GHRP-2 vs Tesamorelin: Comprehensive Comparison
A detailed comparison of GHRP-2 and Tesamorelin, two growth hormone secretagogues that stimulate GH release through different receptor pathways -- ghrelin/GHS-R1a versus GHRH receptor -- with distinct regulatory statuses and clinical applications.
Verdict at a Glance
Tesamorelin is the established choice with FDA approval, physiological GH release, and proven efficacy in visceral fat reduction; GHRP-2 offers potent acute GH stimulation through a complementary pathway and may be most valuable in combination with GHRH analogs for synergistic GH release
| Best for | Pick | Why |
|---|---|---|
| FDA-Approved Clinical Use | Tesamorelin | Tesamorelin (Egrifta) is the only FDA-approved GHRH analog, specifically indicated for reduction of excess abdominal fat in HIV-infected patients with lipodystrophy |
| Maximizing Acute GH Pulse | GHRP-2 | GHRP-2 produces rapid and robust GH peaks within 15-30 minutes through ghrelin receptor activation, generating stronger acute GH pulses than GHRH analogs alone |
| Visceral Fat Reduction | Tesamorelin | Phase 3 trial data demonstrated statistically significant reduction in trunk fat and visceral adipose tissue, with FDA approval for this specific indication |
| Synergistic GH Protocols | GHRP-2 | GHRP-2 acting through GHS-R1a and Tesamorelin through GHRH receptor produce synergistic GH release when combined, making GHRP-2 the ideal complement to a GHRH-based protocol |
| GH Deficiency Diagnostic Testing | GHRP-2 | GHRP-2 stimulation tests have been studied as diagnostic tools for GH deficiency, producing reliable and reproducible GH peaks useful for clinical assessment |
| Category | GHRP-2 | Tesamorelin | Advantage |
|---|---|---|---|
| Mechanism of Action | Synthetic hexapeptide that binds ghrelin receptor (GHS-R1a), stimulating GH release from the anterior pituitary through a pathway independent of GHRH; also increases ghrelin, cortisol, and prolactin | Synthetic 44-amino acid analog of human GHRH that binds the GHRH receptor on pituitary somatotrophs, directly stimulating GH synthesis and pulsatile release through the physiological GHRH pathway | Tesamorelin |
| Research Evidence | Phase 2 clinical studies; extensive preclinical data on GH release kinetics; studied for GH deficiency diagnostics and body composition effects | FDA-approved (Egrifta) based on Phase 3 trials; demonstrated reduction of visceral adipose tissue in HIV lipodystrophy; post-market safety surveillance data available | Tesamorelin |
| Side Effect Profile | Increases cortisol and prolactin alongside GH; stimulates appetite through ghrelin pathway; potential for desensitization with chronic use | FDA-approved safety profile; injection site reactions most common; does not significantly affect cortisol or prolactin; contraindicated in active malignancy | Tesamorelin |
| Dosing Complexity | Typically administered 2-3 times daily via subcutaneous injection to exploit pulsatile GH release; timing relative to meals and sleep is important | Once-daily subcutaneous injection (2 mg); straightforward dosing with FDA-approved protocol; available as prefilled delivery system | Tesamorelin |
| GH Release Profile | Produces rapid, robust GH pulse within 15-30 minutes; strong acute GH release but may desensitize GHS-R1a with chronic dosing; amplifies GHRH-induced GH release synergistically | Stimulates physiological pulsatile GH release through GHRH receptor; maintains feedback sensitivity; more sustained and physiological GH secretion pattern | Tesamorelin |
| Synergistic Potential | Acts on GHS-R1a pathway, which is synergistic with GHRH pathway; combining with GHRH analogs produces supra-additive GH release | Acts on GHRH pathway, which is synergistic with GHS-R1a pathway; combining with GHRP amplifies total GH output significantly | Comparable |

Introduction#
GHRP-2 and Tesamorelin are both growth hormone secretagogues -- compounds that stimulate the pituitary gland to release endogenous growth hormone -- but they achieve this through fundamentally different receptor pathways. GHRP-2 (Growth Hormone Releasing Peptide-2) is a synthetic hexapeptide that acts on the ghrelin receptor (GHS-R1a), mimicking the endogenous hormone ghrelin to trigger GH release. Tesamorelin is a 44-amino acid synthetic analog of growth hormone-releasing hormone (GHRH) that binds the GHRH receptor on pituitary somatotrophs, directly stimulating GH synthesis and secretion through the physiological GHRH pathway.
