The GLP-1 Pill Race: Every Oral Obesity Drug in Development

Introduction#
The race to develop a GLP-1 obesity pill is one of the most consequential competitions in pharmaceutical history. Injectable GLP-1 drugs like semaglutide and tirzepatide have already transformed weight management, but injections limit adoption due to needle anxiety, cold chain requirements, and higher costs. An effective oral alternative could expand the addressable market from tens of millions to hundreds of millions of patients worldwide.
As of early 2026, one oral GLP-1 drug is approved for obesity (oral semaglutide 25 mg), and at least five more are racing through clinical development. This guide covers every oral obesity drug in the pipeline, their clinical data, and the technologies enabling oral delivery of these molecules.
Important: Only oral semaglutide 25 mg (oral Wegovy) is currently FDA-approved for weight management. All other oral agents discussed are investigational.
The State of the Race#
| Drug | Company | Type | Phase | Weight Loss | Duration |
|---|---|---|---|---|---|
| Oral semaglutide 25 mg | Novo Nordisk | Peptide + SNAC | Approved | 13.6% | 64 wk |
| Orforglipron | Eli Lilly | Small molecule | Phase 3 | 11.2% | 72 wk |
| Aleniglipron | Structure Therapeutics | Small molecule | Phase 2 | 15.3%* | 36 wk |
| Oral VK2735 | Viking Therapeutics | Peptide | Phase 2 | 12.2% | 13 wk |
| Oral amycretin | Novo Nordisk | Peptide + SNAC | Phase 1 | 13.1% | 12 wk |
| Oral ribupatide | Kailera/Hengrui | Peptide | Phase 2 | ~12% | 26 wk |
*Placebo-adjusted value
The Two Technologies#
Oral Peptides (SNAC-Enhanced)#
The first approach to oral GLP-1 delivery was pioneered by Novo Nordisk with semaglutide. These drugs use SNAC (sodium N-[8-(2-hydroxybenzoyl)amino]caprylate), a small molecule that creates a localized buffer zone in the stomach wall, enabling peptide absorption.
How SNAC works:
- Tablet dissolves in the stomach
- SNAC raises local pH near the gastric mucosa
- This protects the peptide from acid degradation
- SNAC also enhances transcellular absorption
- Peptide enters the bloodstream through the gastric wall
Limitations of SNAC:
- Must be taken on an empty stomach (overnight fasting)
- 30-minute wait before eating, drinking, or other medications
- Low oral bioavailability (~1% for semaglutide)
- Large tablet needed to deliver sufficient drug
- Food dramatically reduces absorption
Current SNAC-dependent oral drugs:
- Oral semaglutide (approved)
- Oral amycretin (Phase 1)
Oral Small Molecules (Non-Peptide)#
The second approach replaces the peptide entirely with a non-peptide small molecule that activates the GLP-1 receptor. Small molecules are naturally absorbed from the GI tract like conventional oral drugs.
Advantages of small molecules:
- No food timing restrictions
- No absorption enhancer needed
- Higher oral bioavailability
- Smaller tablets
- Room temperature stability
- Simpler, cheaper manufacturing
Current oral small molecules:
- Orforglipron (Phase 3)
- Aleniglipron (Phase 2)
Oral Peptide Dual Agonists#
A third category involves oral peptide dual agonists that may use proprietary absorption technologies:
- Oral VK2735 (absorption technology not fully disclosed)
- Oral ribupatide (absorption technology not fully disclosed)
Drug Profiles#
1. Oral Semaglutide 25 mg (Novo Nordisk) -- APPROVED#
Status: FDA-approved (December 2025), launched January 2026 at $149/month Mechanism: GLP-1 receptor agonist peptide with SNAC Dosing: Once daily on empty stomach, 30-minute fasting window
Oral semaglutide made history as the first oral GLP-1 drug approved for weight management:
- OASIS 4: 13.6% weight loss at 64 weeks (25 mg dose)
- OASIS 1: 15.1% weight loss at 68 weeks (50 mg dose, not approved for obesity)
- GI side effects consistent with the GLP-1 class
- Available in 3, 7, 14, and 25 mg tablets (dose escalation over 8 weeks)
The 25 mg dose provides weight loss comparable to (though slightly less than) injectable semaglutide 2.4 mg (14.9% at 68 weeks). The higher 50 mg dose matched injectable efficacy but is not approved for obesity.
Key limitation: The SNAC formulation requires strict fasting -- take on an empty stomach with no more than 4 oz of water, wait 30 minutes before food, drink, or other medications.
