Ipamorelin vs Hexarelin: Selectivity vs Potency in GH Release
Comparing ipamorelin and hexarelin as growth hormone secretagogues, covering GH potency, selectivity, cardioprotective effects, and clinical evidence.
Verdict at a Glance
Hexarelin for maximum GH potency and cardioprotective research; ipamorelin for clean, selective GH release in sustained protocols where hormonal balance matters
| Best for | Pick | Why |
|---|---|---|
| Maximum Acute GH Release | Hexarelin | Hexarelin produces the highest acute GH peak among all studied GHRPs, making it the choice when single-dose GH maximization is the goal |
| Cardiovascular Protection Research | Hexarelin | Hexarelin unique CD36 receptor binding provides GH-independent cardioprotective effects not available from any other GHS peptide |
| Long-Term GH Optimization | Ipamorelin | Ipamorelin shows less tachyphylaxis than hexarelin and produces a clean GH release without cortisol or prolactin elevation, favoring sustained protocols |
| Combined GHRH/GHRP Protocols | Ipamorelin | The minimal off-target hormonal effects of ipamorelin make it the preferred GHRP partner for synergistic protocols with GHRH analogs |
| GH-Deficient Patient Research | Hexarelin | Hexarelin has been studied in GH-deficient populations in Phase II trials, demonstrating its ability to stimulate residual pituitary function |
| Category | Hexarelin | Ipamorelin | Advantage |
|---|---|---|---|
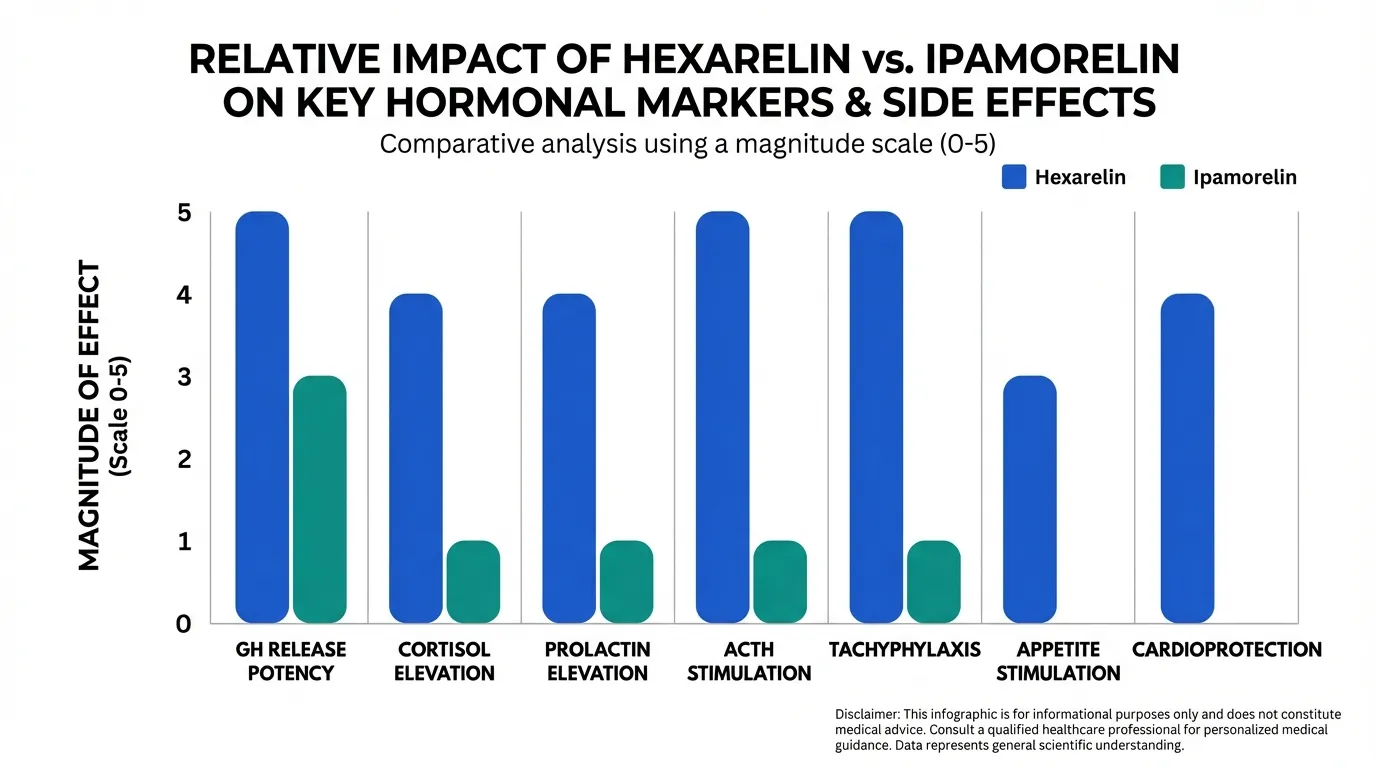
| GH Release Potency | Most potent GHS peptide studied; produces the highest acute GH release among GHRPs; subject to tachyphylaxis with repeated dosing | Moderate GH release; lower peak levels than hexarelin but consistent dose-dependent response; less prone to desensitization | Hexarelin |
| Selectivity Profile | Least selective GHRP; significant cortisol, prolactin, and ACTH elevation; broader hormonal activation beyond GH axis | Most selective GHS peptide; minimal cortisol, prolactin, or ACTH changes; isolated GH stimulation | Ipamorelin |
