Alprostadil vs PT-141: Peripheral Vasodilator vs Central Desire Pathway
Alprostadil vs PT-141 compared across mechanism, efficacy, side effects, dosing, and clinical applications for sexual dysfunction treatment.
Verdict at a Glance
Alprostadil and PT-141 target fundamentally different aspects of sexual dysfunction and are not direct competitors. Alprostadil is the established choice for male erectile dysfunction, producing reliable erections through direct peripheral vasodilation regardless of the underlying cause. PT-141 addresses the central desire deficit that PDE5 inhibitors and alprostadil cannot reach, making it uniquely relevant for hypoactive sexual desire disorder. The choice depends entirely on the clinical problem — mechanical erectile failure versus diminished sexual desire — and in some cases both mechanisms may be complementary.
| Best for | Pick | Why |
|---|---|---|
| Male erectile dysfunction unresponsive to PDE5 inhibitors | Alprostadil | Direct peripheral vasodilation produces erections independent of CNS arousal, with over 80% response rate across all ED etiologies |
| Hypoactive sexual desire disorder (clinical) | PT-141 | Only FDA-approved treatment targeting central desire pathways through MC4R activation in the hypothalamus |
| Post-prostatectomy erectile dysfunction | Alprostadil | Neurogenic ED after prostatectomy responds well to direct smooth muscle relaxation via alprostadil when nerve-dependent mechanisms are impaired |
| Psychogenic sexual dysfunction with desire component | PT-141 | Central mechanism addresses the brain-level desire deficit that characterizes psychogenic dysfunction better than peripheral vasodilators |
| Combined desire and erectile dysfunction | Alprostadil | Alprostadil is the only FDA-approved option for men between these two; PT-141 is approved only for female HSDD currently |
| Category | Alprostadil | PT-141 | Advantage |
|---|---|---|---|
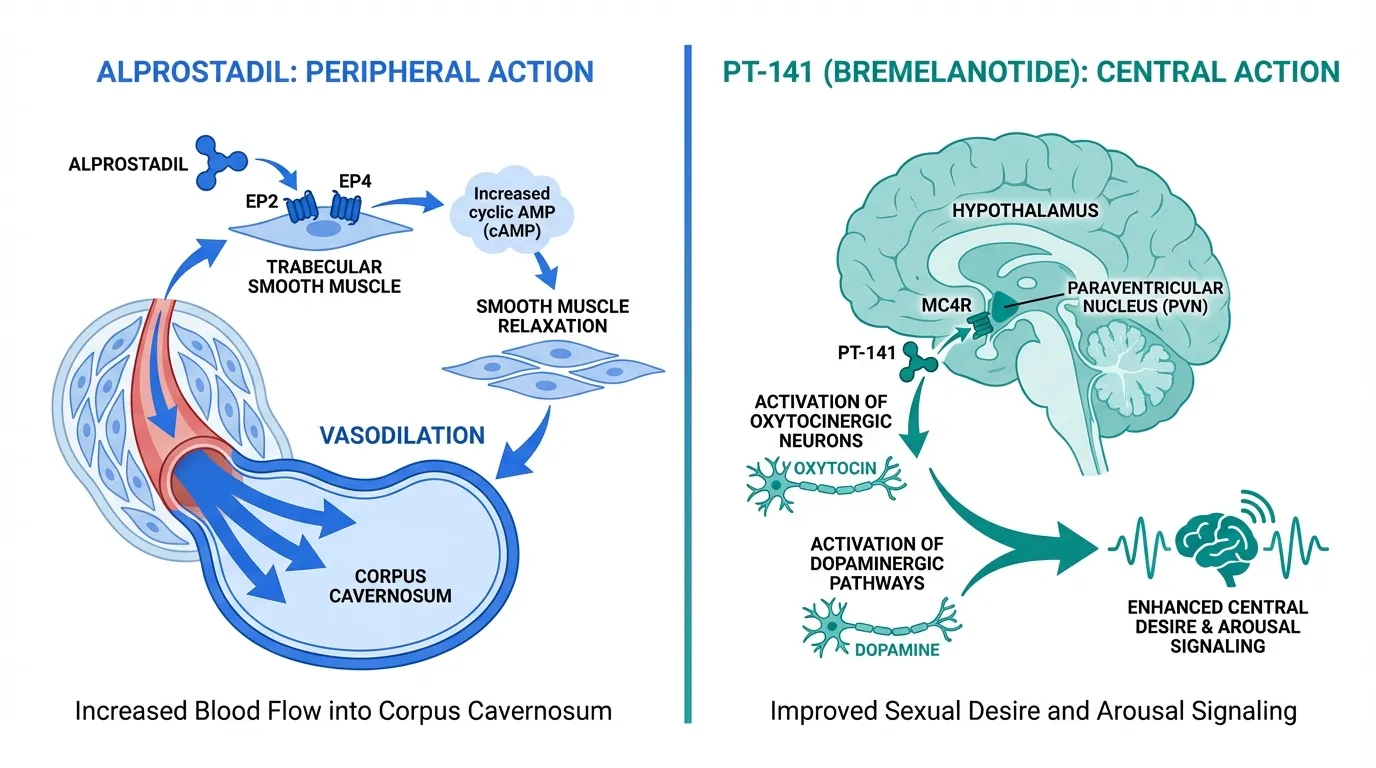