Competitive advantage: It is approved and available now, at a significantly lower price ($149/month) than injectable Wegovy (~$1,350/month list price).
2. Orforglipron (Eli Lilly) -- PHASE 3#
Status: Phase 3 (ATTAIN program, multiple ongoing trials) Mechanism: Non-peptide small molecule GLP-1 receptor agonist Dosing: Once daily, no food restrictions
Orforglipron is the most advanced non-peptide oral GLP-1 agonist:
- ATTAIN-1: 11.2% weight loss at 72 weeks (36 mg dose) in 3,127 participants
- ATTAIN-2: Phase 3 in T2D, results pending
- 54.6% achieved at least 10% weight loss at 36 mg
- GI side effects consistent with GLP-1 class
- CYP enzyme-independent metabolism (fewer drug interactions)
- Stable at room temperature
Structure: Orforglipron (MW 883 Da) is a fully non-peptide molecule based on a pyrimidine scaffold. It was derived from Lilly's proprietary small molecule GLP-1R agonist program. Unlike peptide-based oral GLP-1 drugs, it does not require SNAC or any absorption enhancer.
Competitive analysis: Orforglipron's 11.2% weight loss at 72 weeks is lower than oral semaglutide's 13.6% at 64 weeks and significantly lower than injectable tirzepatide's 20.9%. However, it offers no food timing restrictions, room temperature storage, and potentially lower manufacturing costs. The ATTAIN program also includes CV outcomes trials that could establish cardioprotective benefits.
3. Aleniglipron (Structure Therapeutics) -- PHASE 2#
Status: Phase 2 complete, Phase 3 planned mid-2026 Mechanism: Non-peptide small molecule GLP-1 receptor agonist Dosing: Once daily, no food restrictions
Aleniglipron has produced the most competitive Phase 2 oral weight loss data:
- ACCESS Phase 2b: Placebo-adjusted weight loss of 8.2% (45 mg), 9.8% (90 mg), and 11.3% (120 mg) at 36 weeks
- ACCESS II: Up to 15.3% placebo-adjusted weight loss at 36 weeks (240 mg)
- 86% achieved at least 5% weight loss at 120 mg
- 70% achieved at least 10% weight loss at 120 mg
- Weight loss continuing at 44 weeks in open-label extension
Tolerability innovation: Aleniglipron's tolerability improved significantly with low-dose initiation at 2.5 mg. In a body composition sub-study, starting at 2.5 mg eliminated adverse event-related discontinuations during the initial dosing period. This suggests that the 65% nausea rate seen in ACCESS may be manageable with careful titration.
Competitive analysis: At 36 weeks, aleniglipron's trajectory at higher doses (240 mg: 15.3% placebo-adjusted) suggests it could approach or exceed injectable semaglutide levels at longer durations. Phase 3 data will be critical to establishing its competitive position.
4. Oral VK2735 (Viking Therapeutics) -- PHASE 2#
Status: Phase 2 complete, Phase 3 expected Q3 2026 Mechanism: Dual GLP-1/GIP receptor agonist peptide Dosing: Once daily oral tablet
VK2735 is the only oral dual GLP-1/GIP agonist in clinical development with reported data:
- VENTURE-Oral: 12.2% weight loss at 13 weeks
- Up to 97% achieved at least 5% weight loss
- Up to 80% achieved at least 10% weight loss
- 99% of GI TEAEs were mild or moderate
- Vomiting reported in 26% vs 10% placebo
Dual agonist advantage: As a dual GLP-1/GIP agonist, oral VK2735 targets two receptors versus the single GLP-1 target of oral semaglutide, orforglipron, and aleniglipron. Injectable dual agonists (tirzepatide) have shown superior weight loss versus GLP-1 monoagonists, suggesting oral VK2735 may ultimately offer a ceiling above oral monoagonists.
Competitive analysis: The 12.2% weight loss at 13 weeks is striking for such a short trial. At the same 13-week timepoint, the SC formulation achieved 14.7%, suggesting the oral form retains most of the injectable's potency. If Phase 3 results over 52-72 weeks show weight loss approaching 20%, oral VK2735 could be transformative.
