Gonadorelin vs Triptorelin: Native GnRH vs Long-Acting Agonist
Gonadorelin vs triptorelin compared: stimulatory vs suppressive GnRH effects, HPG axis modulation, and clinical applications.
Verdict at a Glance
Gonadorelin and triptorelin produce opposite clinical outcomes despite targeting the same receptor. Gonadorelin stimulates LH/FSH release and supports the HPG axis, making it essential for diagnostic testing and fertility applications. Triptorelin suppresses the axis through sustained receptor desensitization, providing chemical castration for hormone- dependent conditions. The choice is entirely determined by the clinical goal: stimulation and axis support (gonadorelin) versus suppression and hormone deprivation (triptorelin). Triptorelin has the broader range of FDA-approved indications and the convenience of depot formulations.
| Best for | Pick | Why |
|---|---|---|
| Pituitary function diagnostic testing | Gonadorelin | FDA-approved for evaluating pituitary gonadotroph function; acute LH/FSH stimulation test with rapid assessment |
| Advanced prostate cancer treatment | Triptorelin | FDA-approved for androgen deprivation therapy with depot formulations providing months of sustained castrate testosterone levels |
| Fertility support and HPG axis stimulation | Gonadorelin | Stimulates endogenous LH/FSH release to support gonadal function; used in pulsatile protocols for hypothalamic amenorrhea |
| Endometriosis or uterine fibroid management | Triptorelin | Suppresses estrogen to menopausal levels, reducing endometriotic lesion activity and fibroid volume |
| Category | Gonadorelin | Triptorelin | Advantage |
|---|---|---|---|
| Mechanism of Action | Synthetic decapeptide identical to native GnRH; stimulates pulsatile LH and FSH release from anterior pituitary gonadotrophs via Gq/11-PLC-Ca2+ signaling; short half-life maintains physiological signaling patterns | GnRH agonist with D-Trp6 substitution conferring metabolic stability; initial stimulatory flare followed by pituitary desensitization and gonadotropin suppression; produces chemical castration with continuous use | Comparable |
| Research Evidence | FDA-approved for diagnostic testing of pituitary gonadotroph function; used in fertility protocols; well-characterized pharmacology with decades of clinical experience | FDA-approved for prostate cancer, endometriosis, central precocious puberty, and uterine fibroids; extensive Phase 3 data; available in depot formulations (1, 3, and 6 month) | Triptorelin |
| Side Effect Profile | Generally well-tolerated; transient headache, nausea, and flushing; minimal systemic effects due to short half-life; does not cause sustained hormone suppression | Initial testosterone/estrogen flare (1-2 weeks); sustained castrate hormone levels with hot flashes, bone density loss, sexual dysfunction, and metabolic changes; reversible upon discontinuation | Gonadorelin |
| Dosing Complexity | Short half-life (minutes) requires pulsatile or frequent administration for sustained effect; single-dose IV/SC for diagnostic testing; pump delivery for therapeutic use | Available in convenient depot formulations providing 1, 3, or 6 months of continuous GnRH receptor stimulation from a single injection | Triptorelin |
| Clinical Applications | Diagnostic testing, fertility treatment support, pulsatile GnRH replacement for hypothalamic amenorrhea; stimulates rather than suppresses the HPG axis | Prostate cancer (androgen deprivation), endometriosis, uterine fibroids, central precocious puberty, gender-affirming care, fertility preservation; suppresses the HPG axis | Triptorelin |

Introduction#
Gonadorelin and triptorelin both act on the GnRH receptor, yet they produce diametrically opposite clinical outcomes. Gonadorelin, identical to native GnRH, stimulates LH and FSH release to support reproductive function. Triptorelin, a modified GnRH analog with enhanced stability, produces initial stimulation followed by sustained pituitary desensitization that suppresses gonadal hormones to castrate levels.
