KPV vs Larazotide: Two Approaches to Gut Barrier Health
Comparing KPV and Larazotide for gut health: anti-inflammatory NF-kB inhibition versus tight junction regulation with different evidence levels and mechanisms.
Verdict at a Glance
KPV and Larazotide target gut barrier health through fundamentally different mechanisms: KPV suppresses the inflammatory signaling (NF-kB) that damages the gut barrier, while Larazotide directly stabilizes tight junctions by blocking zonulin-mediated permeability. Larazotide has a vastly stronger evidence base, with Phase 3 clinical data for celiac disease, FDA Fast Track designation, and safety data from 800+ patients. KPV remains entirely preclinical with no human clinical trials. For conditions driven by increased permeability (celiac disease, gluten sensitivity), Larazotide has direct clinical evidence. For conditions driven by mucosal inflammation (IBD), KPV's NF-kB mechanism is more directly relevant but unproven in humans. Their mechanisms are complementary rather than competing -- one addresses the inflammatory trigger while the other reinforces the structural barrier.
| Best for | Pick | Why |
|---|---|---|
| Celiac Disease Research | Larazotide | Larazotide was specifically developed for celiac disease, has Phase 3 clinical trial data demonstrating reduced symptom days, and holds FDA Fast Track designation. KPV has no celiac-specific data. |
| Inflammatory Bowel Disease Research | KPV | KPV's NF-kB inhibition directly targets the inflammatory pathology of IBD, with preclinical efficacy in both Crohn's and UC models. Larazotide's tight junction mechanism is less directly relevant to established IBD inflammation. |
| General Gut Barrier Support | Larazotide | Larazotide directly stabilizes tight junctions, the structural basis of gut barrier integrity, and has human clinical data. KPV supports barrier function indirectly through inflammation reduction but lacks human evidence. |
| Current Accessibility for Research | KPV | KPV is available through research peptide suppliers and has demonstrated oral bioavailability. Larazotide is not commercially available outside clinical trials or specialized research procurement. |
| Category | KPV | Larazotide | Advantage |
|---|---|---|---|
| Mechanism of Action | Alpha-MSH-derived tripeptide (Lys-Pro-Val) that inhibits NF-kB activation in a dose-dependent manner, suppressing pro-inflammatory cytokines (TNF-alpha, IL-1beta, IL-6, IL-8). Enters cells via PepT1 transporter in intestinal epithelial and immune cells. Targets the inflammatory component of gut barrier dysfunction. | Synthetic octapeptide (AT-1001) that acts as a zonulin receptor antagonist, preventing zonulin-mediated opening of intestinal tight junctions. Directly targets paracellular permeability by stabilizing claudin and occludin proteins at tight junction complexes. Works locally in the gut lumen without systemic absorption. | Comparable |