| Mechanism of Action | Prostaglandin E1 analog that activates EP2/EP4 receptors on corpus cavernosum smooth muscle, increasing cAMP to produce direct vasodilation and erection independent of CNS arousal or desire signaling | Melanocortin-4 receptor agonist acting in the hypothalamus to activate central sexual desire and arousal pathways through dopaminergic and oxytocinergic signaling, with no direct peripheral vascular effect | Comparable |
| Clinical Evidence | FDA-approved since 1995 with over 30 years of clinical use for ED; response rates exceed 80% across diverse etiologies including post-prostatectomy and severe vasculogenic ED | FDA-approved in 2019 for female HSDD based on Phase 3 RECONNECT trials; Phase 2 data in male ED showed efficacy including in PDE5 inhibitor non-responders, but male indication not pursued to approval | Alprostadil |
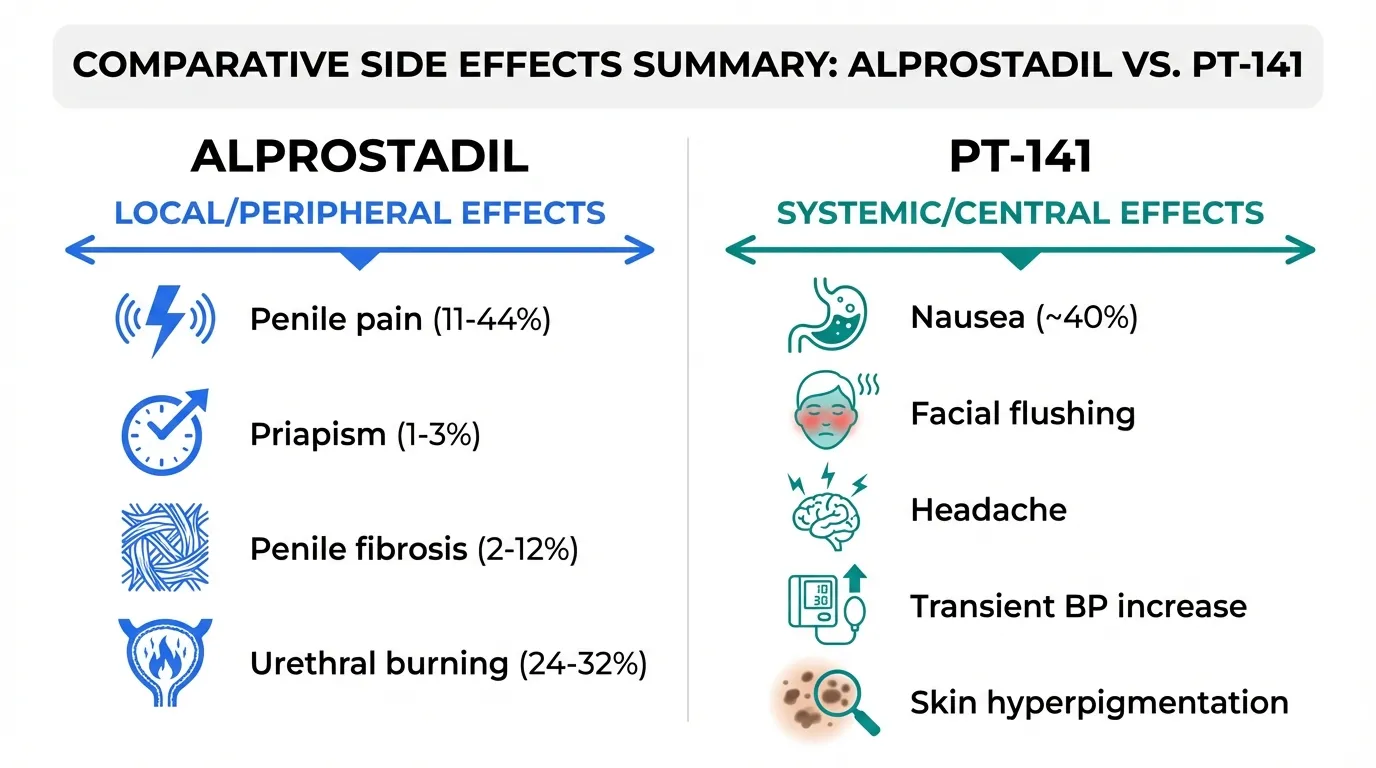
| Side Effect Profile | Penile pain at injection site (11-44%); priapism risk (1-3%) requiring emergency treatment; penile fibrosis with chronic use (2-12%); urethral discomfort with MUSE formulation (24-32%) | Nausea in approximately 40% of patients; transient facial flushing; headache; mild blood pressure elevation; focal skin hyperpigmentation; limited to 8 doses per month per FDA label | Comparable |
| Administration and Dosing | Intracavernosal injection (Caverject/Edex) or intraurethral pellet (MUSE); dose titrated individually from 1.25 to 60 mcg; on-demand use with onset in 5-20 minutes; requires injection technique training | Subcutaneous injection via autoinjector (Vyleesi); fixed 1.75 mg dose; administered at least 45 minutes before anticipated activity; simpler administration but requires advance planning | PT-141 |
| Scope of Application | FDA-approved specifically for male erectile dysfunction across all etiologies including neurogenic, vasculogenic, and mixed; effective as second-line therapy after PDE5 inhibitor failure | FDA-approved for hypoactive sexual desire disorder in premenopausal women; addresses desire rather than arousal or erection; Phase 2 male ED data exists but no male approval; targets a different dimension of sexual dysfunction | Comparable |

Introduction#
