GHRP-2 vs Hexarelin: Comprehensive Comparison
A detailed comparison of GHRP-2 and Hexarelin covering mechanisms of action, GH secretion potency, dosing protocols, side effects, desensitization profiles, and research evidence for these two prominent growth hormone secretagogues.
Verdict at a Glance
GHRP-2 for sustained GH augmentation research due to lower desensitization and regulatory precedent; Hexarelin for acute maximal GH release studies and cardiovascular research via its unique CD36 mechanism
| Best for | Pick | Why |
|---|---|---|
| Sustained GH Augmentation | GHRP-2 | GHRP-2 maintains GH-releasing efficacy over longer administration periods with significantly less tachyphylaxis than Hexarelin |
| Maximum Acute GH Release | Hexarelin | Hexarelin is the most potent GHS studied in humans, producing the largest single-dose GH response among all synthetic GHRPs |
| GH Deficiency Diagnostic Testing | GHRP-2 | GHRP-2 is approved in Japan specifically as a diagnostic agent for GH deficiency, providing regulatory validation and established testing protocols |
| Cardiovascular Research | Hexarelin | Hexarelin uniquely binds CD36 receptors, conferring GH-independent cardioprotective effects including reduced infarct size and improved cardiac function in preclinical models |
| Combination Protocols with GHRH Analogs | GHRP-2 | GHRP-2's lower desensitization profile makes it better suited for sustained combination protocols with CJC-1295 or other GHRH analogs |
| Anti-Aging and Body Composition Research | GHRP-2 | GHRP-2 offers more consistent long-term GH elevation with less appetite stimulation, making it more practical for body composition studies |
| Category | GHRP-2 | Hexarelin | Advantage |
|---|---|---|---|
| Mechanism of Action | Synthetic hexapeptide GHS that activates GHS-R1a to stimulate pituitary GH release; also suppresses somatostatin and modulates hypothalamic GHRH neurons with minimal ghrelin-like appetite effects | Synthetic hexapeptide GHS with potent GHS-R1a activation for GH release; uniquely binds CD36 scavenger receptors conferring cardioprotective effects independent of GH secretion | Hexarelin |
| Research Evidence | Extensive clinical data including Phase 2 trials; approved in Japan as a diagnostic agent for GH deficiency; well-characterized pharmacokinetics | Phase 2 clinical trials completed; most potent GHS studied in humans; significant cardiovascular research including post-MI and heart failure models | Comparable |
| Side Effect Profile | Mild cortisol and prolactin elevations at higher doses; minimal appetite stimulation compared to other GHRPs; generally well-tolerated | Cortisol and prolactin elevations similar to other GHRPs; pronounced tachyphylaxis (desensitization) with chronic use limiting long-term efficacy | GHRP-2 |
| Desensitization Risk | Lower desensitization risk with sustained GH response over weeks of administration; maintains efficacy with repeated dosing | Significant tachyphylaxis observed within 4-16 weeks of continuous use; GH response diminishes substantially with chronic administration | GHRP-2 |
| GH Release Potency | Potent GH secretagogue producing robust GH pulses; dose-dependent response plateauing around 200-300 mcg | Most potent GHS studied in humans; produces the largest GH release among all synthetic GHRPs at equivalent doses | Hexarelin |
| Regulatory Status | Approved in Japan as a diagnostic tool for GH deficiency (GHRP Kaken 100); Phase 2 clinical trials completed internationally | Phase 2 clinical trials completed for GH deficiency and cardiovascular applications; not approved for therapeutic use in any jurisdiction | GHRP-2 |

Introduction#
GHRP-2 and Hexarelin are both synthetic hexapeptide growth hormone secretagogues (GHS) that stimulate the release of growth hormone from the anterior pituitary gland by activating the growth hormone secretagogue receptor (GHS-R1a). Developed during the 1980s and 1990s as part of the broader effort to create orally active GH-releasing compounds, these peptides share a common receptor target but differ meaningfully in potency, desensitization profiles, and secondary pharmacological properties.