| Research Evidence | Entirely preclinical evidence base. Demonstrated efficacy in murine DSS and TNBS colitis models with reduced inflammation and improved histology. In vitro NF-kB inhibition confirmed in multiple cell types. No human clinical trials conducted for any indication. Limited number of published studies overall. | Advanced clinical development through Phase 3 for celiac disease. Phase 2b trial (n=342) showed reduced intestinal permeability and GI symptoms versus placebo. Phase 3 trial demonstrated statistically significant improvement in symptom days. Received FDA Fast Track designation for celiac disease. Multiple peer-reviewed publications from independent groups. | Larazotide |
| Side Effect Profile | No human safety data exists. Animal studies report no significant adverse effects at studied doses. As a naturally derived tripeptide fragment of alpha-MSH, theoretical safety profile is favorable. However, absence of human data means the actual side effect profile is unknown. No formal toxicology studies published. | Well-characterized safety profile from multiple clinical trials. Side effects comparable to placebo in Phase 2 and Phase 3 studies. Most common adverse events were headache, upper respiratory tract infection, and nausea at rates similar to placebo. Minimal systemic absorption limits off-target effects. Over 800 patients exposed in clinical trials. | Larazotide |
| Gut Health Applications | Studied primarily for inflammatory bowel disease (IBD) models. Preclinical data in both Crohn's-like (TNBS) and ulcerative colitis-like (DSS) models. Mechanism (NF-kB inhibition) is broadly relevant to any inflammatory gut condition. PepT1-mediated oral uptake allows targeted intestinal delivery. No clinical data for any specific gut condition. | Developed specifically for celiac disease with Phase 3 clinical data. Mechanism (tight junction stabilization) is directly relevant to conditions involving increased intestinal permeability ("leaky gut"). Being investigated for other permeability-related conditions. Does not address inflammation directly but prevents the permeability increase that triggers downstream inflammation. | Larazotide |
| Accessibility and Practical Use | Available through research peptide suppliers without prescription. Not FDA-approved or regulated as a drug. Small tripeptide with demonstrated oral bioavailability via PepT1 transporter, which is unusual for peptides. No standardized dosing established. Low manufacturing complexity due to small size (3 amino acids). | Not yet commercially available as an approved drug (pending regulatory approval). Available only through clinical trial enrollment or research supply. FDA Fast Track designation may accelerate approval timeline for celiac disease. Would require prescription if approved. Oral capsule formulation designed for clinical use. | KPV |

Introduction#
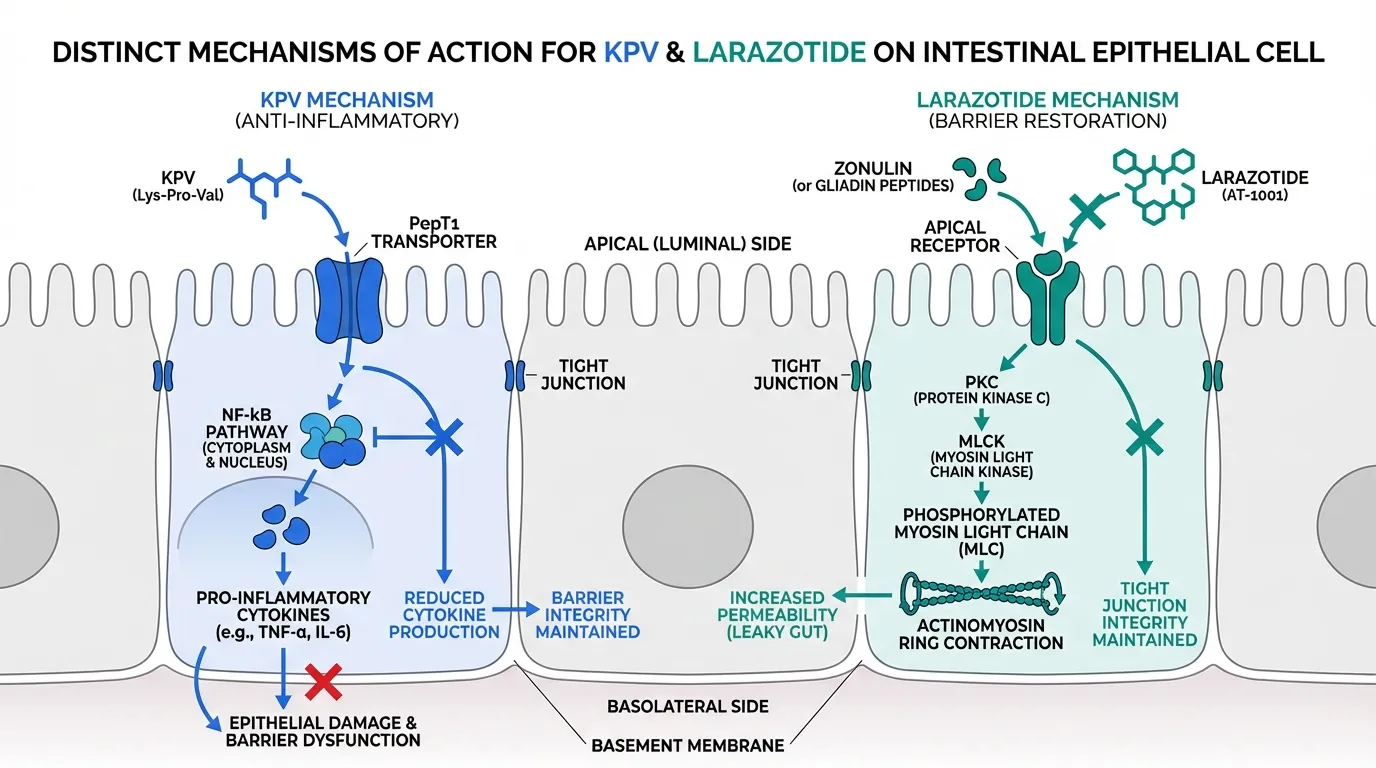
KPV and Larazotide represent two fundamentally different strategies for addressing gut barrier dysfunction. KPV, a tripeptide derived from alpha-melanocyte-stimulating hormone, attacks the problem from the inflammatory side -- suppressing the NF-kB-driven cytokine cascade that damages intestinal epithelium. Larazotide (AT-1001), a synthetic octapeptide, takes the structural approach -- directly blocking zonulin-mediated opening of tight junctions to maintain paracellular barrier integrity.