5. Oral Amycretin (Novo Nordisk) -- PHASE 1#
Status: Phase 1 complete, Phase 2 planning expected Mechanism: Unimolecular GLP-1/amylin receptor co-agonist peptide with SNAC Dosing: Once daily oral tablet (SNAC formulation)
Novo Nordisk's oral amycretin is the earliest-stage but potentially most exciting oral candidate:
- Phase 1: 13.1% weight loss at 12 weeks (highest-dose oral cohort)
- For context, the SC formulation achieved 24.3% at 36 weeks
- Single peptide molecule combining GLP-1 and amylin activity
- Uses SNAC absorption technology (same as oral semaglutide)
Competitive analysis: The 13.1% weight loss at just 12 weeks represents the fastest rate of oral GLP-1 weight loss observed to date (~1.09% per week). If this trajectory is maintained, oral amycretin could potentially achieve 20%+ weight loss at longer timepoints, which would be unprecedented for an oral obesity drug. However, the Phase 1 sample size is small, and tolerability data (82% nausea in SC form) may limit dose escalation.
SNAC limitation: Like oral semaglutide, oral amycretin requires SNAC and will likely need fasting conditions, which reduces its convenience advantage versus small molecules.
6. Oral Ribupatide (Kailera/Hengrui) -- PHASE 2#
Status: Phase 2 complete in China, global development planned Mechanism: Dual GLP-1/GIP receptor agonist peptide Dosing: Once daily oral tablet
Ribupatide is being developed in both injectable (Phase 3 in China) and oral formulations:
- Phase 2 (China): Approximately 12% weight loss at 26 weeks (highest dose)
- More than 50% of highest-dose participants lost at least 10%
- ~38% achieved at least 15% weight loss
- GI side effects were mild to moderate
- Low nausea rates compared to other oral GLP-1 drugs (11.9-22.7%)
Competitive analysis: Ribupatide's oral formulation showed notably lower GI side effect rates than most competitors, which could be a differentiating factor. The 12% weight loss at 26 weeks in a Chinese population suggests competitive efficacy, though cross-population comparisons are limited.
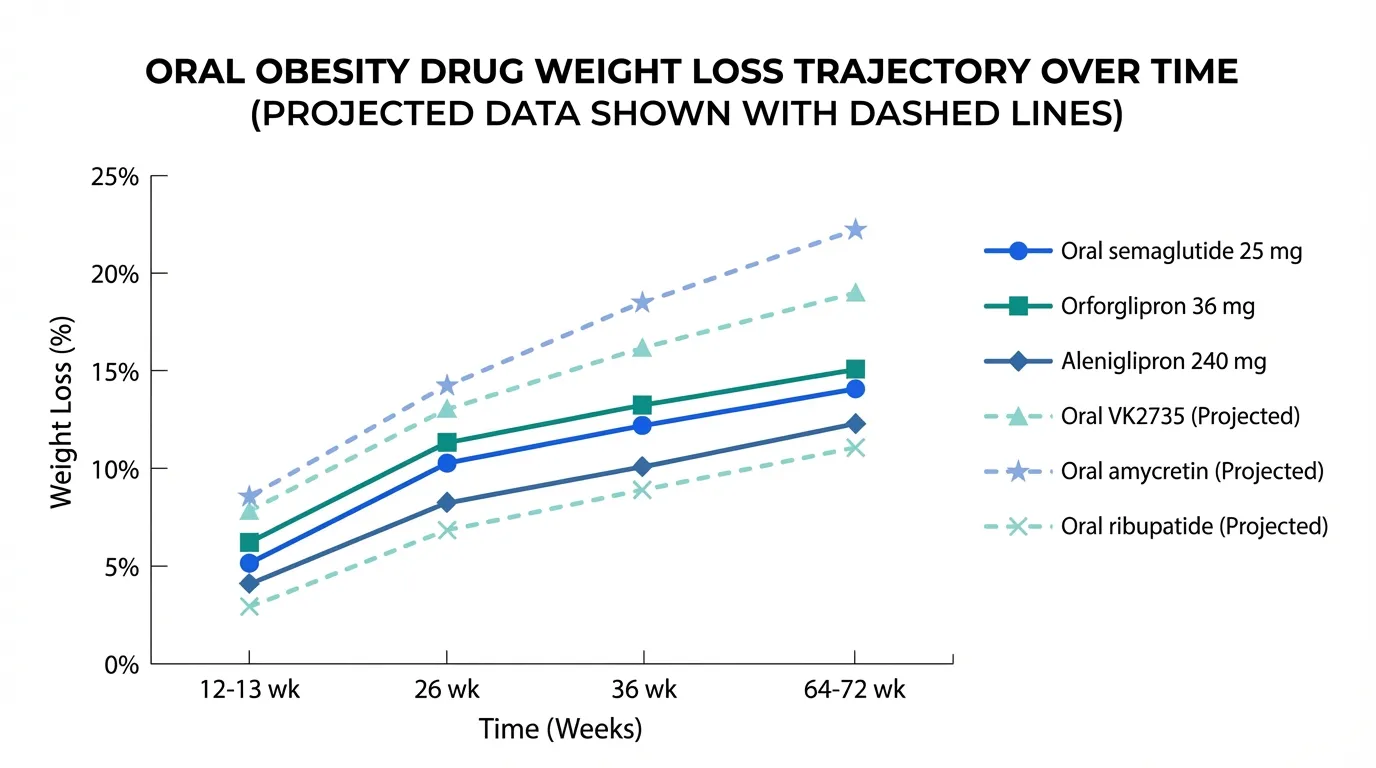
Comparative Analysis#
Efficacy Trajectory Comparison#
| Drug | 12-13 wk | 26 wk | 36 wk | 64-72 wk |
|---|---|---|---|---|
| Oral semaglutide 25 mg | -- | -- | -- | 13.6% |
| Orforglipron 36 mg | -- | -- | -- | 11.2% |
| Aleniglipron 240 mg | -- | -- | 15.3%* | -- |
| Oral VK2735 | 12.2% | -- | -- | -- |
| Oral amycretin | 13.1% | -- | -- | -- |
| Oral ribupatide | -- | ~12% | -- | -- |
*Placebo-adjusted
Convenience Comparison#
| Feature | Oral Semaglutide | Orforglipron | Aleniglipron | Oral VK2735 |
|---|---|---|---|---|
