DSIP vs Oveporexton: Sleep Peptides Compared
Evidence-based comparison of DSIP (delta sleep-inducing peptide) and oveporexton (TAK-861), two fundamentally different approaches to sleep disorders -- a research peptide promoting delta sleep versus a Phase 3 orexin receptor agonist for narcolepsy.
Verdict at a Glance
Oveporexton (TAK-861) is the clear winner on scientific evidence, having demonstrated statistically significant efficacy across multiple Phase 3 trials for narcolepsy type 1, with a well-characterized mechanism targeting the orexin receptor 2. DSIP remains a research peptide with limited and outdated clinical evidence. However, these peptides address fundamentally different conditions -- oveporexton targets narcolepsy-related wakefulness deficits while DSIP aims to promote deeper sleep in insomnia. They are not direct substitutes. For narcolepsy, oveporexton represents a potential breakthrough. For general sleep optimization, DSIP remains investigational with insufficient evidence to recommend clinical use.
| Best for | Pick | Why |
|---|---|---|
| Narcolepsy Type 1 | Oveporexton | Phase 3 trials (FirstLight and RadiantLight) demonstrated statistically significant improvement across all narcolepsy symptoms with p<0.001. Addresses the underlying orexin deficiency that causes NT1. |
| Evidence-Based Treatment | Oveporexton | Phase 2b data published in NEJM, two positive Phase 3 trials, FDA Breakthrough Therapy designation. DSIP has no modern clinical trial data. |
| Oral Convenience | Oveporexton | Oveporexton is an oral tablet taken twice daily. DSIP requires subcutaneous injection, reconstitution, and evening timing. |
| Current Availability | DSIP | DSIP is available now from research peptide suppliers, while oveporexton is not yet commercially available pending FDA approval. However, DSIP lacks FDA approval and standardized quality control. |
| Sleep Quality Enhancement (Non-Narcolepsy) | Neither (insufficient evidence) | DSIP has limited and outdated evidence for insomnia. Oveporexton is designed specifically for narcolepsy, not general insomnia. Neither has strong evidence for general sleep quality improvement. |
| Category | DSIP | Oveporexton | Advantage |
|---|---|---|---|
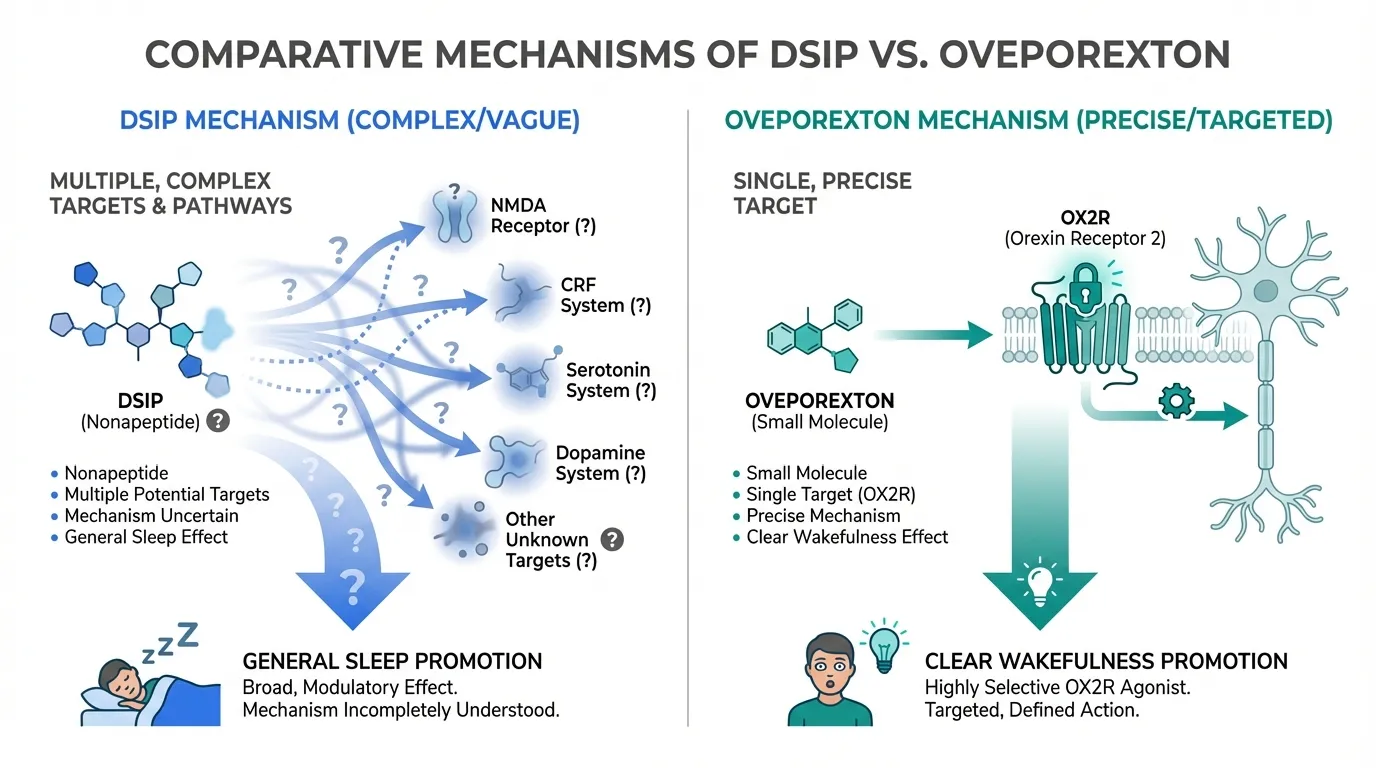
| Mechanism of Action | DSIP is a nonapeptide (Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu) synthesized in the hypothalamus that modulates sleep architecture by promoting slow-wave (delta) sleep. It acts through multiple pathways including NMDA receptor modulation, corticotropin-releasing factor suppression, and serotonin/dopamine signaling rather than through a single defined receptor. | Oveporexton (TAK-861) is a small molecule orexin receptor 2 (OX2R) selective agonist that restores orexin signaling to address the underlying orexin neuron loss in narcolepsy type 1. It directly activates the wake-promoting orexin pathway with a well-defined single-target mechanism. | Oveporexton |