This paradox, where agonists at the same receptor produce opposite effects, is one of the most elegant examples of temporal signaling dynamics in endocrinology. Understanding this mechanism is essential for selecting the appropriate peptide for a given clinical context.
Quick Comparison#
| Feature | Gonadorelin | Triptorelin |
|---|---|---|
| Structure | Native GnRH decapeptide | GnRH with D-Trp6 substitution |
| Molecular Weight | 1,182 Da | 1,311 Da |
| Half-Life | ~2-4 minutes | ~3-5 hours (peptide); months (depot) |
| Net HPG Effect | Stimulatory | Suppressive (after initial flare) |
| LH/FSH | Increases acutely | Suppresses chronically |
| Testosterone/Estrogen | Supports production | Reduces to castrate levels |
| FDA Indications | Diagnostic pituitary testing | Prostate cancer, endometriosis, CPP, fibroids |
| Brand Names | Factrel | Trelstar, Decapeptyl, Gonapeptyl |
| Formulations | IV/SC single dose | Depot IM (1, 3, 6 month) |
Mechanism of Action Comparison#
Gonadorelin#
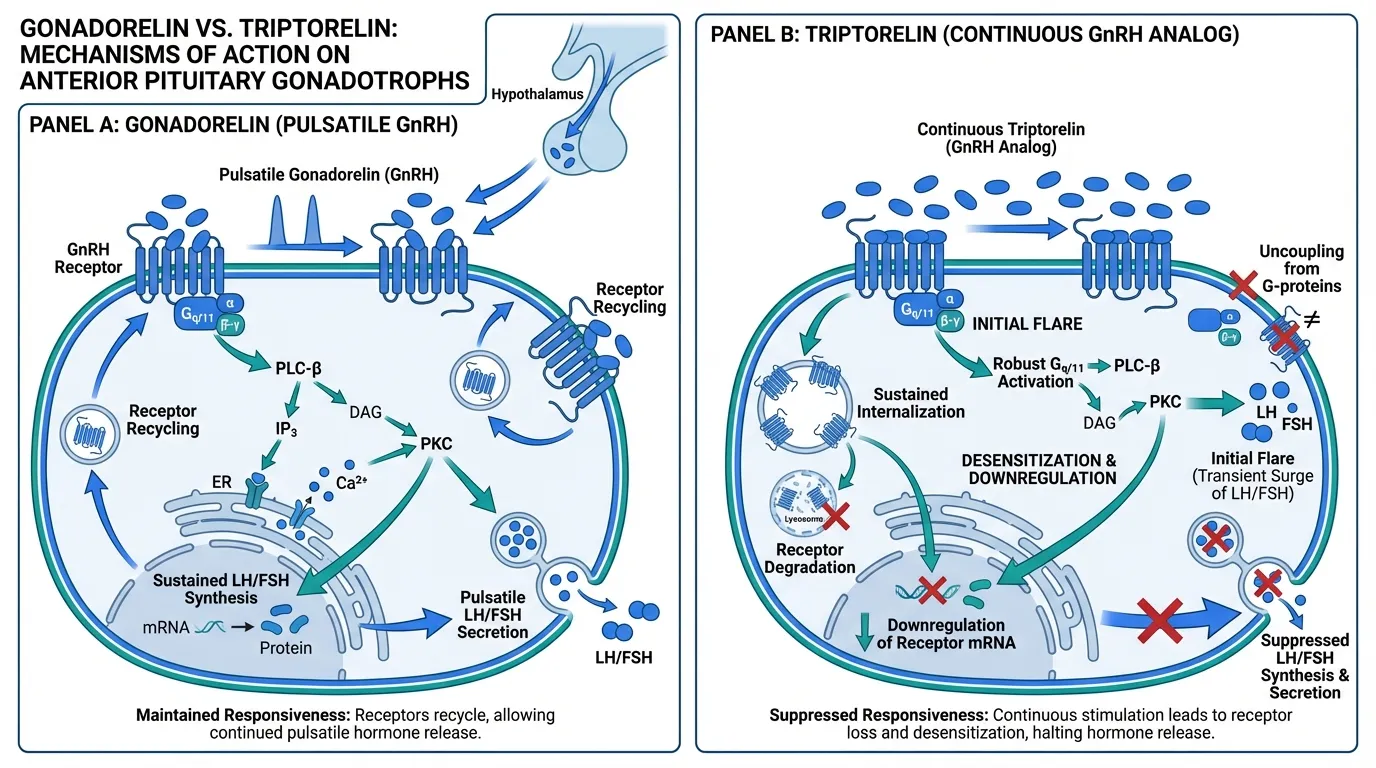
Gonadorelin is a synthetic decapeptide identical in sequence to endogenous gonadotropin-releasing hormone (pGlu-His-Trp-Ser-Tyr-Gly-Leu-Arg-Pro-Gly-NH2). It binds the type I GnRH receptor on anterior pituitary gonadotrophs, a seven-transmembrane GPCR that predominantly couples to Gq/11.