Alprostadil and PT-141 are both FDA-approved treatments for sexual dysfunction, yet they could hardly be more different in mechanism, indication, or clinical philosophy. Alprostadil is a prostaglandin E1 analog that produces erection through direct vasodilation of penile tissue — a purely peripheral, mechanical effect. PT-141 (bremelanotide, marketed as Vyleesi) is a melanocortin-4 receptor agonist that acts in the brain to enhance sexual desire — a central nervous system effect with no direct action on erectile tissue.
This mechanistic divergence reflects the fundamental distinction between arousal (the physical response) and desire (the psychological motivation). Most sexual dysfunction treatments, from PDE5 inhibitors to alprostadil, target the arousal side. PT-141 was the first approved therapy to target the desire side, validating the melanocortin pathway as a legitimate therapeutic target.
This comparison examines both compounds across mechanism, evidence, safety, dosing, and clinical utility. For a comparison between PT-141 and its parent compound, see Melanotan-2 vs PT-141.
Quick Comparison#
| Feature | Alprostadil | PT-141 (Bremelanotide) |
|---|---|---|
| Drug Class | Prostaglandin E1 analog | Melanocortin receptor agonist |
| Brand Names | Caverject, Edex, MUSE | Vyleesi |
| FDA Approval | 1995 (ED in men) | 2019 (HSDD in premenopausal women) |
| Mechanism Level | Peripheral (penile vasculature) | Central (hypothalamic desire circuits) |
| Primary Effect | Erection (mechanical) | Sexual desire (motivational) |
| Administration | Intracavernosal injection or intraurethral | Subcutaneous autoinjector |
| Onset | 5-20 minutes | 45+ minutes |
| Primary Receptor | EP2/EP4 prostanoid receptors | MC4R melanocortin receptor |
Mechanism of Action Comparison#
Alprostadil#
Alprostadil is a synthetic form of prostaglandin E1 (PGE1), an endogenous lipid mediator. When injected directly into the corpus cavernosum (the erectile tissue of the penis) or administered intraurethrally, alprostadil activates EP2 and EP4 prostanoid receptors on smooth muscle cells. This activates adenylyl cyclase, increasing intracellular cyclic AMP (cAMP), which causes smooth muscle relaxation, arterial vasodilation, and increased blood flow into the lacunar spaces of the corpus cavernosum.