| Cardioprotective Effects | Unique cardioprotective properties via CD36 receptor binding; GH-independent cardiac benefits demonstrated in preclinical and clinical studies | No documented direct cardioprotective effects beyond indirect GH-mediated benefits | Hexarelin |
| Research Evidence | Extensive clinical pharmacology; Phase II cardiac studies; GH-deficient patient trials; CD36 mechanism well-characterized | Phase I/II data confirming selectivity; postoperative ileus trials; well-characterized human pharmacokinetics | Hexarelin |
| Desensitization Risk | Notable tachyphylaxis with chronic dosing; GH response diminishes significantly over weeks of continuous use | Less prone to desensitization; more consistent GH response with sustained use compared to hexarelin | Ipamorelin |

Introduction#
Hexarelin and Ipamorelin bookend the selectivity spectrum among growth hormone secretagogue peptides. Hexarelin is the most potent GHS studied, delivering the highest acute GH peak, but at the cost of significant cortisol and prolactin elevation and notable tachyphylaxis. Ipamorelin is the most selective, producing a clean GH pulse with essentially no off-target hormonal effects, making it suited for sustained protocols.
What makes this comparison particularly interesting is hexarelin's unique cardioprotective property: it binds the CD36 scavenger receptor independently of GHS-R1a, producing cardiovascular benefits unrelated to growth hormone release. This dual mechanism gives hexarelin a pharmacological dimension that no other GHS peptide shares.
Quick Comparison Table#
| Feature | Hexarelin | Ipamorelin |
|---|---|---|
| Structure | Hexapeptide (887 Da) | Pentapeptide (711.85 Da) |
| GH potency | Highest among GHRPs | Moderate |
