HCG vs HMG: Gonadotropin Hormones for Fertility Compared
HCG vs HMG compared for fertility and testosterone support — mechanisms, clinical applications, and reproductive endocrinology uses.
Verdict at a Glance
HCG and HMG serve complementary rather than competing roles in reproductive medicine. HCG provides LH-like activity for triggering ovulation, maintaining Leydig cell function, and supporting testosterone production. HMG provides combined FSH and LH activity essential for follicular development in IVF and ovulation induction protocols. In male applications, HCG has the broader role. In female fertility, both are routinely used together in sequential protocols where HMG stimulates follicular growth and HCG triggers final oocyte maturation.
| Best for | Pick | Why |
|---|---|---|
| Male testosterone support during TRT | HCG | LH-mimetic activity maintains Leydig cell function and intratesticular testosterone, preserving fertility potential during exogenous testosterone |
| Controlled ovarian stimulation for IVF | HMG | Dual FSH/LH activity promotes multi-follicular development needed for oocyte retrieval in assisted reproduction |
| Ovulation trigger in fertility protocols | HCG | LH surge mimic triggers final oocyte maturation and ovulation at precise timing in stimulated cycles |
| Male hypogonadotropic hypogonadism with infertility | HMG | FSH component is essential for spermatogenesis initiation; often used in combination with HCG for complete gonadotropin replacement |
| Category | HCG | HMG | Advantage |
|---|---|---|---|
| Mechanism of Action | Glycoprotein that mimics LH by binding the LH/CG receptor (LHCGR); stimulates Leydig cell testosterone production in males and triggers ovulation in females via Gs-cAMP-PKA steroidogenic signaling | Purified preparation containing both FSH and LH activity from postmenopausal urine; stimulates follicular development (FSH) and steroidogenesis (LH) simultaneously | Comparable |
| Research Evidence | FDA-approved for hypogonadism, cryptorchidism, and ovulation induction; decades of clinical use; extensive pharmacology literature | FDA-approved for ovulation induction and controlled ovarian stimulation; standard of care in IVF protocols; well-established clinical evidence | Comparable |
| Side Effect Profile | Ovarian hyperstimulation syndrome risk in women; gynecomastia possible in men; headache; injection site reactions; estrogen elevation from aromatization of increased testosterone | Ovarian hyperstimulation syndrome risk (primary concern); multiple pregnancy risk; injection site reactions; requires careful monitoring with ultrasound and estradiol levels | Comparable |
| Clinical Applications | Male hypogonadism, cryptorchidism, ovulation trigger in IVF, Leydig cell function preservation during TRT; broad range across male and female fertility | Controlled ovarian hyperstimulation for IVF, ovulation induction in anovulatory women, male hypogonadotropic hypogonadism; primarily female fertility focused | HCG |
| Hormonal Target | Exclusively LH-like activity; stimulates testosterone and progesterone production; no direct FSH activity | Dual FSH and LH activity in a single preparation; directly stimulates follicular growth and maturation alongside steroidogenesis | HMG |

Introduction#
HCG and HMG are both gonadotropin preparations used extensively in reproductive medicine, but they provide different hormonal activities. HCG (human chorionic gonadotropin) mimics LH to stimulate steroidogenesis and trigger ovulation. HMG (human menopausal gonadotropin/menotropin) provides both FSH and LH activity, making it essential for follicular development in assisted reproduction.
Understanding when each is appropriate, and how they are often used together, is fundamental to reproductive endocrinology.