The result is a mechanically induced erection that occurs independently of:
- Sexual desire or psychological arousal
- Central nervous system signaling
- Intact cavernosal nerve function
- Endothelial nitric oxide production (the pathway targeted by PDE5 inhibitors)
This independence from upstream signaling is both alprostadil's greatest strength (it works regardless of ED etiology) and its conceptual limitation (it addresses the mechanics of erection without affecting desire).
PT-141#
PT-141 is a cyclic heptapeptide that activates melanocortin-4 receptors (MC4R) in the paraventricular nucleus of the hypothalamus. MC4R-expressing neurons in this region project to brainstem autonomic centers and interface with mesolimbic dopaminergic pathways — the reward and motivation circuitry that underpins sexual desire.
The mechanism proceeds through several steps:
- MC4R activation in the hypothalamus
- Downstream stimulation of oxytocinergic neurons projecting to the spinal cord
- Activation of dopaminergic signaling in the medial preoptic area
- Enhanced central sexual arousal and desire signaling
- Facilitation (not direct induction) of the normal physiological arousal cascade
Unlike alprostadil, PT-141 does not produce a purely mechanical response. It enhances the brain's disposition toward sexual arousal, which can then facilitate the normal downstream cascade including erection. This means PT-141's effects are more context-dependent — they are most apparent when there is sexual stimulation or context present.
Evidence and Clinical Data#
Alprostadil Clinical Evidence#
Alprostadil has the more extensive evidence base, reflecting three decades of clinical use:
- Intracavernosal efficacy — response rates (defined as erection sufficient for intercourse) exceed 80% across diverse ED populations, including men with diabetes, cardiovascular disease, post-prostatectomy status, and spinal cord injury
- MUSE efficacy — the intraurethral formulation shows lower response rates (approximately 43% successful intercourse) but provides a needle-free alternative
- PDE5 inhibitor failures — alprostadil is effective in approximately 50-60% of men who do not respond to oral PDE5 inhibitors, making it the standard second-line therapy
- Long-term data — studies with follow-up exceeding 5 years demonstrate sustained efficacy, though dropout rates of 30-50% reflect the burden of injection-based treatment
- Combination data — alprostadil can be combined with PDE5 inhibitors or other vasoactive agents (papaverine, phentolamine in "trimix" formulations) for refractory cases
PT-141 Clinical Evidence#
PT-141's clinical data spans both female and male populations:
- RECONNECT trials (female) — two Phase 3 pivotal trials in premenopausal women with HSDD showed statistically significant improvements in the Female Sexual Function Index desire domain and reductions in distress scores compared to placebo. These trials led to FDA approval
- Male ED Phase 2 — double-blind, placebo-controlled studies in men demonstrated that PT-141 improved erectile response measured by RigiScan, with efficacy in a subset of men who had not responded to sildenafil
- Functional neuroimaging — fMRI studies confirmed that PT-141 activates brain regions associated with sexual arousal, providing direct evidence of its central mechanism
- Dose-response — clinical studies established the 1.75 mg subcutaneous dose as the optimal balance of efficacy and tolerability
Evidence Gap#
The evidence profiles differ both in depth and in indication. Alprostadil has decades of real-world use data in millions of men for its approved indication. PT-141 has rigorous Phase 3 data for female HSDD but only Phase 2 data for male sexual dysfunction, and its approved indication does not include men.