This distinction matters because gut barrier dysfunction is not a single condition but a spectrum. In celiac disease, gluten triggers zonulin release, which opens tight junctions and allows gluten peptides to access the lamina propria, initiating an autoimmune response. In inflammatory bowel disease, chronic inflammation directly damages epithelial cells and disrupts barrier function from the intracellular side. The optimal therapeutic strategy depends on whether the primary driver is permeability (favoring Larazotide) or inflammation (favoring KPV).
This comparison examines the evidence, mechanisms, and practical considerations for each peptide to help researchers evaluate which is more relevant to their area of investigation.
Regulatory Note: Larazotide holds FDA Fast Track designation for celiac disease but is not yet approved. KPV is not FDA-approved for any indication and has no registered clinical trials.
Mechanism of Action Comparison#
KPV: Inflammatory Suppression via NF-kB#
KPV (Lys-Pro-Val) is the C-terminal tripeptide of alpha-MSH that retains the parent peptide's anti-inflammatory activity. Its primary mechanism involves dose-dependent inhibition of NF-kB, the master transcription factor controlling expression of pro-inflammatory cytokines, chemokines, and adhesion molecules. When NF-kB activation is suppressed, production of TNF-alpha, IL-1beta, IL-6, and IL-8 decreases, reducing inflammatory damage to the intestinal epithelium 1.
A distinguishing feature of KPV is its cellular uptake mechanism. Unlike most peptides that require injection, KPV enters intestinal epithelial cells and immune cells via the PepT1 (SLC15A1) transporter. This is significant because PepT1 expression is upregulated in inflamed intestinal tissue, meaning KPV is preferentially concentrated at sites of active inflammation -- a form of passive targeting 2.
Comparative studies have shown that KPV exerts anti-inflammatory effects comparable to or exceeding those of the full-length alpha-MSH peptide, despite being only three amino acids. This potency is attributed to efficient cellular uptake via PepT1 and retention of the critical C-terminal pharmacophore 3.
Larazotide: Tight Junction Stabilization via Zonulin Antagonism#
Larazotide (AT-1001) is a synthetic octapeptide derived from the Vibrio cholerae zonula occludens toxin (Zot). It functions as a competitive antagonist at the zonulin receptor, preventing zonulin from triggering the intracellular signaling cascade that leads to tight junction disassembly 4.
The zonulin pathway works as follows: when zonulin (or gliadin-derived peptides in celiac disease) binds to its receptor on intestinal epithelial cells, it activates a signaling cascade involving protein kinase C and myosin light chain kinase (MLCK). MLCK phosphorylates the myosin light chain in the perijunctional actinomyosin ring, causing contraction that physically pulls tight junction proteins apart. Larazotide blocks the initial receptor binding event, preventing this entire downstream cascade 4.
Importantly, Larazotide acts locally in the gut lumen. The peptide is designed to have minimal systemic absorption, which limits off-target effects but also means its activity is restricted to the intestinal epithelial surface. This luminal restriction is appropriate for celiac disease (where the trigger arrives luminally as dietary gluten) but potentially limiting for conditions where barrier dysfunction originates from the basolateral side.
Why the Mechanisms Are Complementary#
KPV and Larazotide address gut barrier dysfunction from opposite directions. KPV works intracellularly, reducing the inflammatory mediators that damage tight junctions from within. Larazotide works extracellularly, preventing the signaling events that open tight junctions from the luminal surface. In conditions where both increased permeability and mucosal inflammation are present -- which describes most chronic gut disorders -- the two mechanisms are complementary rather than redundant.