| Research Evidence | DSIP has limited clinical evidence. A 1992 double-blind study in chronic insomniacs showed modest sleep improvements. Most research is from the 1970s-1990s with small sample sizes and inconsistent methodology. No large-scale RCTs or modern regulatory-quality trials exist. | Oveporexton has robust Phase 3 evidence. Two pivotal Phase 3 trials (FirstLight and RadiantLight) met all primary and secondary endpoints with p<0.001 across doses in narcolepsy type 1. Phase 2b data published in the New England Journal of Medicine. Breakthrough Therapy designation from the FDA. | Oveporexton |
| Side Effect Profile | DSIP safety data is limited. Reported side effects from small studies include occasional headache and morning grogginess. No systematic safety evaluation exists. Long-term effects are unknown due to lack of controlled trials. | Oveporexton was generally well-tolerated in Phase 3 trials with no serious treatment-related adverse events. Most common side effects were insomnia (paradoxical at higher doses), urinary urgency, and urinary frequency. Safety profile consistent across multiple studies. | Oveporexton |
| Dosing and Administration | DSIP is administered by subcutaneous or intravenous injection, typically 100-500 mcg in the evening before sleep. No standardized dosing protocol exists. Available only as a research peptide requiring reconstitution. | Oveporexton is an oral tablet taken twice daily (1 mg or 2 mg). Convenient oral administration with established dosing from Phase 3 trials. Expected to be available by prescription upon FDA approval. | Oveporexton |
| Accessibility | DSIP is available from research peptide suppliers and some compounding pharmacies. Not FDA-approved for any indication. No prescription required from research sources, but quality varies significantly between suppliers. | Oveporexton is not yet commercially available. Currently in late-stage clinical development with NDA submission planned for 2025. Upon approval, will require a prescription and will likely be expensive as a branded pharmaceutical. | DSIP |

Introduction#
DSIP (delta sleep-inducing peptide) and oveporexton (TAK-861) represent two fundamentally different approaches to sleep-related disorders, separated by decades of scientific progress. DSIP was discovered in 1977 as a nonapeptide found in the cerebral venous blood of rabbits during electrically induced sleep, while oveporexton is a 21st-century small molecule agonist targeting the orexin receptor 2 with precision pharmacology.
These compounds address different aspects of sleep pathology. DSIP aims to promote slow-wave (delta) sleep and normalize sleep architecture, while oveporexton restores wakefulness by replacing the missing orexin signaling in narcolepsy type 1. They are not direct alternatives for the same condition, but their comparison illustrates how sleep pharmacology has evolved from poorly characterized neuropeptides to targeted receptor agonists.