Side Effect Comparison#
Alprostadil Side Effects#
Alprostadil's side effects are predominantly local, reflecting its route of administration:
- Penile pain — the most common adverse effect of intracavernosal injection, reported in 11-44% of patients. Pain is typically mild to moderate, dose-dependent, and tends to diminish with continued use
- Priapism — prolonged erection lasting more than 4-6 hours occurs in approximately 1-3% of patients. Priapism is a medical emergency requiring intervention (aspiration, phenylephrine injection) to prevent permanent tissue damage
- Penile fibrosis — repeated injection can cause fibrous plaque formation in the tunica albuginea, reported in 2-12% of long-term users. This can lead to penile curvature (Peyronie's-like changes)
- Urethral effects — the MUSE formulation causes urethral burning or discomfort in 24-32% of users, with occasional urethral bleeding
- Systemic effects — rare; mild hypotension and dizziness reported infrequently
PT-141 Side Effects#
PT-141's side effects are systemic, reflecting its central mechanism:
- Nausea — the most significant adverse event, reported in approximately 40% of women in RECONNECT trials and approximately 18% in male studies. Nausea is the primary driver of treatment discontinuation
- Facial flushing — transient, typically mild, occurring within minutes of injection
- Headache — reported at rates modestly above placebo
- Blood pressure — transient increases (mean 2-3 mmHg systolic) led to a contraindication in uncontrolled hypertension and cardiovascular disease
- Skin hyperpigmentation — focal darkening at injection sites in some patients, related to residual MC1R activity
- Dosing restriction — the FDA label limits use to no more than 8 doses per month and no more than 1 dose per 24 hours
Safety Profile Comparison#
The side effect profiles are almost entirely non-overlapping, reflecting the different mechanisms and routes of administration. Alprostadil's risks are predominantly local (injection site pain, priapism, fibrosis) while PT-141's risks are predominantly systemic (nausea, BP changes). Neither compound has significant drug-drug interactions with PDE5 inhibitors, though combining alprostadil with PDE5 inhibitors requires careful dosing to avoid prolonged erection.
Administration and Dosing#
Alprostadil Administration#
| Parameter | Intracavernosal (Caverject/Edex) | Intraurethral (MUSE) |
|---|---|---|
| Route | Direct injection into corpus cavernosum | Pellet inserted into urethra |
| Dose range | 1.25-60 mcg (individually titrated) | 125-1000 mcg |
| Onset | 5-20 minutes | 5-10 minutes |
| Duration | 30-60 minutes (dose-dependent) | 30-60 minutes |
| Training | Requires in-office injection training | Simpler but requires instruction |
| Frequency | No more than 3 times per week | No more than 2 times per 24 hours |
| Storage | Refrigerated (reconstituted) | Room temperature |
Dose titration is essential with alprostadil. The initial dose is typically low (2.5 mcg for neurogenic ED, 10 mcg for vasculogenic ED), with upward adjustment based on response. Over-dosing risks priapism.
PT-141 Administration#
| Parameter | Details |
|---|---|
| Route | Subcutaneous (autoinjector, abdomen or thigh) |
| Dose | Fixed 1.75 mg per injection |
| Onset | Approximately 45 minutes |
| Duration | Effects may persist for several hours |
| Frequency | No more than 1 dose per 24 hours; maximum 8 per month |
| Storage | Room temperature |
PT-141's administration is simpler than intracavernosal alprostadil — it requires a standard subcutaneous injection via a pre-filled autoinjector rather than a penile injection requiring specific anatomical knowledge.
Clinical Application Comparison#
When Alprostadil Is the Clear Choice#
- Organic ED with identified vascular or neurogenic cause — alprostadil's mechanical mechanism works regardless of etiology
- PDE5 inhibitor failure — alprostadil is the established second-line therapy
- Post-prostatectomy ED — nerve-independent mechanism is particularly valuable when cavernosal nerves have been damaged
- Diabetes-related ED — high efficacy in diabetic ED where vascular and neurological pathology coexist
- Need for reliable, predictable erection — alprostadil's direct mechanism produces erection more reliably than any centrally-acting agent
When PT-141 May Be Relevant#
- Hypoactive sexual desire disorder — PT-141's approved indication, targeting the desire deficit rather than erectile mechanics
- Psychogenic sexual dysfunction — central mechanism may address brain-level arousal and desire issues
- Patients who decline penile injection — subcutaneous autoinjection is less invasive than intracavernosal injection
- Combined desire and arousal dysfunction — PT-141 may complement (not replace) peripheral ED treatments by addressing the desire component
Can They Be Combined?#
Combining alprostadil and PT-141 is theoretically logical since they act at completely different levels — peripheral mechanics (alprostadil) and central desire (PT-141). A man with both diminished desire and erectile dysfunction could, in principle, benefit from both mechanisms. However, this combination has not been studied in clinical trials. The blood pressure effects of PT-141 combined with the hemodynamic changes from alprostadil-induced erection have not been characterized. Any such combination should be approached with caution and medical supervision.