GHRP-2 (D-Ala-D-2-Nal-Ala-Trp-D-Phe-Lys-NH2, MW 817.9 Da) has achieved regulatory approval in Japan as a diagnostic agent for growth hormone deficiency, making it one of the few synthetic GHRPs with clinical validation. Hexarelin (His-D-2-methyl-Trp-Ala-Trp-D-Phe-Lys-NH2, MW 887 Da) is recognized as the most potent growth hormone secretagogue studied in humans but is limited by pronounced desensitization with chronic use. Hexarelin also uniquely engages CD36 scavenger receptors, providing cardioprotective effects that are entirely independent of its GH-releasing activity.
This comparison examines the key pharmacological and practical differences between these two closely related GHRPs to aid researchers in understanding which compound may be more appropriate for specific investigational contexts.
Mechanism of Action Comparison#
GHRP-2#
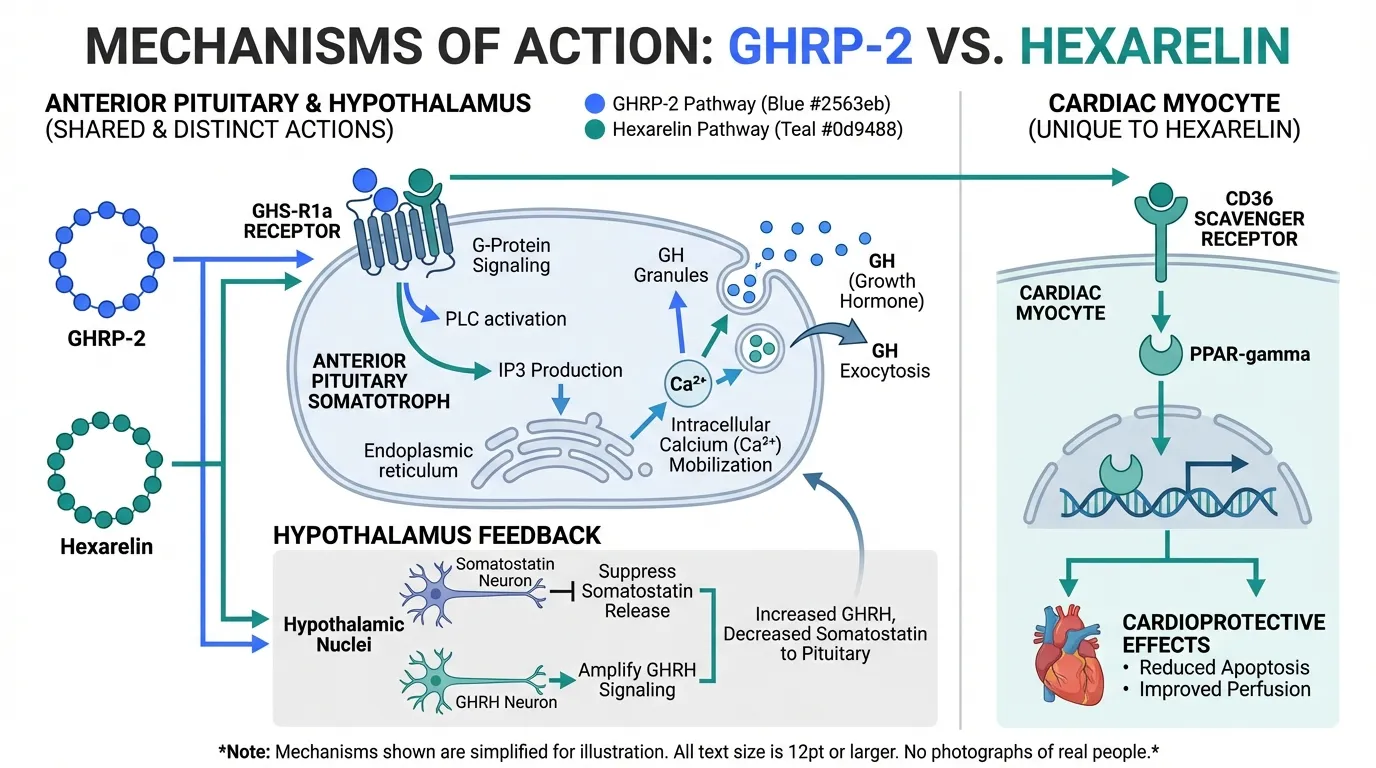
GHRP-2 stimulates growth hormone release through a dual mechanism. As a GHS-R1a agonist, it directly activates the ghrelin receptor on somatotroph cells in the anterior pituitary, triggering intracellular calcium mobilization and subsequent GH exocytosis. Simultaneously, GHRP-2 acts at the hypothalamic level to suppress somatostatin (the primary GH inhibitor) and amplify endogenous GHRH signaling, creating a synergistic effect on pulsatile GH release.