This mechanistic distinction is not merely academic. The ghrelin and GHRH pathways converge on the same pituitary somatotroph cells but through different intracellular signaling cascades, producing different GH release kinetics, hormonal side effect profiles, and -- critically -- synergistic effects when combined. Understanding these differences is essential for researchers and clinicians evaluating growth hormone secretagogue strategies, particularly given that Tesamorelin has achieved FDA approval while GHRP-2 remains an investigational compound.
Mechanism of Action Comparison#
GHRP-2#
GHRP-2 (pralmorelin, KP-102) is a synthetic hexapeptide with the sequence D-Ala-D-2Nal-Ala-Trp-D-Phe-Lys-NH2 and a molecular weight of 817.9 Da. It functions as a potent agonist of the growth hormone secretagogue receptor type 1a (GHS-R1a), the same receptor activated by the endogenous hormone ghrelin.
The GHS-R1a signaling pathway operates through several interconnected mechanisms:
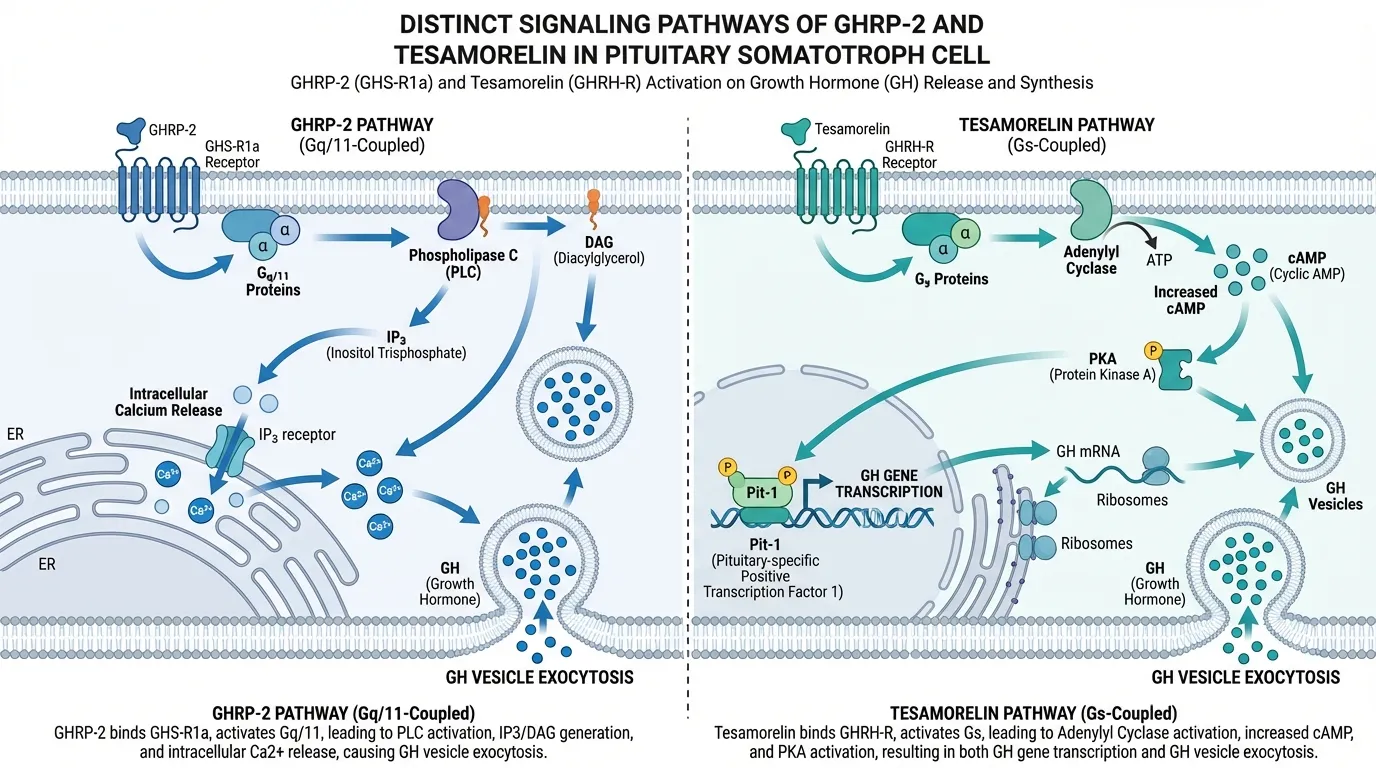
- Phospholipase C activation: GHS-R1a couples to Gq/11 proteins, activating phospholipase C, which generates inositol trisphosphate (IP3) and diacylglycerol (DAG). IP3 triggers calcium release from intracellular stores, while DAG activates protein kinase C