| Cortisol effect | Significant elevation | Minimal to none |
| Prolactin effect | Moderate elevation | Minimal to none |
| Unique property | CD36-mediated cardioprotection | Exceptional GH selectivity |
| Tachyphylaxis | Significant with chronic use | Less pronounced |
| Research phase | Phase II (cardiac, GH deficiency) | Phase I/II (ileus, GH studies) |
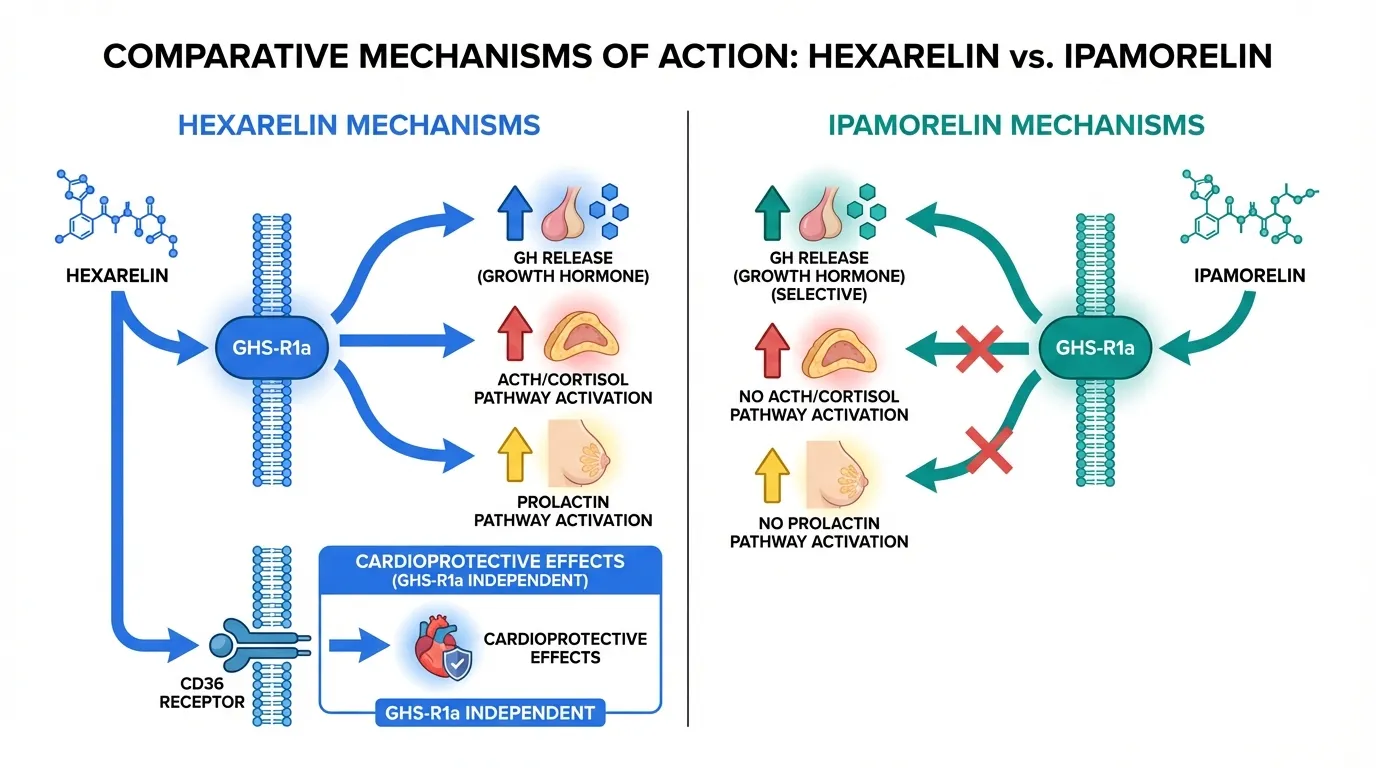
Mechanism of Action Comparison#
Hexarelin#
Hexarelin (His-D-2-methyl-Trp-Ala-Trp-D-Phe-Lys-NH2) is a synthetic hexapeptide with N-methyltryptophan substitution that confers enhanced GHS-R1a binding potency. It produces the most robust acute GH release among all studied GHRPs, though this comes with broader hormonal activation including ACTH-dependent cortisol release and prolactin elevation.
The distinguishing feature of hexarelin is its binding to CD36, a class B scavenger receptor expressed on cardiomyocytes, endothelial cells, and macrophages. This GHS-R1a-independent mechanism produces cardioprotective effects including improved cardiac contractility, reduced infarct size after ischemia, and anti-atherosclerotic activity. The CD36-mediated effects have been demonstrated even in GHS-R1a knockout models, confirming their independence from the ghrelin receptor pathway.
A significant limitation of hexarelin is tachyphylaxis: with repeated dosing over weeks, the GH response diminishes substantially, likely due to GHS-R1a downregulation and desensitization. This limits its utility in sustained GH-optimization protocols.
Ipamorelin#
Ipamorelin (Aib-His-D-2-Nal-D-Phe-Lys-NH2) achieves its selectivity through a binding mode at GHS-R1a that efficiently triggers GH release without engaging the ACTH-cortisol axis or dopamine-mediated prolactin pathways. Clinical studies have confirmed that at doses producing significant GH elevation, cortisol and prolactin levels remain statistically unchanged from baseline.