Notably, GHRP-2 produces substantially less appetite stimulation than GHRP-6 or ghrelin itself, despite activating the same receptor. This selectivity is attributed to its distinct binding orientation within the GHS-R1a binding pocket, which favors GH secretion signaling cascades over appetite-related pathways. GHRP-2 also causes modest, dose-dependent elevations in cortisol, ACTH, and prolactin, though these effects are generally transient and clinically insignificant at standard research doses. Its ability to amplify GHRH-induced GH release makes it particularly effective in combination protocols, where GHRP-2 and GHRH analogs together produce GH responses greater than the sum of either agent alone.
Hexarelin#
Hexarelin shares the core GHS-R1a mechanism with GHRP-2, activating pituitary somatotrophs to release stored GH through calcium-dependent exocytosis. At the hypothalamic level, Hexarelin similarly suppresses somatostatin tone and enhances GHRH neuronal activity. However, Hexarelin consistently produces the largest GH release of any synthetic GHS studied in human clinical trials, with peak GH levels exceeding those achieved by GHRP-2, GHRP-6, or ipamorelin at comparable doses.
What distinguishes Hexarelin pharmacologically is its binding to CD36 (cluster of differentiation 36), a class B scavenger receptor expressed on cardiac myocytes, macrophages, and endothelial cells. This interaction activates PPAR-gamma signaling and downstream cardioprotective pathways, including reduced myocardial apoptosis, improved coronary perfusion, and attenuation of ischemia-reperfusion injury. These effects occur independently of GH secretion, as demonstrated by studies in GH-deficient and hypophysectomized animal models where cardiac benefits persisted. This dual-receptor pharmacology positions Hexarelin uniquely among GHRPs as both a GH secretagogue and a cardiovascular protective agent.
Dosing Comparison#
GHRP-2 Dosing#
