Peptides for Men's Sexual Health: PT-141, Kisspeptin, and Emerging Options

Introduction#
Male sexual dysfunction encompasses a spectrum of conditions — from erectile dysfunction (ED) affecting an estimated 30 million men in the United States to hypoactive sexual desire disorder (HSDD), premature ejaculation, and orgasmic disorders. While PDE5 inhibitors (sildenafil, tadalafil) revolutionized ED treatment by targeting peripheral vascular mechanisms, they do not address desire, and approximately 30-40% of men with ED do not respond adequately to these medications.
Peptides offer mechanistically distinct approaches to male sexual health. Some act centrally in the brain to modulate desire and arousal pathways. Others support the hormonal axis that underpins sexual function. Two peptides discussed in this guide — alprostadil and PT-141 — hold FDA approvals for sexual dysfunction indications, though PT-141's approval is currently limited to women. The remaining compounds are in various stages of clinical investigation.
This guide reviews the evidence for each peptide, clearly distinguishing between FDA-approved therapies, compounds with clinical trial data, and those with only preclinical or early-phase evidence. For the broader landscape of sexual health peptides including female-specific applications, see Peptides for Sexual Health.
Important note: Sexual dysfunction in men frequently has multiple contributing factors including cardiovascular disease, diabetes, hormonal imbalances, neurological conditions, medications, and psychological factors. A thorough medical evaluation should precede any treatment approach.
Understanding Male Sexual Function#
Male sexual function involves the coordinated interplay of several systems:
- Central desire pathways — sexual motivation originates in the hypothalamus and limbic system, modulated by dopamine, melanocortins, oxytocin, and kisspeptin. These pathways determine whether a man experiences sexual desire
- Hormonal axis — the hypothalamic-pituitary-gonadal (HPG) axis produces testosterone via GnRH, LH, and FSH signaling. Testosterone is necessary (though not sufficient) for normal libido and erectile function
- Peripheral vascular mechanisms — erection requires nitric oxide-mediated smooth muscle relaxation in the corpus cavernosum, increasing blood flow. PDE5 inhibitors and alprostadil act at this level
- Neurological integration — autonomic nervous system signaling coordinates arousal, erection, emission, and ejaculation
Different peptides target different levels of this system, which is why understanding the mechanism is essential for evaluating their relevance.
1. PT-141 (Bremelanotide)#
Evidence Level: FDA-approved for HSDD in premenopausal women; Phase 2 data for male ED Primary Mechanism: Melanocortin-4 receptor (MC4R) agonist in the central nervous system FDA Status: Approved as Vyleesi for female HSDD; not approved for male indications
Mechanism in Male Sexual Function#
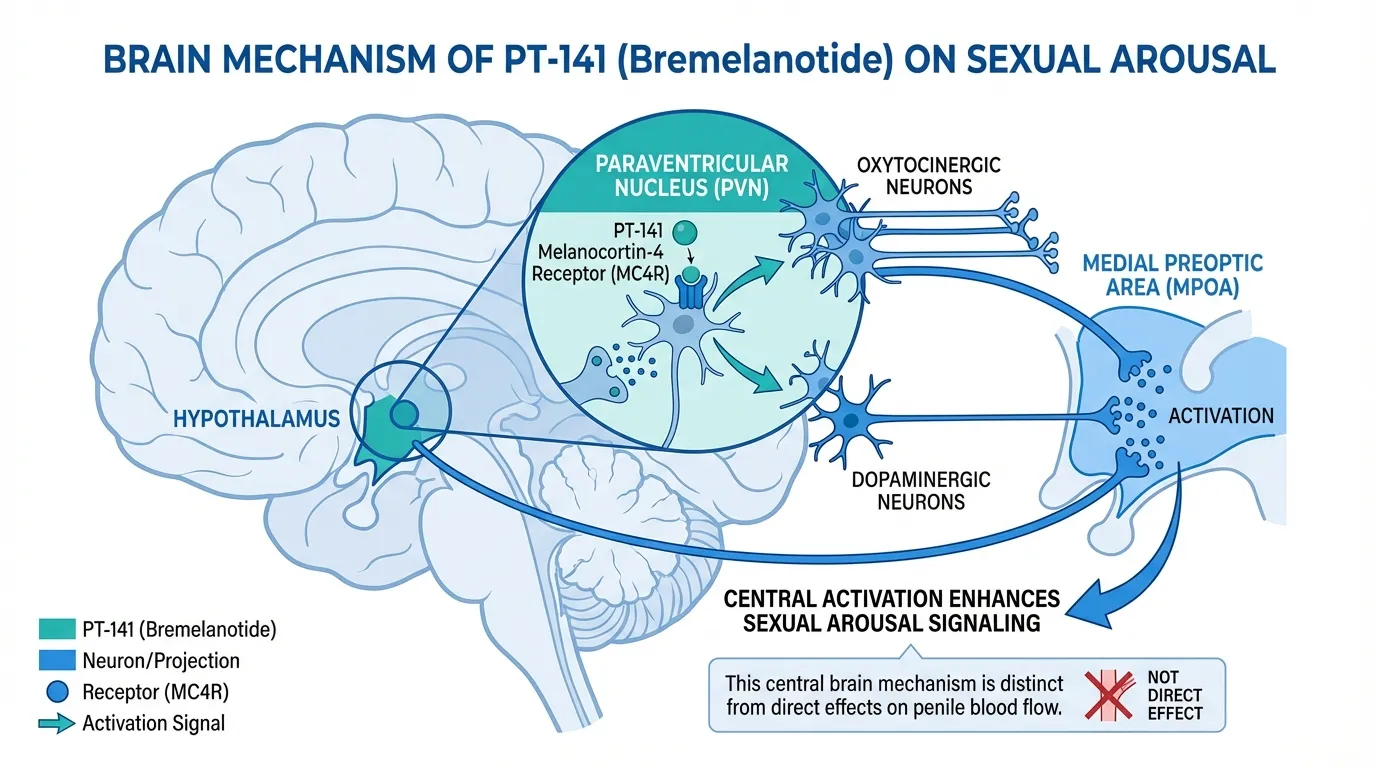