This selectivity does not extend to unique receptor targets like hexarelin's CD36 binding. Ipamorelin's therapeutic effects are mediated entirely through GHS-R1a-dependent GH release and the downstream effects of elevated GH and IGF-1.
Ipamorelin shows less tachyphylaxis than hexarelin, maintaining more consistent GH responses over repeated dosing periods, though some receptor desensitization can still occur with extended use.
Evidence and Research Comparison#
Hexarelin Research#
- Cardiac studies: Phase II trials demonstrating improved cardiac function in GH-deficient patients; preclinical data showing reduced infarct size and improved contractility
- CD36 mechanism: Well-characterized GH-independent cardioprotective pathway confirmed in knockout models
- GH deficiency: Clinical studies in GH-deficient adults showing restored GH secretion
- Pharmacology: Extensive human dose-response and pharmacokinetic characterization
- Tachyphylaxis documentation: Clinical studies documenting the time course and magnitude of GH response attenuation
Ipamorelin Research#
- Selectivity confirmation: Multiple human studies confirming GH-specific release without cortisol or prolactin changes
- Postoperative ileus: Clinical trials for accelerated bowel recovery after surgery
- Dose-response: Well-characterized dose-dependent GH release in healthy volunteers
- Combination protocols: Studies demonstrating maintained selectivity when combined with GHRH analogs
Side Effects and Safety Comparison#
Hexarelin Side Effects#
- Cortisol elevation: Clinically significant at standard GH-releasing doses; requires monitoring in sustained use
- Prolactin elevation: Moderate increases; potential concern for long-term protocols
- ACTH stimulation: Activates hypothalamic-pituitary-adrenal axis
- Appetite effects: Mild appetite stimulation through ghrelin pathway
- Tachyphylaxis: GH response diminishes over 4-8 weeks of continuous dosing
- Water retention: GH-mediated fluid retention possible
Ipamorelin Side Effects#
- Minimal hormonal effects: No clinically significant cortisol, ACTH, or prolactin changes
- Transient headache: Occasionally reported
- Injection site reactions: Mild and transient
- Water retention: GH-mediated fluid retention possible with sustained use
- No significant appetite changes: Does not activate orexigenic pathways
Dosing and Administration Comparison#
Hexarelin Dosing#
- Typical research dose: 1-2 mcg/kg, subcutaneous or IV
- Common dose: 100-200 mcg per administration
- Frequency: 2-3 times daily
- Cycling recommended: Due to tachyphylaxis, periodic breaks (e.g., 4 weeks on, 2-4 weeks off) are often discussed
Ipamorelin Dosing#
- Typical research dose: 200-300 mcg per administration, subcutaneous
- Frequency: 2-3 times daily
- Timing: Empty stomach; often before sleep or combined with GHRH analog
- Continuous use: More amenable to sustained protocols than hexarelin
Verdict#
This comparison is defined by complementary strengths rather than one peptide being universally superior:
Hexarelin excels in three scenarios: when maximum acute GH release is the primary goal, when cardiovascular protection is being researched (through its unique CD36 mechanism), and in short-term GH-deficiency diagnostic or assessment contexts. Its tachyphylaxis and hormonal side effects limit sustained use.
Ipamorelin is the better choice for sustained GH optimization protocols, combined GHRH/GHRP regimens, and any context where maintaining hormonal balance (stable cortisol, prolactin, and ACTH) is important. Its clean release profile makes it the most widely used GHS in anti-aging and body composition research.
For researchers interested in the full GHS landscape, comparing both with GHRP-2 (which sits between them in selectivity), Sermorelin (GHRH pathway), and CJC-1295 No DAC (sustained GHRH signaling) provides a comprehensive view of growth hormone stimulation options. See the Half-Life Comparison Tool for pharmacokinetic comparisons.
