNAC absorption enhancer needed
- Stable at room temperature
- Simple once-daily dosing
- Non-peptide structure (easier manufacturing)
The ATTAIN program includes studies in T2D (ATTAIN-2), cardiovascular outcomes, and combinations.
Aleniglipron (Structure Therapeutics) -- Phase 2#
Aleniglipron has produced the most competitive oral weight loss data to date:
- ACCESS: 11.3% placebo-adjusted weight loss at 36 weeks (120 mg)
- ACCESS II: 15.3% placebo-adjusted weight loss at 36 weeks (240 mg)
- Low-dose initiation (2.5 mg) significantly improved tolerability
- Phase 3 planned for mid-2026
At 36 weeks, aleniglipron's trajectory suggests it could approach injectable-level efficacy with longer treatment duration.
Oral VK2735 (Viking Therapeutics) -- Phase 2#
VK2735 is unique as the only dual GLP-1/GIP agonist with an oral formulation in clinical development:
- 12.2% weight loss at 13 weeks (oral tablet)
- 97% of treatment groups achieved at least 5% weight loss
- Oral Phase 3 expected Q3 2026
- The injectable SC formulation achieved 14.7% at 13 weeks
Oral Amycretin (Novo Nordisk) -- Phase 1#
Novo Nordisk's oral amycretin demonstrated 13.1% weight loss at just 12 weeks, the highest early-stage oral result. However, this was a Phase 1 trial with small numbers. The injectable SC formulation achieved 24.3% at 36 weeks, suggesting significant upside potential.
Oral Ribupatide (Kailera/Hengrui) -- Phase 2#
An oral dual GLP-1/GIP agonist that achieved approximately 12% weight loss at 26 weeks in Phase 2 in China, with more than half of participants on the highest dose losing at least 10%. GI side effects were mild to moderate.
Tolerability Comparison#
GI side effects are the primary tolerability concern for all GLP-1 drugs, regardless of route:
| Drug | Route | Nausea | Vomiting | Discontinuation |
|---|---|---|---|---|
| SC semaglutide 2.4 mg | Injectable | 20-40% | 10-21% | ~7% |
| Tirzepatide 15 mg | Injectable | 20-30% | 10-15% | ~5% |
| Orforglipron 36 mg | Oral | ~30% | ~15% | ~8% |
| Aleniglipron 120 mg | Oral | ~65% | ~32% | ~11% |
| Oral VK2735 | Oral | ~20% | ~26% | Low |
| Oral amycretin | Oral | ~82% | ~53% | ~33% |
Oral formulations do not appear to have inherently better or worse GI tolerability than injectables. Dose titration strategies are critical for both routes.
The Future of Oral GLP-1 Drugs#
The Convergence#
The efficacy gap between oral and injectable GLP-1 drugs is narrowing. Aleniglipron at higher doses (240 mg) is approaching 15% weight loss at 36 weeks. Oral amycretin achieved 13.1% at just 12 weeks. As dose optimization continues and trial durations extend, oral agents may close the gap further.
Combination Potential#
The future likely includes oral combination therapies. If oral GLP-1/GIP dual agonists (VK2735, ribupatide) achieve efficacy similar to injectable tirzepatide, the convenience advantage could be transformative.
Who Should Consider Oral vs Injectable?#
Oral may be preferred for:
- Patients with needle phobia or injection anxiety
- Patients who travel frequently
- Those seeking lower-cost options
- Patients comfortable with daily dosing
- First-line therapy before escalating to injectables
Injectable may be preferred for:
- Patients seeking maximum weight loss
- Those who prefer less frequent dosing (weekly or monthly)
- Patients who struggle with daily medication adherence
- Those who need dual or triple agonist mechanisms
Conclusion#
The oral GLP-1 revolution is well underway. With oral semaglutide approved, orforglipron in Phase 3, and multiple oral dual agonists in Phase 2, the next few years will see a dramatic expansion of oral obesity pharmacotherapy options.
While injectable formulations currently offer the highest peak weight loss, oral agents are approaching competitive efficacy with significant practical advantages. The ideal anti-obesity toolkit of the future will likely include both oral and injectable options, allowing personalized treatment selection based on individual patient preferences, efficacy goals, and clinical needs.
This article is for educational and informational purposes only. It does not constitute medical advice. Consult a healthcare provider for treatment decisions.
References#
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety
- Orforglipron Overview and Research Guide
- Orforglipron Dosing Protocols
- Orforglipron Side Effects and Safety
- Tirzepatide Overview and Research Guide
- Tirzepatide Dosing Protocols
- Tirzepatide Side Effects and Safety
- Aleniglipron Overview and Research Guide
- Aleniglipron Dosing Protocols
- Aleniglipron Side Effects and Safety
- VK2735 Overview and Research Guide
- VK2735 Dosing Protocols
- VK2735 Side Effects and Safety
- Amycretin Overview and Research Guide
- Amycretin Dosing Protocols
- Amycretin Side Effects and Safety
- Ribupatide Overview and Research Guide
- Ribupatide Dosing Protocols
- Ribupatide Side Effects and Safety