PT-141 activates MC4R in the hypothalamus, a receptor positioned at the intersection of appetite regulation and sexual motivation pathways. In the paraventricular nucleus, MC4R activation triggers downstream signaling through oxytocinergic and dopaminergic neurons that project to the medial preoptic area — the brain region most consistently linked to male sexual motivation across mammalian species.
This central mechanism is fundamentally different from PDE5 inhibitors. PT-141 does not directly affect penile blood flow. Instead, it enhances the brain's sexual arousal signaling, which then facilitates the normal physiological cascade leading to erection. This distinction has a practical implication: PT-141 may be effective in men whose ED has a significant psychogenic or desire-related component, even when PDE5 inhibitors have failed.
Clinical Evidence in Men#
PT-141's clinical development ultimately focused on the female HSDD indication, but several studies evaluated the compound in men:
- Phase 2 erectile dysfunction trial — a double-blind, placebo-controlled study in men with ED demonstrated that PT-141 (administered intranasally at the time) produced statistically significant improvements in erectile response compared to placebo. Notably, 3 of 6 men who had previously failed sildenafil responded to PT-141, suggesting a non-overlapping mechanism
- Psychogenic ED — PT-141 showed particular efficacy in men with psychogenic ED, consistent with its central rather than peripheral mechanism of action
- On-demand dosing — single-dose administration produced effects within 30-60 minutes, with duration sufficient for sexual activity
Why PT-141 Is Not Approved for Men#
Despite positive Phase 2 data, the clinical program for male ED was not advanced to Phase 3 trials. Several factors contributed to this decision. The competitive landscape for male ED was already crowded with PDE5 inhibitors. The intranasal formulation initially studied in men had variable bioavailability. Additionally, the nausea rate (approximately 18% in male studies) presented a commercial challenge in a market where oral PDE5 inhibitors were well-tolerated.
The subcutaneous formulation that ultimately gained FDA approval for female HSDD was not formally studied in large-scale male ED trials.
Side Effects#
PT-141's side effect profile in men includes nausea (the most common adverse event), facial flushing, headache, and transient blood pressure elevation. These effects are consistent across male and female study populations and reflect the broad CNS activity of melanocortin receptor activation.
2. Kisspeptin#
Evidence Level: Clinical research studies (not approved for sexual health) Primary Mechanism: Activation of hypothalamic GnRH neurons; modulation of sexual arousal circuits FDA Status: Investigational
Mechanism in Male Sexual Function#
Kisspeptin is a hypothalamic neuropeptide best known for its role as the master regulator of the HPG axis — it directly activates GnRH neurons in the hypothalamus, triggering the hormonal cascade that produces LH, FSH, and ultimately testosterone. However, kisspeptin neurons also project to brain regions involved in sexual behavior, including the medial amygdala and bed nucleus of the stria terminalis, areas that integrate olfactory, emotional, and sexual information.