Detailed Category Analysis#
GH Release Potency#
Hexarelin: Most potent GHS peptide studied; produces the highest acute GH release among GHRPs; subject to tachyphylaxis with repeated dosing
Ipamorelin: Moderate GH release; lower peak levels than hexarelin but consistent dose-dependent response; less prone to desensitization
Advantage: Hexarelin
Selectivity Profile#
Hexarelin: Least selective GHRP; significant cortisol, prolactin, and ACTH elevation; broader hormonal activation beyond GH axis
Ipamorelin: Most selective GHS peptide; minimal cortisol, prolactin, or ACTH changes; isolated GH stimulation
Advantage: Ipamorelin
Cardioprotective Effects#
Hexarelin: Unique cardioprotective properties via CD36 receptor binding; GH-independent cardiac benefits demonstrated in preclinical and clinical studies
Ipamorelin: No documented direct cardioprotective effects beyond indirect GH-mediated benefits
Advantage: Hexarelin
Research Evidence#
Hexarelin: Extensive clinical pharmacology; Phase II cardiac studies; GH-deficient patient trials; CD36 mechanism well-characterized
Ipamorelin: Phase I/II data confirming selectivity; postoperative ileus trials; well-characterized human pharmacokinetics
Advantage: Hexarelin
Desensitization Risk#
Hexarelin: Notable tachyphylaxis with chronic dosing; GH response diminishes significantly over weeks of continuous use
Ipamorelin: Less prone to desensitization; more consistent GH response with sustained use compared to hexarelin
Advantage: Ipamorelin
Summary and Verdict#
Hexarelin for maximum GH potency and cardioprotective research; ipamorelin for clean, selective GH release in sustained protocols where hormonal balance matters
Best For Recommendations#
Maximum Acute GH Release#
Recommendation: Hexarelin
Reason: Hexarelin produces the highest acute GH peak among all studied GHRPs, making it the choice when single-dose GH maximization is the goal
Cardiovascular Protection Research#
Recommendation: Hexarelin
Reason: Hexarelin unique CD36 receptor binding provides GH-independent cardioprotective effects not available from any other GHS peptide
Long-Term GH Optimization#
Recommendation: Ipamorelin
Reason: Ipamorelin shows less tachyphylaxis than hexarelin and produces a clean GH release without cortisol or prolactin elevation, favoring sustained protocols
Combined GHRH/GHRP Protocols#
Recommendation: Ipamorelin
Reason: The minimal off-target hormonal effects of ipamorelin make it the preferred GHRP partner for synergistic protocols with GHRH analogs
GH-Deficient Patient Research#
Recommendation: Hexarelin
Reason: Hexarelin has been studied in GH-deficient populations in Phase II trials, demonstrating its ability to stimulate residual pituitary function
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Maximum Acute GH Release
Hexarelin
Hexarelin produces the highest acute GH peak among all studied GHRPs, making it the choice when single-dose GH maximization is the goal
Cardiovascular Protection Research
Hexarelin
Hexarelin unique CD36 receptor binding provides GH-independent cardioprotective effects not available from any other GHS peptide
Long-Term GH Optimization
Ipamorelin
Ipamorelin shows less tachyphylaxis than hexarelin and produces a clean GH release without cortisol or prolactin elevation, favoring sustained protocols
Combined GHRH/GHRP Protocols
Ipamorelin
The minimal off-target hormonal effects of ipamorelin make it the preferred GHRP partner for synergistic protocols with GHRH analogs
GH-Deficient Patient Research
Hexarelin
Hexarelin has been studied in GH-deficient populations in Phase II trials, demonstrating its ability to stimulate residual pituitary function
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Ipamorelin vs Hexarelin: Selectivity vs Potency in GH Release
What are the key differences between Hexarelin and Ipamorelin?
The main differences across comparison categories are: GH Release Potency: advantage goes to Hexarelin; Selectivity Profile: advantage goes to Ipamorelin; Cardioprotective Effects: advantage goes to Hexarelin. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Hexarelin over Ipamorelin?
For the scenario of "Maximum Acute GH Release," research data suggests Hexarelin may be more relevant. Hexarelin produces the highest acute GH peak among all studied GHRPs, making it the choice when single-dose GH maximization is the goal. This is based on currently available evidence and individual circumstances may differ.
In what scenario might Hexarelin be preferred?
For "Cardiovascular Protection Research," Hexarelin may be more appropriate. Hexarelin unique CD36 receptor binding provides GH-independent cardioprotective effects not available from any other GHS peptide. Individual factors and clinical context should guide any decisions.
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.