- Calcium influx: The intracellular calcium rise, combined with membrane depolarization and L-type calcium channel activation, triggers GH vesicle exocytosis from somatotrophs
- Somatostatin antagonism: GHRP-2 partially antagonizes somatostatin's inhibitory effects on GH release, making GH secretion less suppressed during somatostatin-dominant periods
- Hypothalamic effects: GHRP-2 also acts at the hypothalamic level, stimulating GHRH neurons and suppressing somatostatin release, creating a feedforward loop that amplifies pituitary GH output
Beyond GH release, GHRP-2's ghrelin receptor activation produces additional endocrine effects:
- Cortisol increase: GHRP-2 stimulates ACTH and cortisol release, though typically within physiological ranges
- Prolactin elevation: Modest increases in prolactin are observed, especially at higher doses
- Appetite stimulation: Through central ghrelin pathway activation, GHRP-2 can increase hunger, though this effect is less pronounced than with exogenous ghrelin
Tesamorelin#
Tesamorelin (trade name Egrifta) is a synthetic analog of human GHRH consisting of the full 44-amino acid GHRH sequence with a trans-3-hexenoic acid modification at the N-terminus. This modification enhances metabolic stability without altering receptor binding. Its molecular weight is 5135.9 Da, making it significantly larger than GHRP-2.