This dual role — hormonal regulation plus behavioral modulation — makes kisspeptin a unique peptide at the intersection of reproductive endocrinology and sexual neuroscience. For more on kisspeptin's role in reproductive hormone regulation, see Kisspeptin and Fertility Peptides.
Clinical Evidence in Men#
Research from Imperial College London has produced the most significant human data on kisspeptin and male sexual function:
- Brain activation studies — kisspeptin-54 infusion enhanced brain activation in regions associated with sexual arousal when healthy men viewed sexual imagery, as measured by functional MRI. The anterior cingulate cortex and posterior cingulate cortex showed particular enhancement
- Penile tumescence — kisspeptin administration enhanced penile tumescence in response to sexual stimulation in healthy male volunteers, suggesting a facilitation of the physiological arousal response
- Negative mood reduction — kisspeptin reduced negative mood associated with sexual stimuli, potentially relevant for men with psychogenic sexual dysfunction or sexual aversion
- Hormonal effects — kisspeptin robustly stimulates LH and testosterone secretion, which could provide a secondary mechanism for improving sexual function in men with borderline hypogonadism
Limitations#
Kisspeptin-54 has a very short half-life (approximately 28 minutes), making it impractical for therapeutic use in its native form. The studies cited above used continuous intravenous infusion, a format unsuitable for clinical application. Longer-acting kisspeptin analogs such as MVT-602 are being developed to address this limitation. The relationship between kisspeptin's hormonal effects and its psychosexual effects has not been fully dissected — it remains unclear whether these effects can be independently modulated.
3. Alprostadil#
Evidence Level: FDA-approved for erectile dysfunction Primary Mechanism: Prostaglandin E1 (PGE1); peripheral vasodilation of erectile tissue FDA Status: Approved (Caverject, Edex for intracavernosal injection; MUSE for intraurethral)
Mechanism in Male Sexual Function#
Alprostadil is a synthetic form of prostaglandin E1 that acts directly on smooth muscle cells in the corpus cavernosum. By activating EP2 and EP4 prostanoid receptors, alprostadil increases intracellular cAMP, which causes smooth muscle relaxation and arterial vasodilation in penile tissue. This mechanism is independent of sexual arousal — alprostadil produces erection through direct pharmacological action on erectile tissue, bypassing the need for CNS-mediated arousal signals.
This purely peripheral mechanism means alprostadil works regardless of the cause of ED — neurogenic, vasculogenic, psychogenic, or mixed. It is effective in men who do not respond to PDE5 inhibitors, including those with severe vascular disease or post-prostatectomy nerve damage.
Clinical Evidence#
Alprostadil has one of the longest track records of any ED treatment:
- Intracavernosal injection — the gold standard for ED that does not respond to oral therapy. Response rates exceed 80% across diverse ED etiologies. Alprostadil (Caverject/Edex) was FDA-approved in 1995 for intracavernosal injection
- Intraurethral administration — the MUSE (Medicated Urethral System for Erection) delivery system provides a needle-free alternative. Efficacy is lower than injection (approximately 43% successful intercourse rate vs. 70%+ for injection) but acceptable for men who prefer non-injection options
- Combination therapy — alprostadil can be combined with PDE5 inhibitors in men with severe or refractory ED, as the mechanisms are complementary (cAMP elevation via alprostadil plus cGMP preservation via PDE5 inhibitors)
- Post-prostatectomy — alprostadil is particularly valued in men with ED following radical prostatectomy, where nerve damage may prevent response to oral medications
Side Effects#
The primary side effect of intracavernosal alprostadil is penile pain at the injection site (reported in 11-44% of patients depending on the study). Prolonged erection (priapism) occurs in approximately 1-3% of patients and requires medical attention if lasting more than 4 hours. Penile fibrosis (scar tissue formation) can develop with repeated injection, reported in 2-12% of long-term users. Intraurethral alprostadil causes urethral discomfort in approximately 24-32% of users.