Mechanism of Action Comparison#
DSIP#
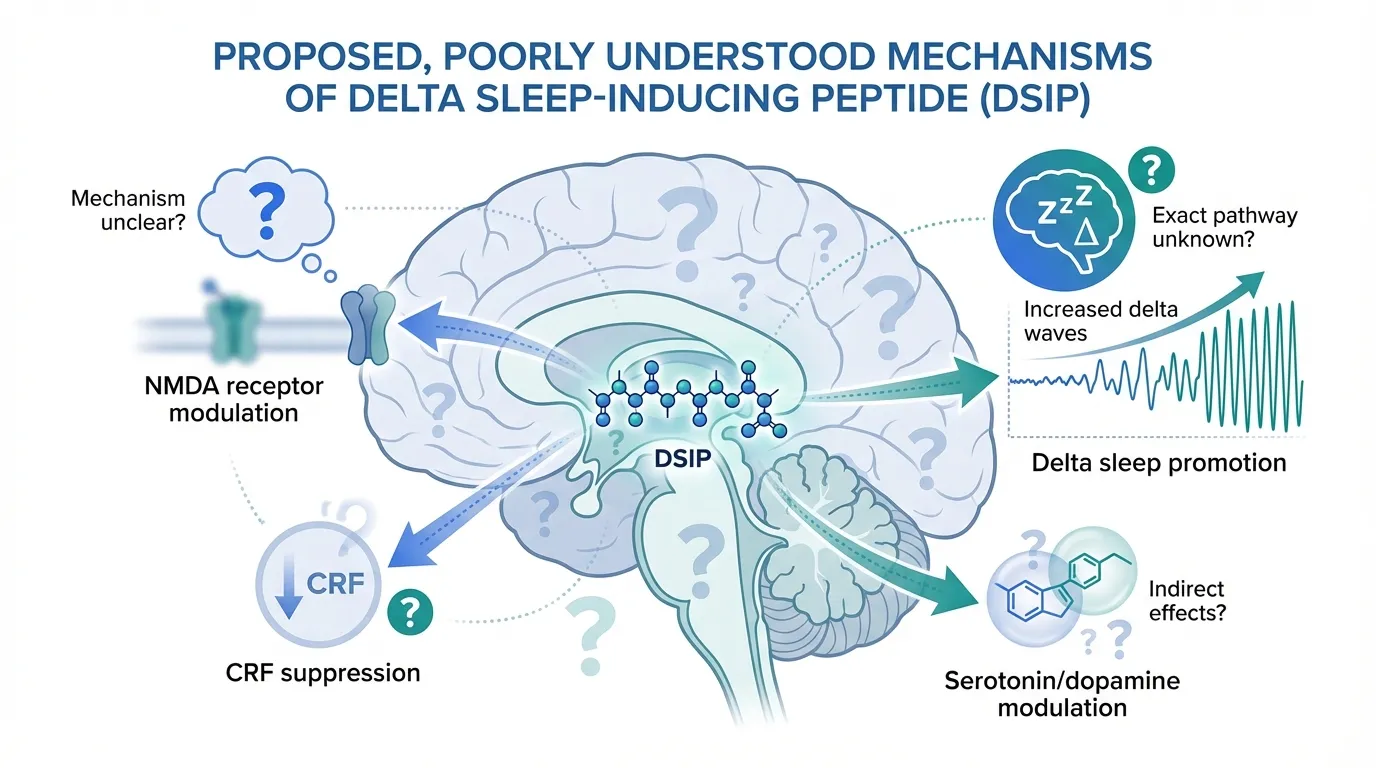
DSIP (Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu) is a naturally occurring nonapeptide synthesized in the hypothalamus. Its mechanism remains incompletely understood despite decades of research. Rather than acting through a single defined receptor, DSIP appears to modulate multiple neural pathways:
- NMDA receptor modulation: May influence glutamatergic signaling involved in sleep-wake transitions
- CRF suppression: Reduces corticotropin-releasing factor, potentially lowering stress-related arousal
- Serotonin/dopamine modulation: Affects monoaminergic systems involved in sleep regulation
- Delta sleep promotion: Increases the proportion of slow-wave (delta) sleep, the most restorative sleep stage
DSIP does not act as a sedative. Instead, it appears to normalize disrupted sleep patterns by modulating the brain's endogenous sleep-promoting mechanisms.