Quick Comparison#
| Feature | HCG | HMG |
|---|---|---|
| Type | Glycoprotein hormone | Gonadotropin mixture |
| Molecular Weight | ~36,700 Da | Variable (FSH + LH) |
| Hormonal Activity | LH-like only | FSH + LH combined |
| Source | Placental (pregnancy urine) or recombinant | Postmenopausal urine extract |
| FDA Indications | Hypogonadism, cryptorchidism, ovulation | Ovulation induction, IVF stimulation |
| Brand Names | Pregnyl, Novarel, Ovidrel | Menopur, Repronex |
| Primary Male Use | Testosterone support, Leydig cell maintenance | Spermatogenesis initiation |
| Primary Female Use | Ovulation trigger | Follicular development |
| Research Status | Approved | Approved |
Mechanism of Action Comparison#
HCG#
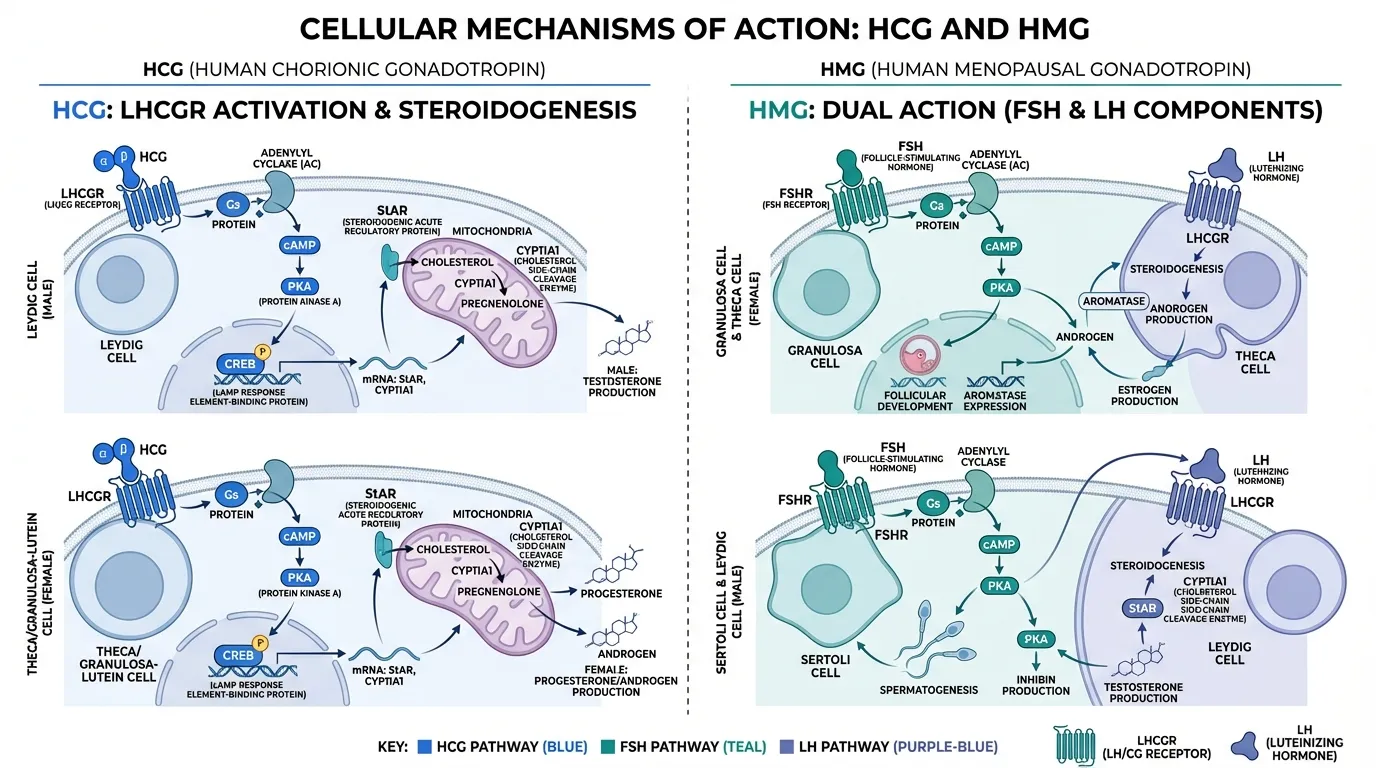
HCG is a heterodimeric glycoprotein that binds and activates the LH/chorionic gonadotropin receptor (LHCGR), a class A GPCR on gonadal and reproductive tissues. HCG is approximately fivefold more potent than LH for cAMP generation and produces slower, sustained signaling kinetics.