4. Gonadorelin#
Evidence Level: FDA-approved for diagnostic use; clinical data for therapeutic applications Primary Mechanism: GnRH agonist; pulsatile stimulation of pituitary LH and FSH release FDA Status: Approved for diagnostic use (Factrel); therapeutic use is off-label
Mechanism in Male Sexual Function#
Gonadorelin is a synthetic form of gonadotropin-releasing hormone (GnRH), the hypothalamic peptide that controls the entire HPG axis. When administered in a pulsatile fashion (mimicking the natural secretory pattern), gonadorelin stimulates the anterior pituitary to release LH and FSH. LH then stimulates Leydig cells in the testes to produce testosterone, while FSH supports spermatogenesis.
Gonadorelin's relevance to male sexual health is indirect but important: it supports endogenous testosterone production. In men with secondary hypogonadism (hypothalamic or pituitary dysfunction causing low testosterone), pulsatile gonadorelin can restore normal testosterone levels while preserving fertility — a significant advantage over exogenous testosterone, which suppresses the HPG axis and can cause infertility.
Clinical Applications#
- Diagnostic testing — the GnRH stimulation test uses gonadorelin to assess pituitary responsiveness, helping distinguish between hypothalamic and pituitary causes of hypogonadism
- Secondary hypogonadism — pulsatile gonadorelin delivered via programmable pump has restored testosterone production and fertility in men with hypothalamic hypogonadism, including Kallmann syndrome
- Testosterone therapy adjunct — some clinicians use low-dose gonadorelin alongside testosterone replacement to maintain some HPG axis activity and testicular function, though evidence for this approach is limited to clinical experience rather than randomized trials
- Post-cycle recovery — in the context of recovery from anabolic steroid use, gonadorelin (along with HCG) has been used to restart suppressed endogenous testosterone production
Limitations#
Pulsatile GnRH therapy requires a programmable infusion pump and is impractical for most outpatient settings. Continuous (non-pulsatile) administration of gonadorelin actually suppresses the HPG axis through receptor downregulation — the same mechanism used by GnRH agonists like triptorelin for prostate cancer treatment. This means the dosing pattern is critical: pulsatile administration stimulates testosterone production, while continuous administration suppresses it.
5. HCG (Human Chorionic Gonadotropin)#
Evidence Level: FDA-approved for hypogonadism; extensive clinical experience Primary Mechanism: LH receptor agonist; direct stimulation of testicular testosterone production FDA Status: Approved for hypogonadotropic hypogonadism and cryptorchidism
Mechanism in Male Sexual Function#
HCG is a glycoprotein hormone that shares structural homology with LH and binds to the same receptor on testicular Leydig cells. By directly stimulating the LH receptor, HCG increases intratesticular testosterone production without requiring hypothalamic or pituitary signaling. This makes HCG effective even when the upper levels of the HPG axis are suppressed — for example, during exogenous testosterone therapy.
Clinical Applications for Sexual Health#
HCG's relevance to male sexual health operates through testosterone support:
- Hypogonadotropic hypogonadism — HCG is FDA-approved for men whose low testosterone results from insufficient pituitary LH secretion. By replacing the LH signal directly, HCG restores testicular testosterone production
- Testosterone therapy adjunct — HCG is widely used alongside exogenous testosterone to prevent testicular atrophy and maintain intratesticular testosterone levels, which are important for spermatogenesis and local paracrine signaling
- Fertility preservation — unlike exogenous testosterone (which suppresses sperm production by eliminating the intratesticular testosterone gradient needed for spermatogenesis), HCG maintains this gradient. Men concerned about fertility while treating low testosterone often use HCG either alone or in combination with testosterone
- Testosterone recovery — HCG can jumpstart testosterone production in men discontinuing testosterone therapy, bridging the period before endogenous HPG axis function recovers
Side Effects#
HCG side effects include injection site reactions, headache, irritability, and breast tenderness (gynecomastia) due to increased aromatization of testosterone to estradiol. Estradiol elevations require monitoring and may necessitate aromatase inhibitor co-administration in some men. HCG can also cause fluid retention.
6. Oxytocin#
Evidence Level: Well-characterized endogenous physiology; mixed clinical data for sexual applications Primary Mechanism: Oxytocin receptor activation in the CNS and periphery FDA Status: Approved for obstetric indications (Pitocin); not approved for sexual health
Mechanism in Male Sexual Function#
Oxytocin is released during sexual arousal and peaks at orgasm in both men and women. In male sexual physiology, oxytocin has several documented roles. Centrally, oxytocinergic neurons in the paraventricular nucleus project to the spinal cord and contribute to the erectile reflex. Peripherally, oxytocin is present in the male reproductive tract and may facilitate ejaculation by acting on smooth muscle in the vas deferens and seminal vesicles.