GHRP-2 has been studied across multiple dosing paradigms in both clinical and preclinical settings:
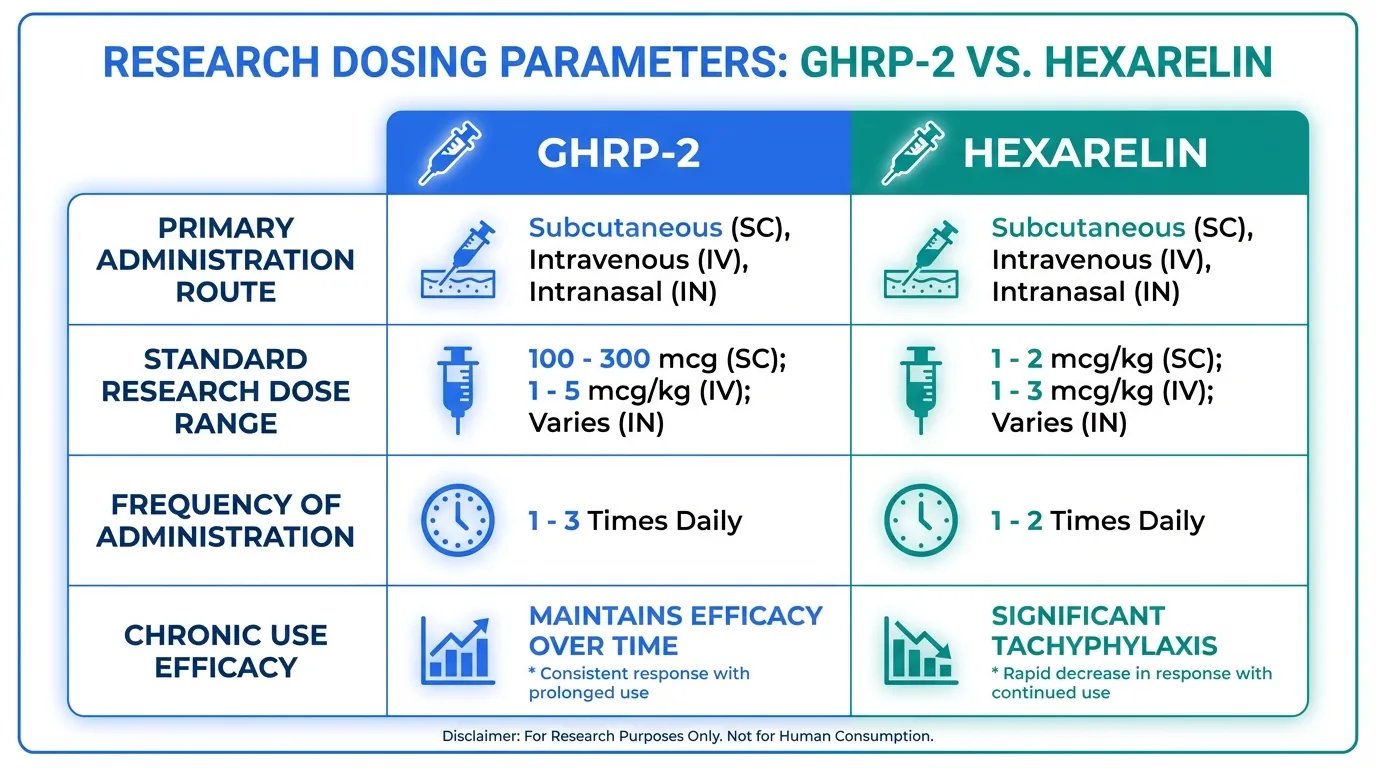
- Subcutaneous injection: Research doses typically range from 100-300 mcg per administration, with 200 mcg being the most commonly studied dose in clinical trials
- Intravenous bolus: Used in diagnostic protocols for GH deficiency at 1 mcg/kg body weight (the approved Japanese protocol)
- Intranasal: Investigated at doses of 10-30 mcg/kg, though bioavailability is reduced compared to injection
- Frequency: Typically administered 1-3 times daily in research protocols, timed around fasting periods to maximize GH response
The GH response to GHRP-2 is dose-dependent up to approximately 200-300 mcg per injection, above which a plateau effect is observed. Peak GH levels typically occur 15-30 minutes post-injection, with the GH pulse resolving within 2-3 hours. GHRP-2 maintains its GH-releasing efficacy with repeated dosing over weeks to months, which is a significant practical advantage.
Hexarelin Dosing#
Hexarelin dosing protocols in research settings include:
- Subcutaneous injection: Standard research doses of 1-2 mcg/kg body weight, typically 100-200 mcg per injection
- Intravenous administration: Used in clinical studies at 1-2 mcg/kg for acute GH response assessment
- Intranasal: Studied at higher doses (up to 400 mcg) due to reduced mucosal absorption
- Frequency: Typically 1-2 times daily, though chronic dosing is limited by tachyphylaxis
Peak GH response to Hexarelin occurs within 15-30 minutes of subcutaneous administration. Critically, studies have demonstrated that the GH-releasing effect of Hexarelin diminishes significantly with continuous administration. Research by Rahim et al. showed that GH response was reduced by approximately 50% after 4 weeks of daily Hexarelin and further diminished by 16 weeks. This tachyphylaxis necessitates cycling strategies with drug-free intervals to restore receptor sensitivity.