Receptor activation initiates the Gs-adenylyl cyclase-cAMP-PKA cascade, phosphorylating CREB and promoting transcription of steroidogenic genes including StAR (steroidogenic acute regulatory protein) and CYP11A1. This drives cholesterol transfer to mitochondria and conversion to pregnenolone, the first step in steroid hormone synthesis.
In males, LHCGR activation on Leydig cells stimulates testosterone production. In females, HCG acts on theca cells for androgen production and on granulosa-lutein cells for progesterone synthesis. HCG also promotes beta-arrestin recruitment, endosomal signaling, MAPK/ERK activation, and angiogenic signaling through VEGF and EG-VEGF pathways.
HMG#
HMG is a purified preparation extracted from the urine of postmenopausal women, containing both follicle-stimulating hormone (FSH) and luteinizing hormone (LH) activity in approximately equal proportions. Modern highly purified HMG preparations (such as Menopur) contain FSH activity supplemented with hCG-derived LH activity.
The FSH component binds the FSH receptor (FSHR) on granulosa cells in females and Sertoli cells in males, activating Gs-cAMP-PKA signaling to promote follicular development, aromatase expression, and spermatogenesis. The LH component activates LHCGR on theca and Leydig cells for steroidogenesis.
The dual activity makes HMG unique: it simultaneously drives follicular maturation (FSH) and provides the steroidogenic environment (LH) needed for optimal oocyte development. This combined activity is why HMG remains a standard of care in IVF protocols despite the availability of recombinant FSH.
Evidence and Research Comparison#
HCG Research#
- Male hypogonadism: FDA-approved for hypogonadotropic hypogonadism; restores intratesticular testosterone and supports spermatogenesis
- Cryptorchidism: Approved for stimulating testicular descent in prepubertal males
- Ovulation induction: Standard ovulation trigger in IVF and IUI protocols; mimics the endogenous LH surge
- TRT adjunct: Widely used to maintain Leydig cell function and testicular volume during exogenous testosterone therapy
- Pregnancy maintenance: Endogenous HCG maintains the corpus luteum during early pregnancy
HMG Research#
- IVF stimulation: Standard of care for controlled ovarian hyperstimulation; multiple meta-analyses comparing HMG with recombinant FSH
- Ovulation induction: FDA-approved for anovulatory infertility in women who have failed clomiphene
- Male infertility: Used in combination with HCG for spermatogenesis induction in hypogonadotropic hypogonadism
- HMG vs rFSH debate: Ongoing clinical discussion about whether HMG's LH component improves IVF outcomes compared to pure recombinant FSH; some meta-analyses suggest higher live birth rates with HMG
Side Effects and Safety Comparison#