Oxytocin also interacts with other systems relevant to sexual function. It modulates dopaminergic signaling in reward circuits, potentially enhancing the pleasurable aspects of sexual activity. It facilitates pair bonding and social attachment, which influence relationship satisfaction and, indirectly, sexual desire.
Clinical Evidence in Men#
Research on exogenous oxytocin for male sexual function has produced mixed results:
- Erectile response — some studies of intranasal oxytocin have reported modest improvements in erectile response, though the effect sizes have been small and inconsistent across trials
- Orgasm and ejaculation — given oxytocin's established role in orgasm physiology, intranasal oxytocin has been explored for ejaculatory disorders. Results have been preliminary and inconclusive
- Social-sexual behavior — intranasal oxytocin has been shown to increase the perceived attractiveness of partners, enhance empathy during sexual interactions, and modify social approach behavior in ways that could indirectly benefit sexual relationships
- Context dependence — oxytocin's effects on male sexual function appear highly context-dependent, influenced by relationship status, attachment style, and the social environment. This variability complicates clinical application
Limitations#
The critical question with intranasal oxytocin is whether sufficient peptide reaches the relevant brain regions. Oxytocin does not cross the blood-brain barrier efficiently, and the extent to which intranasal delivery achieves pharmacologically relevant CNS concentrations remains debated. The mixed clinical results may partly reflect inadequate CNS penetration rather than a lack of biological activity. Oxytocin is not approved for any sexual health indication, and self-administration for sexual enhancement is not supported by current evidence.
How These Peptides Compare#
| Feature | PT-141 | Kisspeptin | Alprostadil | Gonadorelin | HCG | Oxytocin |
|---|---|---|---|---|---|---|
| Target | MC4R (CNS desire) | GnRH neurons + arousal | PGE1 receptors (penile) | GnRH receptor (pituitary) | LH receptor (testicular) | OT receptor (CNS/peripheral) |
| Mechanism Level | Central (desire) | Central (hormonal + arousal) | Peripheral (vascular) | Hormonal axis | Hormonal axis | Central + peripheral |
| FDA Status (male) | Not approved | Investigational | Approved (ED) | Approved (diagnostic) | Approved (hypogonadism) | Not approved |
| Evidence Quality | Phase 2 RCTs | Small clinical studies | Phase 3 RCTs | Established clinical use | Established clinical use | Mixed clinical data |
| Administration | SC injection | IV infusion (research) | Intracavernosal/intraurethral | SC/IV (pulsatile) | SC/IM injection | Intranasal (research) |
| Primary Sexual Effect | Desire/arousal | Arousal facilitation | Erection (mechanical) | Testosterone support | Testosterone support | Bonding/orgasm |
Combining Approaches#
Male sexual dysfunction often involves multiple contributing factors, which is why combination strategies may be more effective than single-agent therapy:
- Central + peripheral — addressing both desire (PT-141 or kisspeptin, investigational) and erectile mechanics (alprostadil or PDE5 inhibitors) could theoretically benefit men with mixed psychogenic and vasculogenic ED
- Hormonal optimization + symptomatic treatment — restoring testosterone with HCG or gonadorelin while using on-demand ED medications addresses the hormonal foundation while providing immediate symptom relief
- Caution on combinations — most peptide combinations for sexual health have not been studied in formal clinical trials. Combining agents that affect blood pressure (PT-141 with alprostadil, for example) could theoretically increase cardiovascular risk
Practical Considerations#
Evidence Hierarchy#
Readers should understand the significant differences in evidence quality among these compounds:
- FDA-approved for male sexual health: Alprostadil (intracavernosal and intraurethral for ED)
- FDA-approved for related male indications: HCG (hypogonadism), gonadorelin (diagnostic)
- FDA-approved but not for men: PT-141 (approved for female HSDD only)
- Investigational with clinical data: Kisspeptin (small clinical studies in men)
- Investigational with mixed data: Oxytocin (intranasal studies with inconsistent results)
When to Consider Peptide-Based Approaches#
Peptides may be relevant for men who have not responded to first-line therapies (PDE5 inhibitors), have contraindications to conventional treatments, have a desire-predominant rather than arousal-predominant dysfunction, need to preserve fertility while addressing hypogonadal symptoms, or have psychogenic components to their dysfunction.