Research Evidence Comparison#
KPV Evidence#
The KPV evidence base is entirely preclinical:
Murine Colitis Models: KPV reduced disease severity in both DSS-induced colitis (modeling ulcerative colitis) and TNBS-induced colitis (modeling Crohn's disease). Oral KPV reduced mucosal inflammation, decreased body weight loss, improved stool consistency, and showed improved histological scores with reduced inflammatory cell infiltration and preserved crypt architecture 5.
In Vitro Studies: KPV inhibited NF-kB activation in colonocytes, macrophages, and dendritic cells at micromolar concentrations. IL-8 production was reduced in a dose-dependent manner in stimulated intestinal epithelial cell lines 2.
PepT1 Transport Studies: The mechanistic basis for oral bioavailability was established in Caco-2 monolayer studies showing active PepT1-mediated transport, with uptake significantly reduced by PepT1 inhibitors 2.
Limitations: Total publication count is modest. No dose-ranging studies have established optimal dosing. No pharmacokinetic data in humans. No safety or toxicology data beyond standard animal study observations.
Larazotide Evidence#
Larazotide has a substantially more advanced evidence base:
Phase 1: Safety and tolerability established in healthy volunteers with dose-proportional pharmacokinetics and minimal systemic absorption confirming the intended luminal mechanism 6.
Phase 2a (n=86): Celiac disease patients on a gluten-free diet exposed to gluten challenge showed that Larazotide (12 mg/day) reduced intestinal permeability (measured by lactulose/mannitol ratio) and gastrointestinal symptoms compared to placebo 6.
Phase 2b (n=342): Larger trial in celiac disease patients confirmed that Larazotide 0.5 mg TID significantly reduced celiac disease symptom scores compared to placebo. The effect was most pronounced in patients with poor symptom control despite a gluten-free diet 7.
Phase 3 (CeliacShield): Demonstrated statistically significant improvement in the number of celiac disease symptom days versus placebo, meeting the primary endpoint. The Phase 3 results support the potential for regulatory approval 8.
FDA Fast Track Designation: Larazotide received Fast Track designation for celiac disease, reflecting the FDA's recognition of an unmet medical need (no approved pharmacotherapy for celiac disease exists beyond dietary gluten avoidance) 8.
Evidence Quality Assessment#
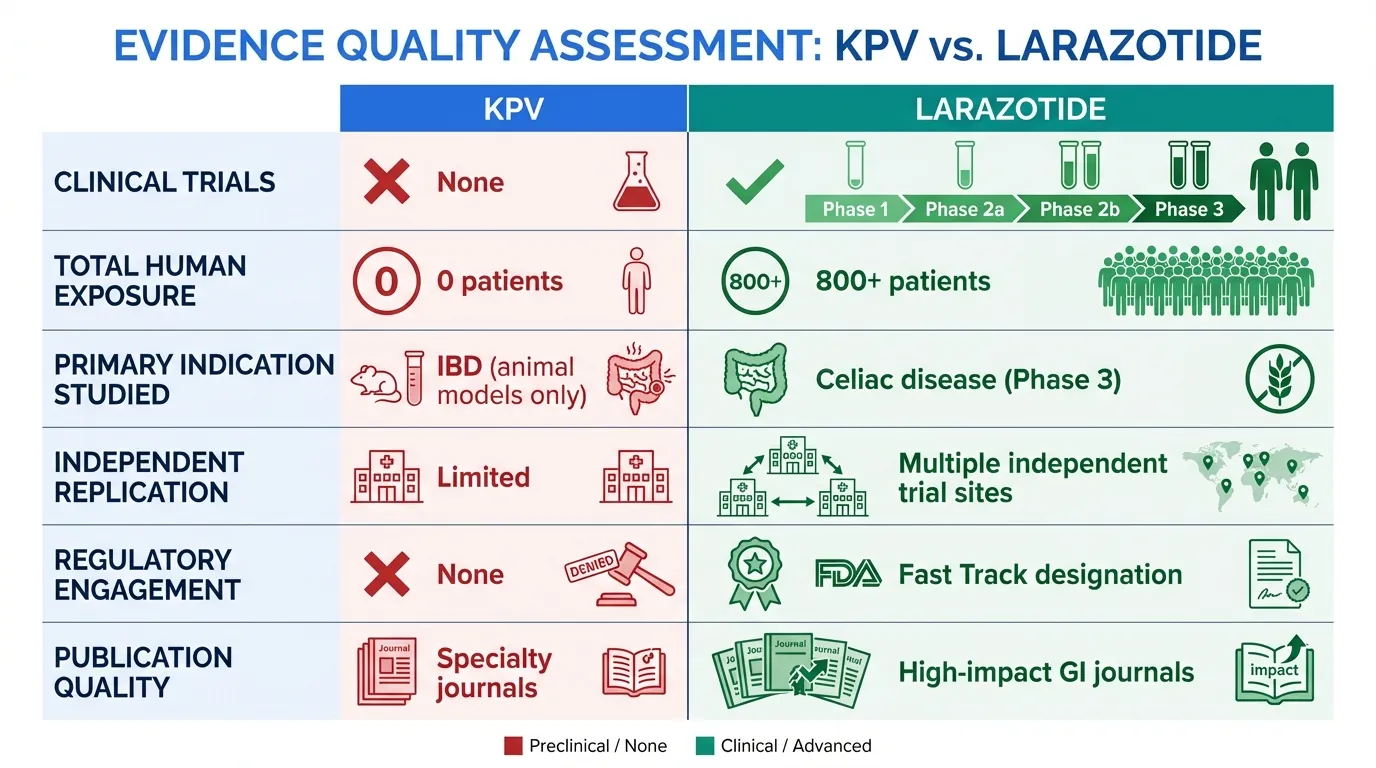
| Metric | KPV | Larazotide |
|---|---|---|
| Clinical trials | None | Phase 1, 2a, 2b, and 3 |
| Total human exposure | 0 | 800+ patients |
| Primary indication studied | IBD (animal models only) | Celiac disease (Phase 3) |
| Independent replication | Limited | Multiple independent trial sites |
| Regulatory engagement | None | FDA Fast Track designation |