HCG Side Effects#
- OHSS: Ovarian hyperstimulation syndrome risk when used as ovulation trigger
- Gynecomastia: Possible in males due to increased estrogen from aromatization
- Headache and injection site reactions: Common mild adverse effects
- Multiple pregnancy: Risk when used for ovulation induction
- Mood changes: Reported by some patients
HMG Side Effects#
- OHSS: Primary safety concern; requires careful monitoring with serial ultrasound and estradiol levels
- Multiple pregnancy: Significant risk with ovulation induction; careful dose titration required
- Injection site reactions: Pain, redness, and swelling
- Allergic reactions: Rare; urinary-derived products carry theoretical immunogenicity risk
- Monitoring burden: Requires frequent clinical visits during stimulation cycles
Dosing and Administration Comparison#
HCG Dosing#
| Parameter | Details |
|---|---|
| Route | Intramuscular or subcutaneous |
| Ovulation trigger | 5,000-10,000 IU single dose (or 250 mcg recombinant) |
| Male hypogonadism | 1,000-2,000 IU 2-3 times weekly |
| TRT adjunct | 500-1,000 IU 2-3 times weekly |
| Cryptorchidism | 1,000-5,000 IU, variable schedules |
| Formulations | Urinary-derived (Pregnyl) or recombinant (Ovidrel) |
HMG Dosing#
| Parameter | Details |
|---|---|
| Route | Intramuscular or subcutaneous |
| IVF stimulation | 150-450 IU daily, adjusted by response |
| Ovulation induction | 75-150 IU daily, titrated to ultrasound |
| Male infertility | 75-150 IU 3 times weekly (with HCG) |
| Monitoring | Serial ultrasound + estradiol levels required |
| Duration | 7-12 days per stimulation cycle |
Use Case Recommendations#
Choose HCG When:#
- Ovulation triggering is needed at precise timing in stimulated IVF or IUI cycles
- Male testosterone support during TRT to maintain Leydig cell function
- Cryptorchidism treatment in pediatric patients
- LH-like activity is specifically needed without FSH stimulation
- Luteal phase support is required after embryo transfer
Choose HMG When:#
- Follicular development is the goal in IVF controlled ovarian stimulation
- Combined FSH/LH activity is needed in a single preparation
- Spermatogenesis induction requires FSH for Sertoli cell support (combined with HCG)
- Anovulatory infertility has not responded to clomiphene
- LH supplementation is desired alongside FSH during ovarian stimulation
Can They Be Combined?#
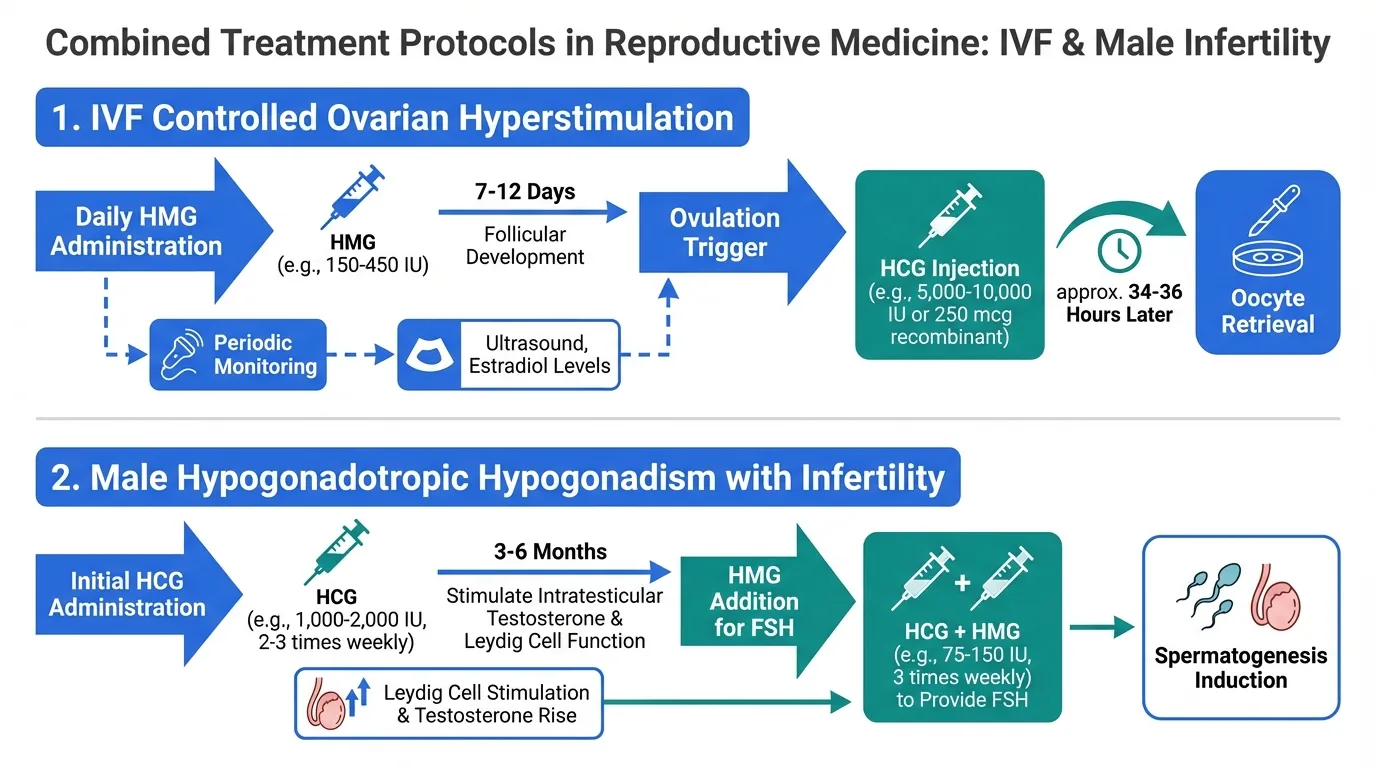
HCG and HMG are routinely used together in reproductive medicine. The most common protocol involves HMG for ovarian stimulation (providing FSH and LH for follicular growth) followed by a single HCG injection as the ovulation trigger (providing the LH surge for final oocyte maturation). This sequential combination is the foundation of most IVF protocols.