Tesamorelin's mechanism follows the physiological GHRH signaling cascade:
- GHRH receptor binding: Tesamorelin binds the GHRH receptor (GHRH-R), a G-protein-coupled receptor expressed primarily on anterior pituitary somatotrophs
- cAMP-PKA pathway: GHRH-R couples to Gs proteins, activating adenylyl cyclase and increasing intracellular cyclic AMP (cAMP). cAMP activates protein kinase A (PKA), which phosphorylates downstream targets
- GH gene transcription: PKA activates the transcription factor Pit-1, which drives GH gene transcription, promoting both acute GH release and long-term GH synthesis
- Pulsatile release: Tesamorelin triggers GH release that follows the physiological pulsatile pattern, preserving the normal ultradian rhythm of GH secretion
Key mechanistic advantages of the GHRH pathway:
- Feedback preservation: Tesamorelin-stimulated GH release remains subject to normal negative feedback through IGF-1 and somatostatin, reducing the risk of supraphysiological GH levels
- Hormonal specificity: Unlike GHRP-2, Tesamorelin does not significantly affect cortisol, prolactin, or appetite at therapeutic doses
- Somatotroph trophic effects: GHRH signaling promotes somatotroph cell health and proliferation, potentially supporting long-term pituitary GH reserve
Dosing Comparison#
GHRP-2 Dosing#
GHRP-2 dosing is based on clinical research studies and Phase 2 trial protocols:
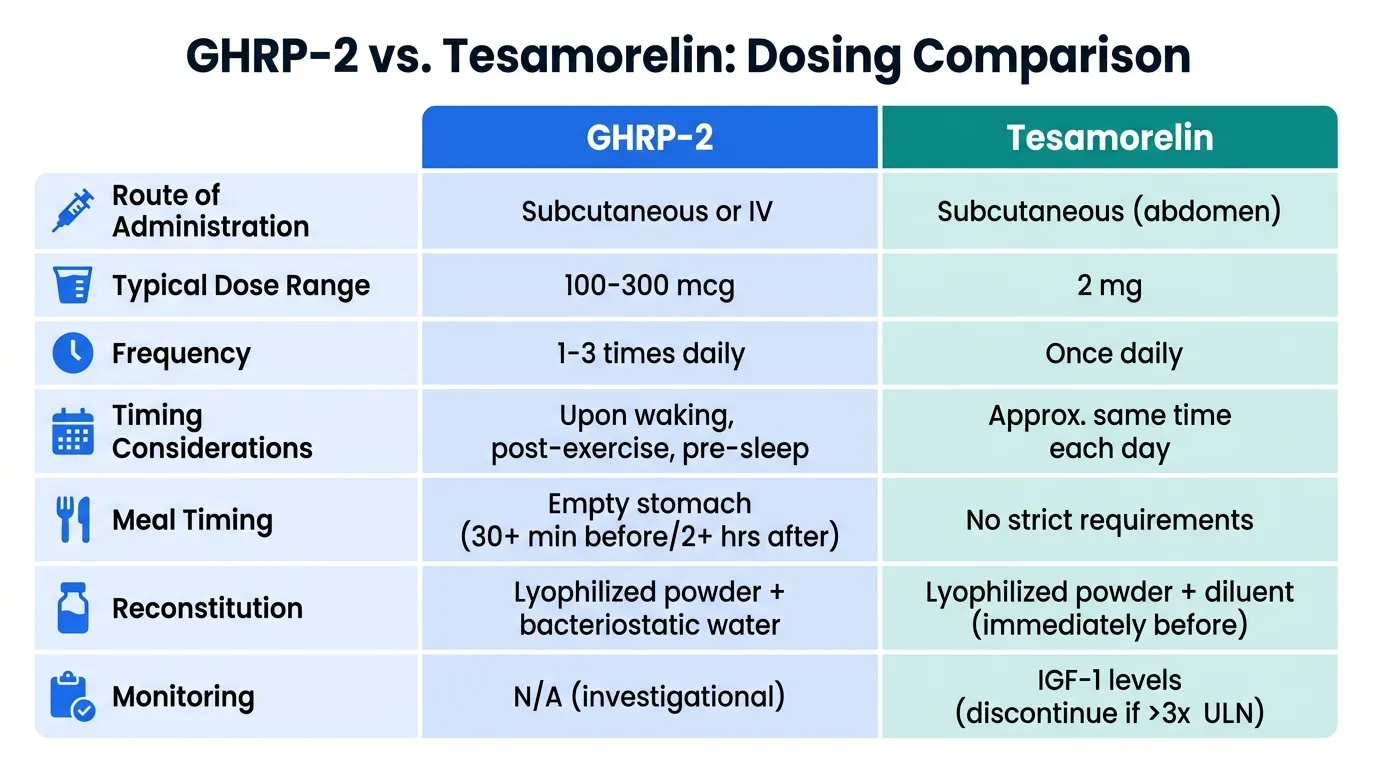
- Route: Subcutaneous or intravenous injection
- Typical research dose: 100-300 mcg per injection
- Frequency: 1-3 times daily; multiple daily doses exploit the pulsatile nature of GH release
- Timing considerations: Often administered upon waking, post-exercise, and before sleep to align with natural GH secretory periods. Should be administered on an empty stomach (30+ minutes before or 2+ hours after meals) to avoid blunting by blood glucose and insulin
- Diagnostic use: Single bolus of 100 mcg IV or 1 mcg/kg IV for GH stimulation testing
- Reconstitution: Lyophilized powder reconstituted with bacteriostatic water
The multiple-daily-dosing requirement and meal-timing restrictions make GHRP-2 protocols more complex than once-daily Tesamorelin administration.