| Food restriction | 30-min fasting | None | None | TBD |
| Formulation | Peptide + SNAC | Small molecule | Small molecule | Peptide |
| Storage | Room temp | Room temp | Room temp | TBD |
| Dose escalation | 8 weeks | TBD | Yes (low start) | TBD |
| Mechanism | GLP-1 | GLP-1 | GLP-1 | GLP-1/GIP |
| Phase | Approved | Phase 3 | Phase 2 | Phase 2 |
Tolerability Comparison#
| Drug | Nausea | Vomiting | AE Discontinuation |
|---|---|---|---|
| Oral semaglutide 25 mg | ~20% | ~8% | ~5% |
| Orforglipron 36 mg | ~30% | ~15% | ~8% |
| Aleniglipron 120 mg | ~65% | ~32% | ~11% |
| Oral VK2735 | ~20% | ~26% | Low |
| Oral amycretin | Not separately reported | Not separately reported | Not separately reported |
| Oral ribupatide 50 mg | ~20% | ~7.5% | Low |
Note: Aleniglipron's high nausea rate may improve with the optimized low-dose initiation protocol.
The Competitive Dynamics#
Novo Nordisk: Two Horses in the Race#
Novo Nordisk has both the only approved oral GLP-1 for obesity (oral semaglutide) and what may be the most potent future oral candidate (oral amycretin). This dual strategy ensures they maintain oral market leadership regardless of which technology (SNAC peptide vs small molecule) ultimately wins.
Eli Lilly: The Non-Peptide Bet#
Lilly is betting on orforglipron's small molecule advantages: no food restrictions, room temperature storage, and simpler manufacturing. While its 72-week weight loss (11.2%) is lower than oral semaglutide, the convenience and cost advantages may win in the broader market.
Structure Therapeutics: The Dark Horse#
Aleniglipron's Phase 2 data (15.3% placebo-adjusted at 36 weeks with the 240 mg dose) is arguably the most impressive oral small molecule result. If Phase 3 confirms these results at longer durations, aleniglipron could challenge both oral semaglutide and orforglipron.
Viking Therapeutics: The Dual Agonist Oral#
VK2735's dual GLP-1/GIP mechanism may give it a ceiling advantage over monoagonist oral drugs. If oral dual agonism can approach injectable tirzepatide's 20.9%, Viking's oral formulation could be category-defining.
Kailera/Hengrui: The Tolerability Play#
Ribupatide's notably lower GI side effect rates and dual agonist mechanism position it as potentially the best-tolerated oral dual agonist.
What Will Define the Winner?#
The oral GLP-1 race will likely be decided by a combination of factors:
- Efficacy -- Can any oral drug approach 20% weight loss? Oral amycretin and VK2735 have the best trajectories.
- Tolerability -- The drug with the best GI tolerability at efficacious doses will have a significant advantage.