Oveporexton#
Oveporexton (TAK-861) is a potent, orally available, selective agonist of the orexin receptor 2 (OX2R). Its mechanism is precise and well-characterized:
- OX2R activation: Directly stimulates the wake-promoting orexin pathway
- Orexin replacement: Compensates for the loss of orexin-producing neurons that causes narcolepsy type 1
- Selective agonism: Preferentially activates OX2R over OX1R, targeting wakefulness without broad hypothalamic stimulation
- Twice-daily dosing: Maintains orexin signaling throughout waking hours
Mechanistic Comparison#
| Feature | DSIP | Oveporexton |
|---|---|---|
| Molecule type | Nonapeptide (9 amino acids) | Small molecule |
| Molecular weight | ~848 Da | Small molecule (undisclosed) |
| Primary target | Multiple (poorly defined) | OX2R (well-defined) |
| Direction of effect | Promotes sleep (delta waves) | Promotes wakefulness |
| Receptor selectivity | Non-selective | OX2R-selective |
| Mechanism clarity | Poorly characterized | Fully characterized |
| Natural occurrence | Endogenous neuropeptide | Synthetic agonist |
Dosing Comparison#
DSIP Dosing#
No standardized dosing protocol exists for DSIP. Reported dosing from research and clinical use:
| Parameter | Details |
|---|---|
| Route | Subcutaneous or intravenous injection |
| Typical dose | 100-500 mcg |
| Timing | Evening, 30-60 minutes before sleep |
| Frequency | Daily or as needed |
| Reconstitution | Required (lyophilized powder) |
| Half-life | Approximately 7-8 minutes (rapid degradation) |
The very short half-life of DSIP raises questions about its pharmacological utility, as the peptide is rapidly degraded after injection. Some researchers have explored modified analogs with improved stability.
Oveporexton Dosing#
| Parameter | Details |
|---|---|
| Route | Oral tablet |
| Doses tested | 1 mg and 2 mg twice daily |
| Timing | Morning and midday (promotes daytime wakefulness) |
| Frequency | Twice daily |
| Reconstitution | None (oral tablet) |
| Onset | Phase 3 data showed significant effects at 12 weeks |
Side Effects Comparison#
DSIP Side Effects#
Limited safety data exists for DSIP:
- Occasional headache reported in small studies
- Morning grogginess at higher doses
- No systematic adverse event reporting
- No long-term safety data available
- No anti-drug antibody or immunogenicity testing
Oveporexton Side Effects#
From Phase 2 and Phase 3 clinical trials:
| Adverse Event | Frequency | Severity |
|---|---|---|
| Insomnia | Common | Mild (paradoxical, dose-related) |
| Urinary urgency | Common | Mild |
| Urinary frequency | Common | Mild |
| Serious treatment-related AEs | None reported | N/A |
Oveporexton was generally well-tolerated with a safety profile consistent across the Phase 2b, FirstLight, and RadiantLight studies.
Research Evidence Comparison#
DSIP Research#
DSIP research peaked in the 1980s-1990s and has largely stalled:
- Schneider-Helmert (1987): Reported acute sleep-inducing effects of IV DSIP in normal subjects, with sleep increased 59% within a 130-minute observation window
- Schneider-Helmert & Schoenenberger (1992): Double-blind study in chronic insomniacs showed DSIP improved sleep efficiency, but sample size was small
- 2024 fusion peptide study: Frontiers in Pharmacology published research on DSIP-BBB fusion peptides in insomnia mouse models, representing renewed interest in the peptide
- No Phase 2 or Phase 3 data: DSIP has never undergone modern regulatory-quality clinical trials
Evidence level: Low -- small studies from the 1980s-1990s, no modern RCTs.
Oveporexton Research#
Oveporexton has a robust and rapidly growing evidence base:
- Phase 2b (NEJM 2025): Published in the New England Journal of Medicine, demonstrating dose-dependent improvements in narcolepsy type 1 symptoms
- FirstLight Phase 3: Met all primary and secondary endpoints (p<0.001) in narcolepsy type 1
- RadiantLight Phase 3: Met all primary and secondary endpoints (p<0.001) across all dose groups at 12 weeks
- Preclinical (Scientific Reports 2024): Demonstrated OX2R selectivity and wakefulness promotion in monkeys and mice
- FDA Breakthrough Therapy: Designation for excessive daytime sleepiness in NT1
Evidence level: High -- multiple Phase 3 RCTs with statistically significant results.
Key Differences Summary#
- Opposite effects: DSIP promotes sleep; oveporexton promotes wakefulness. They target opposite ends of the sleep-wake spectrum.