Tesamorelin Dosing#
FDA-approved dosing for Tesamorelin (Egrifta):
- Route: Subcutaneous injection into the abdomen
- Dose: 2 mg once daily
- Timing: Administered at approximately the same time each day; no strict meal-timing requirements
- Duration: Clinical trials evaluated 26-52 weeks of continuous treatment; effect on visceral fat reduction maintained during treatment but may reverse upon discontinuation
- Reconstitution: Supplied as lyophilized powder with diluent; reconstituted immediately before injection
- Monitoring: IGF-1 levels should be monitored; treatment should be discontinued if IGF-1 exceeds 3 times the upper limit of normal
The simplicity of once-daily dosing without meal restrictions gives Tesamorelin a practical advantage for patient compliance.
Side Effects Comparison#
GHRP-2 Side Effects#
GHRP-2's side effect profile reflects its broad receptor activity:
- Cortisol elevation: ACTH and cortisol increase with each GHRP-2 dose; chronic use may lead to sustained cortisol elevations, though typically within the upper physiological range. This is a meaningful concern for individuals with existing HPA axis dysfunction
- Prolactin increase: Dose-dependent prolactin elevation occurs; clinical significance is generally low at standard doses but may be relevant with chronic high-dose use
- Appetite stimulation: Central ghrelin pathway activation increases hunger, which may be counterproductive for body composition goals but beneficial in cachexia or anorexia contexts
- Water retention: Some reports of fluid retention and peripheral edema, likely related to GH and IGF-1 increases
- Desensitization: Chronic continuous GHRP-2 administration may lead to GHS-R1a downregulation, potentially diminishing GH release over time. Pulsatile dosing strategies may mitigate this
- Injection site reactions: Mild pain, redness at injection sites
- Numbness and tingling: Paresthesias reported in some studies, likely related to GH effects on fluid balance
Tesamorelin Side Effects#
FDA-approved safety profile based on Phase 3 trials and post-market surveillance:
- Injection site reactions: Most common adverse event (up to 8.4%); includes erythema, pruritus, pain, and irritation at injection site
- Peripheral edema: Reported in approximately 6% of patients; related to GH-mediated fluid retention
- Arthralgia: Joint pain reported in 3-5% of patients, a known GH-associated effect
- Myalgia: Muscle pain in approximately 3% of patients
- Paresthesias: Numbness or tingling in extremities in approximately 5%
- Carpal tunnel syndrome: Reported rarely; a recognized complication of elevated GH/IGF-1
- Hyperglycemia: Modest increases in fasting glucose observed; monitoring recommended in diabetic patients
- Contraindications: Active malignancy (GH and IGF-1 may promote tumor growth), disrupted hypothalamic-pituitary axis, pregnancy, known hypersensitivity
Notably absent from Tesamorelin's profile are the cortisol and prolactin elevations seen with GHRP-2, representing a cleaner hormonal side effect profile.