- Convenience -- No food restrictions (orforglipron, aleniglipron) vs fasting required (oral semaglutide, amycretin).
- Cost -- Small molecules may be cheaper to manufacture than SNAC-peptide formulations.
- Timing -- First to market captures early share. Oral semaglutide is already approved; orforglipron could follow in 2027.
- Cardiovascular data -- Orforglipron's CV outcomes trials could establish a benefit that differentiates it.
Timeline#
| Milestone | Expected Date |
|---|---|
| Oral semaglutide 25 mg launch | January 2026 (launched) |
| Aleniglipron Phase 3 initiation | Mid-2026 |
| Oral VK2735 Phase 3 initiation | Q3 2026 |
| Orforglipron ATTAIN-2 (T2D) results | 2026 |
| Oral amycretin Phase 2 initiation | TBD |
| Orforglipron potential approval | 2027-2028 (estimated) |
| Aleniglipron potential approval | 2028-2029 (estimated) |
Conclusion#
The GLP-1 pill race is accelerating. With oral semaglutide approved, orforglipron approaching Phase 3 completion, and multiple oral dual agonists in Phase 2, the obesity treatment landscape is about to be fundamentally reshaped by the shift from injection to pill.
The ultimate winner of this race may not be a single drug but rather a portfolio of oral options offering different mechanism profiles, convenience trade-offs, and price points. For patients, the emergence of multiple oral options means greater access, more choice, and potentially lower costs for GLP-1-based obesity treatment.
This article is for educational and informational purposes only. It does not constitute medical advice. Consult a healthcare provider for treatment decisions.
References#
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety
- Orforglipron Overview and Research Guide
- Orforglipron Dosing Protocols
- Orforglipron Side Effects and Safety
- Aleniglipron Overview and Research Guide
- Aleniglipron Dosing Protocols
- Aleniglipron Side Effects and Safety
- VK2735 Overview and Research Guide
- VK2735 Dosing Protocols
- VK2735 Side Effects and Safety
- Ribupatide Overview and Research Guide
- Ribupatide Dosing Protocols
- Ribupatide Side Effects and Safety
- Amycretin Overview and Research Guide
- Amycretin Dosing Protocols
- Amycretin Side Effects and Safety

{kind=link}
Frequently Asked Questions About The GLP-1 Pill Race: Every Oral Obesity Drug in Development
What does this article cover?
A comprehensive guide to every oral GLP-1 obesity drug in development, from approved oral semaglutide to pipeline agents orforglipron, aleniglipron, VK2735, ribupatide, and amycretin. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Semaglutide, Orforglipron, Aleniglipron, VK2735, Ribupatide, Amycretin. Key context: Semaglutide (First and only approved oral GLP-1 for obesity (25 mg daily), uses SNAC absorption enhancer); Orforglipron (Leading oral non-peptide small molecule GLP-1 agonist in Phase 3, no food restrictions); Aleniglipron (Oral small molecule GLP-1 agonist with competitive Phase 2 data, Phase 3 planned mid-2026). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "The GLP-1 Pill Race: Every Oral Obesity Drug in Development." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: First and only approved oral GLP-1 for obesity (25 mg daily), uses SNAC absorption enhancer. Leading oral non-peptide small molecule GLP-1 agonist in Phase 3, no food restrictions. Oral small molecule GLP-1 agonist with competitive Phase 2 data, Phase 3 planned mid-2026. These takeaways are based on the research data available at the time of publication.
What is Semaglutide and why is it significant?
Semaglutide is a peptide discussed in this article because: First and only approved oral GLP-1 for obesity (25 mg daily), uses SNAC absorption enhancer. For a complete profile of Semaglutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Oral vs Injectable GLP-1 Drugs: The Complete Comparison
A head-to-head comparison of oral and injectable GLP-1 drugs for obesity, including oral semaglutide, orforglipron, aleniglipron, and VK2735 versus their injectable counterparts.

GLP-1 Drugs Ranked by Weight Loss: 2026 Data Comparison
Every GLP-1 and incretin drug ranked by clinical weight loss data as of 2026, from retatrutide at 28.7% to oral orforglipron at 11.2%, with comparison tables and trial details.

Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained
A comprehensive guide to every GLP-1 receptor agonist drug, from FDA-approved semaglutide and tirzepatide to pipeline therapies like retatrutide, amycretin, MariTide, and oral orforglipron.
You Might Also Like
Related content you may find interesting