- Evidence gap: Oveporexton has Phase 3 data in NEJM; DSIP has no modern clinical trials.
- Mechanism clarity: Oveporexton has a defined single-target mechanism (OX2R); DSIP acts through multiple poorly characterized pathways.
- Administration: Oveporexton is an oral tablet; DSIP requires injection with a very short half-life.
- Regulatory status: Oveporexton has Breakthrough Therapy designation and NDA submission planned; DSIP has no regulatory pathway.
- Target condition: Oveporexton specifically treats narcolepsy type 1; DSIP is explored for insomnia and sleep quality generally.
- Availability: DSIP is available now from research suppliers; oveporexton is not yet commercially available.
Conclusion#
DSIP and oveporexton are not direct competitors but rather illustrate the evolution of sleep pharmacology from empirical neuropeptide research to targeted molecular therapy. Oveporexton represents a potential first-in-class treatment for narcolepsy type 1, with rigorous Phase 3 evidence, a well-defined mechanism, and a clear regulatory path. DSIP remains an interesting but poorly validated research peptide with limited clinical evidence.
For patients with narcolepsy type 1, oveporexton offers a scientifically validated approach that addresses the underlying disease mechanism. For individuals seeking general sleep improvement, neither compound has robust evidence -- oveporexton is not designed for insomnia, and DSIP lacks the clinical data to support its use. The comparison highlights the importance of mechanism-based drug development and the limitations of poorly characterized peptide therapies.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Narcolepsy Type 1
Oveporexton
Phase 3 trials (FirstLight and RadiantLight) demonstrated statistically significant improvement across all narcolepsy symptoms with p<0.001. Addresses the underlying orexin deficiency that causes NT1.
Evidence-Based Treatment
Oveporexton
Phase 2b data published in NEJM, two positive Phase 3 trials, FDA Breakthrough Therapy designation. DSIP has no modern clinical trial data.
Oral Convenience
Oveporexton
Oveporexton is an oral tablet taken twice daily. DSIP requires subcutaneous injection, reconstitution, and evening timing.
Current Availability
DSIP
DSIP is available now from research peptide suppliers, while oveporexton is not yet commercially available pending FDA approval. However, DSIP lacks FDA approval and standardized quality control.
Sleep Quality Enhancement (Non-Narcolepsy)
Neither (insufficient evidence)
DSIP has limited and outdated evidence for insomnia. Oveporexton is designed specifically for narcolepsy, not general insomnia. Neither has strong evidence for general sleep quality improvement.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About DSIP vs Oveporexton: Sleep Peptides Compared
Which is better, DSIP or Oveporexton?
Oveporexton (TAK-861) is the clear winner on scientific evidence, having demonstrated statistically significant efficacy across multiple Phase 3 trials for narcolepsy type 1, with a well-characterized mechanism targeting the orexin receptor 2. DSIP remains a research peptide with limited and outdated clinical evidence. However, these peptides address fundamentally different conditions -- oveporexton targets narcolepsy-related wakefulness deficits while DSIP aims to promote deeper sleep in ins... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between DSIP and Oveporexton?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Oveporexton; Research Evidence: advantage goes to Oveporexton; Side Effect Profile: advantage goes to Oveporexton. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Oveporexton over DSIP?
For the scenario of "Narcolepsy Type 1," research data suggests Oveporexton may be more relevant. Phase 3 trials (FirstLight and RadiantLight) demonstrated statistically significant improvement across all narcolepsy symptoms with p<0.001. Addresses the underlying orexin deficiency that causes NT1.. This is based on currently available evidence and individual circumstances may differ.
How do DSIP and Oveporexton differ in their mechanisms of action?
DSIP: DSIP is a nonapeptide (Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu) synthesized in the hypothalamus that modulates sleep architecture by promoting slow-wave (delta) sleep. It acts through multiple pathways.... Oveporexton: Oveporexton (TAK-861) is a small molecule orexin receptor 2 (OX2R) selective agonist that restores orexin signaling to address the underlying orexin neuron loss in narcolepsy type 1. It directly ac....
Which has fewer side effects, DSIP or Oveporexton?
In terms of side effects and tolerability, the advantage goes to Oveporexton. DSIP: DSIP safety data is limited. Reported side effects from small studies include occasional headache and morning grogginess. No systematic safety eval.... Oveporexton: Oveporexton was generally well-tolerated in Phase 3 trials with no serious treatment-related adverse events. Most common side effects were insomnia....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.