Research Evidence Comparison#
GHRP-2 Research#
GHRP-2 has a substantial body of research, primarily at the preclinical and Phase 2 level:
- GH release characterization: Extensive pharmacological studies establishing GHRP-2 as one of the most potent synthetic GH secretagogues. Single doses produce GH peaks of 30-90 ng/mL within 15-30 minutes, significantly exceeding natural GH pulses
- Diagnostic applications: Studied as a GH stimulation test for diagnosing GH deficiency in children and adults. The GHRP-2 test shows comparable sensitivity and specificity to insulin tolerance testing with a superior safety profile
- Body composition: Phase 2 studies examining effects on body composition, showing trends toward increased lean mass and decreased fat mass with repeated dosing
- Synergy with GHRH: Key studies demonstrating that combined GHRP-2 + GHRH administration produces GH release 2-3 times greater than either agent alone, establishing the mechanistic basis for combination protocols
- Aging studies: Research showing that GH responses to GHRP-2 are preserved in elderly subjects to a greater degree than responses to GHRH alone, suggesting maintained GHS-R1a sensitivity with aging
- Cardiac effects: Preclinical evidence of cardioprotective properties through GHS-R1a activation, independent of GH release
The primary limitation is that GHRP-2 has not progressed beyond Phase 2 development for any therapeutic indication. Its broad endocrine effects (cortisol, prolactin, appetite) have been viewed as disadvantages relative to more selective GH secretagogues.
Tesamorelin Research#
Tesamorelin has the most extensive clinical evidence base of any GHRH analog:
- Phase 3 trials (HIV lipodystrophy): Two pivotal randomized, double-blind, placebo-controlled trials demonstrated that Tesamorelin 2 mg daily significantly reduced trunk fat (-15.2% vs -0.2% placebo) and visceral adipose tissue (VAT) at 26 weeks. Trunk fat reduction was maintained through 52 weeks of continuous treatment
- Body composition: Tesamorelin increased IGF-1 levels to the normal range, reduced waist circumference, and improved body image without increasing subcutaneous fat or total body weight
- Lipid effects: Favorable effects on triglycerides observed in some studies; no significant adverse effects on glucose homeostasis in non-diabetic patients
- Cognitive function: Exploratory studies in healthy older adults and MCI (mild cognitive impairment) patients suggesting improved executive function and verbal memory with Tesamorelin treatment, potentially through IGF-1-mediated neuroprotective effects
- MASH in HIV: Studies examining Tesamorelin's effects on hepatic fat and liver disease in HIV-positive patients, showing reduced liver fat without worsening of fibrosis markers
- FDA approval: Egrifta approved November 2010; Egrifta SV (single-vial formulation) approved 2019, improving preparation convenience
Key Differences Summary#
- Receptor target: GHRP-2 acts on GHS-R1a (ghrelin receptor); Tesamorelin acts on GHRH-R (GHRH receptor)
- Peptide size: GHRP-2 is a hexapeptide (817.9 Da, 6 amino acids); Tesamorelin is a large peptide (5135.9 Da, 44 amino acids)
- GH release pattern: GHRP-2 produces rapid, sharp GH pulses; Tesamorelin promotes more physiological pulsatile release
- Hormonal selectivity: GHRP-2 increases cortisol, prolactin, and appetite alongside GH; Tesamorelin is more GH-specific
- Regulatory status: GHRP-2 is Phase 2/investigational; Tesamorelin is FDA-approved (Egrifta) for HIV lipodystrophy
- Dosing frequency: GHRP-2 is typically dosed 1-3 times daily; Tesamorelin is once daily
- Feedback sensitivity: Tesamorelin-stimulated GH remains feedback-regulated; GHRP-2 partially overrides somatostatin inhibition
- Synergy: GHRP-2 and Tesamorelin act through complementary pathways, producing synergistic GH release when combined
- Appetite effects: GHRP-2 stimulates appetite (ghrelin pathway); Tesamorelin is appetite-neutral
Conclusion#
GHRP-2 and Tesamorelin stimulate growth hormone release through mechanistically distinct and synergistic pathways, making them complementary rather than interchangeable. Tesamorelin is the clear frontrunner for clinical applications: its FDA approval, physiological GH release pattern, clean hormonal side effect profile, and proven efficacy in reducing visceral adipose tissue make it the established standard among GHRH-based therapies. For clinicians seeking an approved GH secretagogue, Tesamorelin is the only option with regulatory validation.