{kind=link}
Frequently Asked Questions About Oral vs Injectable GLP-1 Drugs: The Complete Comparison
What does this article cover?
A head-to-head comparison of oral and injectable GLP-1 drugs for obesity, including oral semaglutide, orforglipron, aleniglipron, and VK2735 versus their injectable counterparts. This article is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Semaglutide, Orforglipron, Tirzepatide, Aleniglipron, VK2735, Amycretin, Ribupatide. Key context: Semaglutide (Available in both oral (Rybelsus/oral Wegovy) and injectable (Wegovy/Ozempic) forms, enabling dir...); Orforglipron (Leading oral small molecule GLP-1 agonist in Phase 3 with no food timing restrictions); Tirzepatide (Injectable-only dual agonist representing the current gold standard for weight loss). Each peptide is discussed based on available research evidence.
How does Semaglutide compare to Orforglipron?
This article provides a detailed comparison of Semaglutide and Orforglipron based on available research data. Semaglutide: Available in both oral (Rybelsus/oral Wegovy) and injectable (Wegovy/Ozempic) forms, enabling direct comparison. Orforglipron: Leading oral small molecule GLP-1 agonist in Phase 3 with no food timing restrictions. See the full article for detailed analysis.
What are the key takeaways from this article?
The main findings covered in this article include: Available in both oral (Rybelsus/oral Wegovy) and injectable (Wegovy/Ozempic) forms, enabling dir.... Leading oral small molecule GLP-1 agonist in Phase 3 with no food timing restrictions. Injectable-only dual agonist representing the current gold standard for weight loss. These takeaways are based on the research data available at the time of publication.
What is Semaglutide and why is it significant?
Semaglutide is a peptide discussed in this article because: Available in both oral (Rybelsus/oral Wegovy) and injectable (Wegovy/Ozempic) forms, enabling direct comparison. For a complete profile of Semaglutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

GLP-1 Drugs Ranked by Weight Loss: 2026 Data Comparison
Every GLP-1 and incretin drug ranked by clinical weight loss data as of 2026, from retatrutide at 28.7% to oral orforglipron at 11.2%, with comparison tables and trial details.

The GLP-1 Pill Race: Every Oral Obesity Drug in Development
A comprehensive guide to every oral GLP-1 obesity drug in development, from approved oral semaglutide to pipeline agents orforglipron, aleniglipron, VK2735, ribupatide, and amycretin.

Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained
A comprehensive guide to every GLP-1 receptor agonist drug, from FDA-approved semaglutide and tirzepatide to pipeline therapies like retatrutide, amycretin, MariTide, and oral orforglipron.
You Might Also Like
Related content you may find interesting