Side Effects Comparison#
GHRP-2 Side Effects#
GHRP-2 has demonstrated a generally favorable safety profile across clinical studies. Commonly reported effects include:
- Mild, transient increases in cortisol and ACTH levels, typically returning to baseline within 1-2 hours
- Modest prolactin elevation at higher doses (>300 mcg), though less pronounced than with GHRP-6
- Minimal appetite stimulation, a notable advantage over GHRP-6 and native ghrelin
- Transient water retention consistent with increased GH/IGF-1 activity
- Injection site reactions including redness and mild discomfort
- Potential for tingling or numbness in extremities (paraesthesia)
- Possible drowsiness following administration
Importantly, GHRP-2 does not appear to significantly alter glucose homeostasis at standard research doses, though chronic GH elevation carries theoretical concerns regarding insulin sensitivity that warrant monitoring.
Hexarelin Side Effects#
Hexarelin's side effect profile is similar in nature but differs in certain respects:
- Cortisol and prolactin elevations comparable to other GHRPs and somewhat more pronounced than GHRP-2
- The most significant concern is tachyphylaxis, where receptor desensitization leads to progressive loss of GH-releasing efficacy with chronic use
- Appetite stimulation that is more noticeable than GHRP-2, though less than GHRP-6
- Transient flushing and warmth at the time of injection
- Headache reported in some clinical trial participants
- Potential fluid retention with sustained use
The desensitization issue with Hexarelin is not merely a side effect but a fundamental limitation of its chronic utility. Unlike GHRP-2, which maintains relatively stable GH responses over extended periods, Hexarelin's diminishing returns require structured cycling protocols, adding complexity to long-term research designs.
Research Evidence Comparison#
GHRP-2 Research#
GHRP-2 has a robust clinical evidence base, highlighted by its regulatory approval as a diagnostic agent:
- GH deficiency diagnosis: The GHRP-2 stimulation test (Kaken Pharmaceutical) received approval in Japan for diagnosing adult and pediatric GH deficiency, with established sensitivity and specificity parameters. Studies by Doi et al. validated its diagnostic accuracy compared to insulin tolerance testing
- Endocrine studies: Phase 2 clinical trials evaluating GHRP-2 for GH deficiency treatment demonstrated sustained GH elevation, increased IGF-1 levels, and improvements in body composition markers including lean mass and fat distribution
- Combination research: Studies by Bowers et al. demonstrated that GHRP-2 combined with GHRH produces synergistic GH release approximately 2-3 times greater than either peptide alone, establishing the scientific basis for combination protocols
- Aging research: Clinical studies in elderly subjects showed that GHRP-2 restored GH pulse amplitude toward youthful levels, suggesting utility in age-related GH decline
The breadth of clinical data, combined with regulatory approval, provides GHRP-2 with a stronger translational evidence base than most other GHRPs.
Hexarelin Research#
Hexarelin's research portfolio spans both endocrine and cardiovascular domains:
- GH secretion potency: Multiple clinical studies confirmed Hexarelin as the most potent synthetic GHS, with studies by Ghigo et al. demonstrating GH peaks of 50-80 mcg/L in healthy subjects, exceeding responses to all other GHRPs
- Cardiovascular research: Landmark studies by Broglio et al. and Locatelli et al. demonstrated cardioprotective effects in animal models of myocardial infarction, including 50% reduction in infarct size and improved left ventricular function. These effects were mediated through CD36 receptor activation independent of GH
- Heart failure: Preliminary clinical studies in patients with heart failure showed improved cardiac output and reduced systemic vascular resistance following acute Hexarelin administration
- Desensitization studies: Rahim et al. and others systematically characterized the tachyphylaxis phenomenon, providing critical information about the limitations of chronic Hexarelin use
- Pediatric GH deficiency: Clinical trials in GH-deficient children demonstrated significant GH release, though desensitization limited enthusiasm for chronic therapeutic application
Hexarelin's unique cardiovascular pharmacology via CD36 represents a distinct research niche that no other GHS currently occupies.