GHRP-2 offers distinct advantages in specific contexts. Its rapid, potent GH pulses through the ghrelin/GHS-R1a pathway make it valuable for GH stimulation testing and diagnostic applications. More importantly, the synergistic relationship between GHS-R1a and GHRH-R pathways means that GHRP-2 combined with a GHRH analog like Tesamorelin produces GH release substantially greater than either agent alone. This synergy forms the mechanistic basis for combination protocols studied in growth hormone deficiency research.
However, GHRP-2's broader endocrine effects -- including cortisol and prolactin elevation, appetite stimulation, and potential receptor desensitization -- represent practical limitations compared to Tesamorelin's more targeted action. Researchers should weigh these trade-offs based on their specific goals: Tesamorelin for sustained, physiological GH optimization with established safety data; GHRP-2 for potent acute GH stimulation, diagnostic testing, or as a synergistic complement to GHRH-based protocols.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
FDA-Approved Clinical Use
Tesamorelin
Tesamorelin (Egrifta) is the only FDA-approved GHRH analog, specifically indicated for reduction of excess abdominal fat in HIV-infected patients with lipodystrophy
Maximizing Acute GH Pulse
GHRP-2
GHRP-2 produces rapid and robust GH peaks within 15-30 minutes through ghrelin receptor activation, generating stronger acute GH pulses than GHRH analogs alone
Visceral Fat Reduction
Tesamorelin
Phase 3 trial data demonstrated statistically significant reduction in trunk fat and visceral adipose tissue, with FDA approval for this specific indication
Synergistic GH Protocols
GHRP-2
GHRP-2 acting through GHS-R1a and Tesamorelin through GHRH receptor produce synergistic GH release when combined, making GHRP-2 the ideal complement to a GHRH-based protocol
GH Deficiency Diagnostic Testing
GHRP-2
GHRP-2 stimulation tests have been studied as diagnostic tools for GH deficiency, producing reliable and reproducible GH peaks useful for clinical assessment
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About GHRP-2 vs Tesamorelin: Comprehensive Comparison
What are the key differences between GHRP-2 and Tesamorelin?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Tesamorelin; Research Evidence: advantage goes to Tesamorelin; Side Effect Profile: advantage goes to Tesamorelin. 3 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Tesamorelin over GHRP-2?
For the scenario of "FDA-Approved Clinical Use," research data suggests Tesamorelin may be more relevant. Tesamorelin (Egrifta) is the only FDA-approved GHRH analog, specifically indicated for reduction of excess abdominal fat in HIV-infected patients with lipodystrophy. This is based on currently available evidence and individual circumstances may differ.
How do GHRP-2 and Tesamorelin differ in their mechanisms of action?
GHRP-2: Synthetic hexapeptide that binds ghrelin receptor (GHS-R1a), stimulating GH release from the anterior pituitary through a pathway independent of GHRH; also increases ghrelin, cortisol, and prolactin. Tesamorelin: Synthetic 44-amino acid analog of human GHRH that binds the GHRH receptor on pituitary somatotrophs, directly stimulating GH synthesis and pulsatile release through the physiological GHRH pathway.
Which has fewer side effects, GHRP-2 or Tesamorelin?
In terms of side effects and tolerability, the advantage goes to Tesamorelin. GHRP-2: Increases cortisol and prolactin alongside GH; stimulates appetite through ghrelin pathway; potential for desensitization with chronic use. Tesamorelin: FDA-approved safety profile; injection site reactions most common; does not significantly affect cortisol or prolactin; contraindicated in active m....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.