| Publication quality | Specialty journals | High-impact GI journals |
Side Effect Profile Comparison#
KPV Safety#
KPV has no human safety data. Animal studies report no significant adverse effects, but the absence of human data means the safety profile is genuinely unknown. Theoretical safety considerations include:
- Melanocortin pathway effects: As an alpha-MSH fragment, KPV could theoretically interact with melanocortin receptors, though its specificity for NF-kB inhibition over MC receptor activation has been demonstrated at relevant concentrations.
- Immunosuppression risk: Chronic NF-kB suppression could theoretically impair immune surveillance, though this concern applies to any anti-inflammatory agent.
- PepT1 competition: KPV could theoretically compete with dietary di- and tripeptides for PepT1-mediated absorption, though the doses studied are unlikely to saturate the transporter.
Larazotide Safety#
Larazotide has a well-characterized safety profile from over 800 patients in clinical trials:
- Adverse event rates comparable to placebo across all trial phases.
- Most common adverse events (headache, URTI, nausea) occurred at similar rates in treatment and placebo groups.
- No clinically significant changes in laboratory values, vital signs, or physical examination.
- Minimal systemic absorption confirmed by pharmacokinetic studies, limiting the potential for systemic side effects 7.
The luminal mechanism and minimal absorption give Larazotide an inherent safety advantage: the peptide acts where it is needed (gut lumen) and does not reach systemic circulation in meaningful quantities.
Gut Health Applications#
Celiac Disease#
Larazotide is the clear candidate for celiac disease. Its mechanism directly addresses the pathophysiology: gliadin peptides trigger zonulin release, zonulin opens tight junctions, gliadin fragments cross the epithelium, and the adaptive immune system mounts a destructive response. By blocking zonulin-mediated tight junction opening, Larazotide interrupts this sequence at an early, targetable step. Phase 3 clinical data validates this approach.
KPV's NF-kB inhibition could theoretically reduce the downstream inflammatory damage in celiac disease, but it does not address the root cause (increased permeability allowing gliadin access to the immune system). No celiac-specific data exists for KPV.
Inflammatory Bowel Disease#
KPV's mechanism is more directly relevant to IBD. In both Crohn's disease and ulcerative colitis, NF-kB-driven inflammation is a central driver of mucosal damage and barrier dysfunction. KPV's demonstrated efficacy in both DSS (UC-like) and TNBS (Crohn's-like) models supports its potential relevance, though the absence of human data is a significant limitation.