Key Differences Summary#
- Potency: Hexarelin produces the largest acute GH release of any synthetic GHS; GHRP-2 is potent but produces somewhat lower peak GH levels
- Desensitization: GHRP-2 maintains GH-releasing efficacy with chronic use; Hexarelin shows significant tachyphylaxis within 4-16 weeks
- Appetite effects: GHRP-2 causes minimal appetite stimulation; Hexarelin produces moderate appetite increase
- Cardiovascular activity: Hexarelin uniquely binds CD36 receptors for GH-independent cardioprotection; GHRP-2 lacks this secondary mechanism
- Regulatory status: GHRP-2 is approved in Japan as a GH deficiency diagnostic; Hexarelin has no regulatory approvals
- Molecular weight: GHRP-2 is 817.9 Da; Hexarelin is 887 Da
- Clinical phase: Both have completed Phase 2 clinical trials
- Prolactin/cortisol effects: Both elevate these hormones, with Hexarelin producing slightly more pronounced increases
- Combination suitability: GHRP-2 is better suited for long-term combination protocols with GHRH analogs due to sustained receptor sensitivity
Conclusion#
GHRP-2 and Hexarelin represent two closely related but pharmacologically distinct growth hormone secretagogues. For research requiring sustained GH augmentation over extended periods, GHRP-2 offers clear advantages through its resistance to desensitization, minimal appetite effects, and regulatory validation in Japan. Its well-characterized pharmacokinetic profile and synergy with GHRH analogs make it the more practical choice for long-term investigational protocols.
Hexarelin, while limited by tachyphylaxis for chronic GH augmentation, holds unique value in cardiovascular research through its CD36-mediated cardioprotective effects. Its unmatched potency for acute GH release also makes it valuable for single-dose pharmacological studies and diagnostic applications where maximal GH stimulation is desired. The choice between these peptides ultimately depends on the research objective: sustained physiological GH enhancement favors GHRP-2, while maximal acute GH release or cardiovascular investigation favors Hexarelin.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Sustained GH Augmentation
GHRP-2
GHRP-2 maintains GH-releasing efficacy over longer administration periods with significantly less tachyphylaxis than Hexarelin
Maximum Acute GH Release
Hexarelin
Hexarelin is the most potent GHS studied in humans, producing the largest single-dose GH response among all synthetic GHRPs
GH Deficiency Diagnostic Testing
GHRP-2
GHRP-2 is approved in Japan specifically as a diagnostic agent for GH deficiency, providing regulatory validation and established testing protocols
Cardiovascular Research
Hexarelin
Hexarelin uniquely binds CD36 receptors, conferring GH-independent cardioprotective effects including reduced infarct size and improved cardiac function in preclinical models
Combination Protocols with GHRH Analogs
GHRP-2
GHRP-2's lower desensitization profile makes it better suited for sustained combination protocols with CJC-1295 or other GHRH analogs
Anti-Aging and Body Composition Research
GHRP-2
GHRP-2 offers more consistent long-term GH elevation with less appetite stimulation, making it more practical for body composition studies
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About GHRP-2 vs Hexarelin: Comprehensive Comparison
What are the key differences between GHRP-2 and Hexarelin?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Hexarelin; Research Evidence: advantage goes to neither (tie); Side Effect Profile: advantage goes to GHRP-2. 3 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider GHRP-2 over Hexarelin?
For the scenario of "Sustained GH Augmentation," research data suggests GHRP-2 may be more relevant. GHRP-2 maintains GH-releasing efficacy over longer administration periods with significantly less tachyphylaxis than Hexarelin. This is based on currently available evidence and individual circumstances may differ.
How do GHRP-2 and Hexarelin differ in their mechanisms of action?
GHRP-2: Synthetic hexapeptide GHS that activates GHS-R1a to stimulate pituitary GH release; also suppresses somatostatin and modulates hypothalamic GHRH neurons with minimal ghrelin-like appetite effects. Hexarelin: Synthetic hexapeptide GHS with potent GHS-R1a activation for GH release; uniquely binds CD36 scavenger receptors conferring cardioprotective effects independent of GH secretion.
Which has fewer side effects, GHRP-2 or Hexarelin?
In terms of side effects and tolerability, the advantage goes to GHRP-2. GHRP-2: Mild cortisol and prolactin elevations at higher doses; minimal appetite stimulation compared to other GHRPs; generally well-tolerated. Hexarelin: Cortisol and prolactin elevations similar to other GHRPs; pronounced tachyphylaxis (desensitization) with chronic use limiting long-term efficacy.
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.