In male infertility, HCG is used first to stimulate testosterone production (often for 3-6 months), then HMG is added to provide the FSH necessary for spermatogenesis initiation. This combined approach is standard for treating hypogonadotropic hypogonadism with infertility.
For additional context on reproductive peptides, see our comparison of gonadorelin vs triptorelin and our profiles on kisspeptin and gonadorelin.
Verdict#
HCG and HMG are complementary gonadotropin preparations rather than true competitors. HCG provides LH-like activity for testosterone stimulation, ovulation triggering, and Leydig cell maintenance. HMG provides the combined FSH/LH activity essential for follicular development and spermatogenesis support.
In clinical practice, the question is rarely "which one" but "when each one." HMG drives the development phase (follicle growth, spermatogenesis initiation), while HCG provides the triggering and maintenance functions (ovulation, testosterone production). Together, they form the hormonal backbone of assisted reproduction and male fertility treatment.
For related comparisons, see gonadorelin vs triptorelin, and explore our dosing calculator for weight-based dosing estimation.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Male testosterone support during TRT
HCG
LH-mimetic activity maintains Leydig cell function and intratesticular testosterone, preserving fertility potential during exogenous testosterone
Controlled ovarian stimulation for IVF
HMG
Dual FSH/LH activity promotes multi-follicular development needed for oocyte retrieval in assisted reproduction
Ovulation trigger in fertility protocols
HCG
LH surge mimic triggers final oocyte maturation and ovulation at precise timing in stimulated cycles
Male hypogonadotropic hypogonadism with infertility
HMG
FSH component is essential for spermatogenesis initiation; often used in combination with HCG for complete gonadotropin replacement
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About HCG vs HMG: Gonadotropin Hormones for Fertility Compared
Which is better, HCG or HMG?
HCG and HMG serve complementary rather than competing roles in reproductive medicine. HCG provides LH-like activity for triggering ovulation, maintaining Leydig cell function, and supporting testosterone production. HMG provides combined FSH and LH activity essential for follicular development in IVF and ovulation induction protocols. In male applications, HCG has the broader role. In female fertility, both are routinely used together in sequential protocols where HMG stimulates follicular gr... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between HCG and HMG?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to neither (tie); Side Effect Profile: advantage goes to neither (tie). 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider HCG over HMG?
For the scenario of "Male testosterone support during TRT," research data suggests HCG may be more relevant. LH-mimetic activity maintains Leydig cell function and intratesticular testosterone, preserving fertility potential during exogenous testosterone. This is based on currently available evidence and individual circumstances may differ.
How do HCG and HMG differ in their mechanisms of action?
HCG: Glycoprotein that mimics LH by binding the LH/CG receptor (LHCGR); stimulates Leydig cell testosterone production in males and triggers ovulation in females via Gs-cAMP-PKA steroidogenic signaling. HMG: Purified preparation containing both FSH and LH activity from postmenopausal urine; stimulates follicular development (FSH) and steroidogenesis (LH) simultaneously.
Which has fewer side effects, HCG or HMG?
In terms of side effects and tolerability, the advantage goes to neither (comparable). HCG: Ovarian hyperstimulation syndrome risk in women; gynecomastia possible in men; headache; injection site reactions; estrogen elevation from aromatiz.... HMG: Ovarian hyperstimulation syndrome risk (primary concern); multiple pregnancy risk; injection site reactions; requires careful monitoring with ultra....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.