Larazotide's tight junction mechanism could contribute to IBD management by reducing permeability, but it does not address the inflammatory component that drives barrier breakdown in IBD. Tight junction dysfunction in IBD is primarily a consequence of inflammation rather than a primary trigger (as it is in celiac disease).
"Leaky Gut" and Increased Intestinal Permeability#
For conditions associated with increased intestinal permeability beyond celiac disease -- including non-celiac gluten sensitivity, irritable bowel syndrome, and environmental enteropathy -- Larazotide's direct tight junction mechanism is the more evidence-based choice. However, if permeability is secondary to chronic low-grade inflammation, KPV's anti-inflammatory approach addresses the upstream cause.
Accessibility and Practical Considerations#
KPV#
KPV is available through research peptide suppliers. Its small size (3 amino acids) makes it relatively inexpensive to synthesize. The demonstrated oral bioavailability via PepT1 is a practical advantage, though no standardized oral dosing has been established in humans. Sublingual and topical formulations have also been discussed in research contexts.
Larazotide#
Larazotide is not commercially available as an approved drug. Access is currently limited to clinical trial enrollment or specialized research procurement. If approved for celiac disease, it would be available by prescription as an oral capsule. The FDA Fast Track designation could accelerate the regulatory timeline. Larazotide's oral capsule formulation is designed for practical clinical use, with TID dosing established in clinical trials.
Key Differences#
- Mechanism: KPV inhibits intracellular inflammatory signaling (NF-kB). Larazotide blocks extracellular tight junction disassembly (zonulin antagonism).
- Evidence tier: Larazotide has Phase 3 clinical data. KPV has only preclinical data.
- Primary indication: Larazotide was developed for celiac disease. KPV has been studied in IBD models.
- Systemic effects: KPV has potential systemic anti-inflammatory effects. Larazotide acts locally with minimal absorption.
- Current availability: KPV is accessible through research suppliers. Larazotide is not commercially available.
- Oral use: Both can be administered orally, but through different mechanisms -- KPV via active PepT1 transport, Larazotide via luminal activity without absorption.
- Combination rationale: The mechanisms are complementary (inflammatory suppression plus structural barrier reinforcement), but no combination studies exist.
Conclusion#
KPV and Larazotide demonstrate that "gut barrier health" is not a single therapeutic target but a complex system addressable from multiple angles. Larazotide's zonulin antagonism directly reinforces the structural tight junction barrier and has the clinical data to support it -- Phase 3 results for celiac disease represent the most advanced clinical program for any gut barrier peptide. KPV's NF-kB inhibition addresses the inflammatory driver of barrier dysfunction and is mechanistically well-suited to IBD, but it remains entirely preclinical.
For researchers studying celiac disease, Larazotide is the evidence-based choice. For those focused on inflammatory bowel disease, KPV has the more directly relevant mechanism but lacks human validation. The complementary nature of their mechanisms suggests that combination approaches could be valuable, but this remains a theoretical consideration without supporting clinical data. Both peptides underscore an important principle in gut barrier research: the optimal intervention depends on whether increased permeability is the cause or the consequence of the underlying condition.