What Peptides Do Not Replace#
Peptides are not substitutes for addressing underlying causes of sexual dysfunction. Cardiovascular risk factor management, diabetes control, medication review, psychological counseling, relationship therapy, and lifestyle modifications (exercise, sleep, stress management) remain foundational. Peptides should be considered as potential components of a comprehensive approach, not standalone solutions.
Future Directions#
Several developments may expand the role of peptides in male sexual health:
- Longer-acting kisspeptin analogs — compounds like MVT-602 could make kisspeptin's effects therapeutically practical, overcoming the short half-life limitation of native kisspeptin-54
- PT-141 for male indications — formal Phase 3 trials of subcutaneous PT-141 in men with ED or HSDD could lead to approval for male indications
- Selective melanocortin agonists — next-generation MC4R agonists with improved nausea profiles could improve tolerability
- Oral formulations — development of orally bioavailable peptide analogs would significantly improve patient acceptance and compliance
Conclusion#
Peptides offer mechanistically diverse approaches to male sexual health that complement — rather than replace — existing therapies. Alprostadil stands as the established FDA-approved peptide option for male ED, working through direct peripheral vasodilation. PT-141 provides a unique central mechanism targeting desire pathways, with clinical evidence in men that did not progress to approval. HCG and gonadorelin support the hormonal foundation of sexual function by maintaining testosterone production. Kisspeptin and oxytocin represent emerging areas where brain-level modulation of sexual arousal is being explored.
The diversity of mechanisms — from peripheral vascular effects to central desire pathways to hormonal axis support — reflects the complexity of male sexual function itself and argues against a one-size-fits-all approach to treatment.
For related content, see Peptides for Sexual Health, Kisspeptin and Fertility Peptides, and the Alprostadil vs PT-141 comparison. For dosing tools, visit the Dosing Calculator.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Alprostadil Overview and Research Guide
- Alprostadil Dosing Protocols
- Alprostadil Side Effects and Safety
- Gonadorelin Overview and Research Guide
- Gonadorelin Dosing Protocols
- Gonadorelin Side Effects and Safety
- HCG Overview and Research Guide
- HCG Dosing Protocols
- HCG Side Effects and Safety
- Oxytocin Overview and Research Guide
- Oxytocin Dosing Protocols
- Oxytocin Side Effects and Safety
- PT-141 Overview and Research Guide
- PT-141 Dosing Protocols
- PT-141 Side Effects and Safety

{kind=link}
Frequently Asked Questions About Peptides for Men's Sexual Health: PT-141, Kisspeptin, and Emerging Options
What does this article cover?
Guide to peptides researched for male sexual health including PT-141, kisspeptin, gonadorelin, HCG, alprostadil, and oxytocin with evidence levels. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Alprostadil, Gonadorelin, HCG, Oxytocin, PT-141. Key context: Alprostadil (FDA-approved prostaglandin E1 analog for erectile dysfunction via intracavernosal or intraurethra...); Gonadorelin (GnRH analog used diagnostically and therapeutically to support endogenous testosterone production...); HCG (LH analog that stimulates testicular testosterone production and maintains fertility during testo...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Peptides for Men's Sexual Health: PT-141, Kisspeptin, and Emerging Options." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: FDA-approved prostaglandin E1 analog for erectile dysfunction via intracavernosal or intraurethra.... GnRH analog used diagnostically and therapeutically to support endogenous testosterone production.... LH analog that stimulates testicular testosterone production and maintains fertility during testo.... These takeaways are based on the research data available at the time of publication.
What is Alprostadil and why is it significant?
Alprostadil is a peptide discussed in this article because: FDA-approved prostaglandin E1 analog for erectile dysfunction via intracavernosal or intraurethral administration. For a complete profile of Alprostadil, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Reproductive Health Peptides: A Research Roundup
Peptides for reproductive health — kisspeptin, gonadorelin, HCG, HMG, triptorelin, and PT-141 — with evidence levels and clinical status.

What Peptides Are FDA Approved? The Complete List (2026)
Complete list of FDA-approved peptide drugs with brand names, indications, and approval dates. Updated March 2026 with the RFK Jr. Category 1 reclassification of 14 peptides for compounding pharmacy access.

Peptides for Sexual Health: PT-141, Kisspeptin, and Beyond
Peptides for sexual health — PT-141, kisspeptin, Melanotan-2, and oxytocin — covering mechanisms, clinical evidence, and safety data.
You Might Also Like
Related content you may find interesting