Verdict#
Alprostadil and PT-141 answer different clinical questions. Alprostadil answers "how do we produce an erection when the normal vascular mechanism has failed?" PT-141 answers "how do we restore sexual desire when the brain's motivational circuits are underactive?" These are fundamentally different problems, and neither compound can solve the other's target indication.
For male erectile dysfunction, alprostadil remains the FDA-approved peptide option with an unmatched evidence base spanning three decades. For hypoactive sexual desire disorder, PT-141 is the only approved peptide therapy, validated through Phase 3 trials though currently approved only for women.
The existence of both compounds in the pharmacopoeia reflects the growing clinical recognition that sexual dysfunction is not a single entity but a family of distinct conditions requiring mechanistically targeted treatments. For the broader landscape of sexual health peptides, see Peptides for Sexual Health and Peptides for Men's Sexual Health.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Male erectile dysfunction unresponsive to PDE5 inhibitors
Alprostadil
Direct peripheral vasodilation produces erections independent of CNS arousal, with over 80% response rate across all ED etiologies
Hypoactive sexual desire disorder (clinical)
PT-141
Only FDA-approved treatment targeting central desire pathways through MC4R activation in the hypothalamus
Post-prostatectomy erectile dysfunction
Alprostadil
Neurogenic ED after prostatectomy responds well to direct smooth muscle relaxation via alprostadil when nerve-dependent mechanisms are impaired
Psychogenic sexual dysfunction with desire component
PT-141
Central mechanism addresses the brain-level desire deficit that characterizes psychogenic dysfunction better than peripheral vasodilators
Combined desire and erectile dysfunction
Alprostadil
Alprostadil is the only FDA-approved option for men between these two; PT-141 is approved only for female HSDD currently
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Alprostadil vs PT-141: Peripheral Vasodilator vs Central Desire Pathway
Which is better, Alprostadil or PT-141?
Alprostadil and PT-141 target fundamentally different aspects of sexual dysfunction and are not direct competitors. Alprostadil is the established choice for male erectile dysfunction, producing reliable erections through direct peripheral vasodilation regardless of the underlying cause. PT-141 addresses the central desire deficit that PDE5 inhibitors and alprostadil cannot reach, making it uniquely relevant for hypoactive sexual desire disorder. The choice depends entirely on the clinical pr... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Alprostadil and PT-141?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Clinical Evidence: advantage goes to Alprostadil; Side Effect Profile: advantage goes to neither (tie). 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Alprostadil over PT-141?
For the scenario of "Male erectile dysfunction unresponsive to PDE5 inhibitors," research data suggests Alprostadil may be more relevant. Direct peripheral vasodilation produces erections independent of CNS arousal, with over 80% response rate across all ED etiologies. This is based on currently available evidence and individual circumstances may differ.
How do Alprostadil and PT-141 differ in their mechanisms of action?
Alprostadil: Prostaglandin E1 analog that activates EP2/EP4 receptors on corpus cavernosum smooth muscle, increasing cAMP to produce direct vasodilation and erection independent of CNS arousal or desire signaling. PT-141: Melanocortin-4 receptor agonist acting in the hypothalamus to activate central sexual desire and arousal pathways through dopaminergic and oxytocinergic signaling, with no direct peripheral vascula....
Which has fewer side effects, Alprostadil or PT-141?
In terms of side effects and tolerability, the advantage goes to neither (comparable). Alprostadil: Penile pain at injection site (11-44%); priapism risk (1-3%) requiring emergency treatment; penile fibrosis with chronic use (2-12%); urethral disc.... PT-141: Nausea in approximately 40% of patients; transient facial flushing; headache; mild blood pressure elevation; focal skin hyperpigmentation; limited ....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.