References#
Further Reading#
- KPV Overview and Research Guide
- KPV Side Effects
- KPV Dosing Protocols
- Larazotide Overview and Research Guide
- Larazotide Side Effects
- Larazotide Dosing Protocols
Footnotes#
-
Brzoska T, Luger TA, Maaser C, Abels C, Bohm M. Alpha-melanocyte-stimulating hormone and related tripeptides: biochemistry, antiinflammatory and protective effects. Endocr Rev. 2008;29(5):581-602. PMID: 18612058. ↩
-
Dalmasso G, Charrier-Hisamuddin L, Nguyen HT, Yan Y, Sitaraman S, Merlin D. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008;134(1):166-178. PMID: 18061177. ↩ ↩2 ↩3
-
Catania A, Gatti S, Colombo G, Lipton JM. Targeting melanocortin receptors as a novel strategy to control inflammation. Pharmacol Rev. 2004;56(1):1-29. PMID: 15001661. ↩
-
Fasano A. Zonulin and its regulation of intestinal barrier function: the biological door to inflammation, autoimmunity, and cancer. Physiol Rev. 2011;91(1):151-175. PMID: 21248165. ↩ ↩2
-
Laroui H, Dalmasso G, Nguyen HT, Yan Y, Sitaraman SV, Merlin D. Drug-loaded nanoparticles targeted to the colon with polysaccharide hydrogel reduce colitis in a mouse model. Gastroenterology. 2010;138(3):843-853. PMID: 19909746. ↩
-
Paterson BM, Lammers KM, Arrieta MC, Fasano A, Meddings JB. The safety, tolerance, pharmacokinetic and pharmacodynamic effects of single doses of AT-1001 in coeliac disease subjects: a proof of concept study. Aliment Pharmacol Ther. 2007;26(5):757-766. PMID: 17697209. ↩ ↩2
-
Leffler DA, Kelly CP, Green PH, et al. Larazotide acetate for persistent symptoms of celiac disease despite a gluten-free diet: a randomized controlled trial. Gastroenterology. 2015;148(7):1311-1319. PMID: 25683116. ↩ ↩2
-
Kelly CP, Green PH, Murray JA, et al. Larazotide acetate in patients with coeliac disease undergoing a gluten challenge: a randomised placebo-controlled study. Aliment Pharmacol Ther. 2013;37(2):252-262. PMID: 23163616. ↩ ↩2

{kind=link}
{kind=link}
Which Is Better For...
Celiac Disease Research
Larazotide
Larazotide was specifically developed for celiac disease, has Phase 3 clinical trial data demonstrating reduced symptom days, and holds FDA Fast Track designation. KPV has no celiac-specific data.
Inflammatory Bowel Disease Research
KPV
KPV's NF-kB inhibition directly targets the inflammatory pathology of IBD, with preclinical efficacy in both Crohn's and UC models. Larazotide's tight junction mechanism is less directly relevant to established IBD inflammation.
General Gut Barrier Support
Larazotide
Larazotide directly stabilizes tight junctions, the structural basis of gut barrier integrity, and has human clinical data. KPV supports barrier function indirectly through inflammation reduction but lacks human evidence.
Current Accessibility for Research
KPV
KPV is available through research peptide suppliers and has demonstrated oral bioavailability. Larazotide is not commercially available outside clinical trials or specialized research procurement.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About KPV vs Larazotide: Two Approaches to Gut Barrier Health
Which is better, KPV or Larazotide?
KPV and Larazotide target gut barrier health through fundamentally different mechanisms: KPV suppresses the inflammatory signaling (NF-kB) that damages the gut barrier, while Larazotide directly stabilizes tight junctions by blocking zonulin-mediated permeability. Larazotide has a vastly stronger evidence base, with Phase 3 clinical data for celiac disease, FDA Fast Track designation, and safety data from 800+ patients. KPV remains entirely preclinical with no human clinical trials. For condi... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between KPV and Larazotide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to Larazotide; Side Effect Profile: advantage goes to Larazotide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Larazotide over KPV?
For the scenario of "Celiac Disease Research," research data suggests Larazotide may be more relevant. Larazotide was specifically developed for celiac disease, has Phase 3 clinical trial data demonstrating reduced symptom days, and holds FDA Fast Track designation. KPV has no celiac-specific data.. This is based on currently available evidence and individual circumstances may differ.
How do KPV and Larazotide differ in their mechanisms of action?
KPV: Alpha-MSH-derived tripeptide (Lys-Pro-Val) that inhibits NF-kB activation in a dose-dependent manner, suppressing pro-inflammatory cytokines (TNF-alpha, IL-1beta, IL-6, IL-8). Enters cells via PepT.... Larazotide: Synthetic octapeptide (AT-1001) that acts as a zonulin receptor antagonist, preventing zonulin-mediated opening of intestinal tight junctions. Directly targets paracellular permeability by stabiliz....
Which has fewer side effects, KPV or Larazotide?
In terms of side effects and tolerability, the advantage goes to Larazotide. KPV: No human safety data exists. Animal studies report no significant adverse effects at studied doses. As a naturally derived tripeptide fragment of a.... Larazotide: Well-characterized safety profile from multiple clinical trials. Side effects comparable to placebo in Phase 2 and Phase 3 studies. Most common adv....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.