Receptor activation triggers phospholipase C beta (PLC-beta), generating IP3 and DAG from PIP2. IP3 mobilizes calcium from endoplasmic reticulum stores (the initial spike), while DAG activates PKC and promotes L-type calcium channel opening (sustained plateau). These combined Ca2+/PKC signals drive:
- Immediate secretion: Exocytosis of stored LH and FSH granules within minutes
- MAPK activation: ERK1/2 and JNK activation driving Egr-1, c-Fos, and AP-1 transcription factors
- Gene expression: LH-beta, FSH-beta, and common alpha-subunit (CGA) gene transcription
A critical feature of gonadorelin is its short half-life (~2-4 minutes), which allows it to mimic the pulsatile secretion pattern of endogenous GnRH. This pulsatility is essential: the pituitary decodes GnRH pulse frequency to determine the ratio of LH to FSH output. Low-frequency pulses favor FSH-beta through cAMP/CREB and NFAT pathways, while higher-frequency pulses favor LH-beta through ERK/Egr-1.
Because the type I GnRH receptor uniquely lacks a cytoplasmic C-terminal tail, it is relatively resistant to rapid beta-arrestin-mediated desensitization, which helps maintain signaling responsiveness to each pulse.
Triptorelin#
Triptorelin shares 9 of 10 amino acids with native GnRH but substitutes D-tryptophan for glycine at position 6. This single change produces two critical pharmacological consequences:
- Metabolic stability: D-amino acid substitution confers resistance to enzymatic degradation, extending the half-life from minutes to hours
- Enhanced receptor affinity: Increased binding affinity for the GnRH receptor
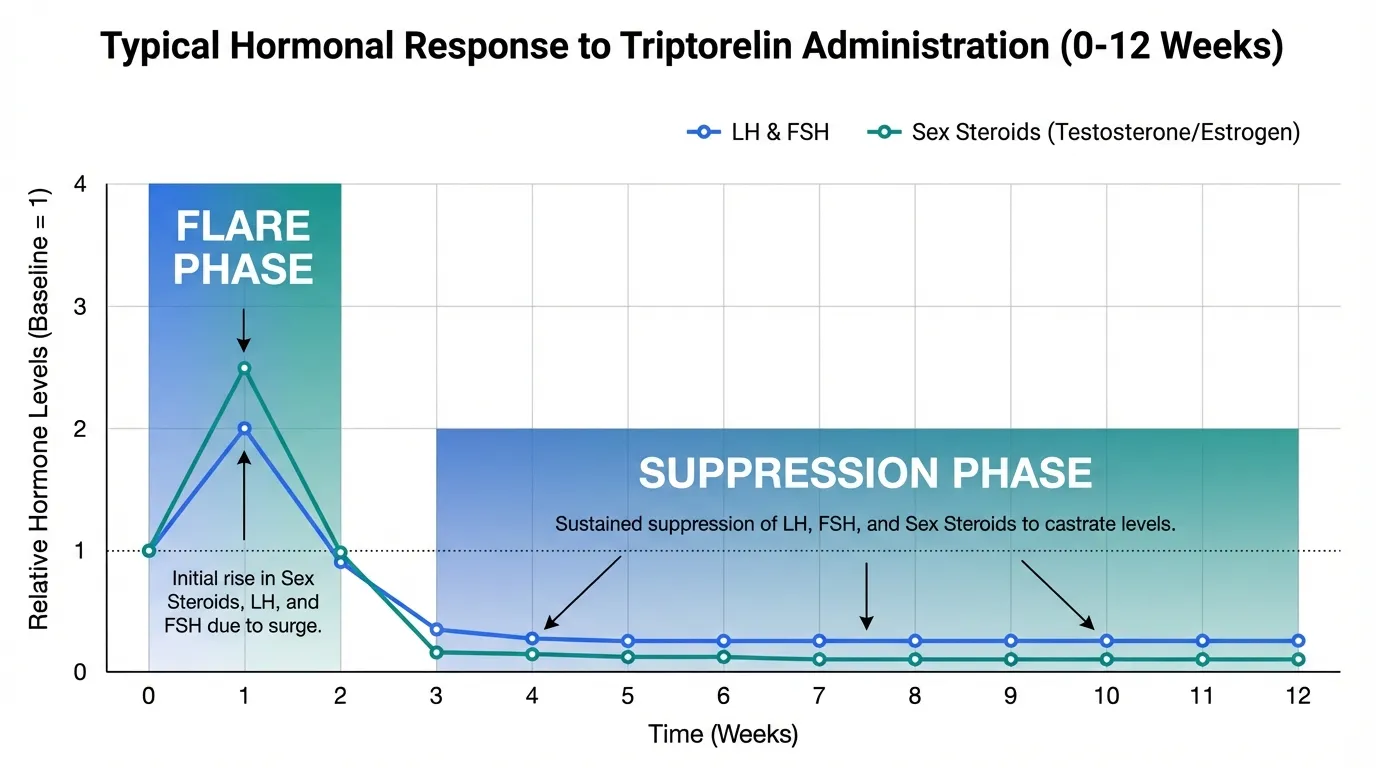
The result is continuous, non-pulsatile GnRH receptor stimulation, which triggers the hallmark biphasic response:
Phase 1 (Flare, weeks 1-2): Initial receptor activation produces robust LH and FSH secretion, temporarily increasing sex steroids. Testosterone may rise 50-100% above baseline in men during this period.
Phase 2 (Desensitization, week 2+): Continuous receptor occupation leads to receptor internalization and degradation, uncoupling of Gq/11 signaling, downregulation of GnRH receptor mRNA, induction of MAPK phosphatases, and suppression of gonadotropin gene expression. LH and FSH fall to castrate levels, with downstream sex steroids following.
In depot formulations, triptorelin is formulated in biodegradable microspheres that provide sustained release over 1, 3, or 6 months, maintaining continuous suppression from a single injection.
Evidence and Research Comparison#
Gonadorelin Research#
Gonadorelin has established clinical utility in specific applications:
- Diagnostic testing: FDA-approved as a diagnostic agent for evaluating pituitary gonadotroph function; a GnRH stimulation test measures LH/FSH response to distinguish hypothalamic from pituitary causes of hypogonadism
- Pulsatile GnRH therapy: Used with portable infusion pumps for treating hypothalamic amenorrhea and infertility, where the hypothalamus fails to produce adequate GnRH pulses
- Fertility protocols: Applied in some assisted reproduction protocols to stimulate endogenous gonadotropin release
- Research tool: Standard pharmacological tool for studying GnRH receptor signaling, pulse-frequency decoding, and gonadotroph physiology
The clinical evidence is robust for diagnostic use and well-established for pulsatile fertility applications, though the latter requires specialized pump delivery systems.
Triptorelin Research#
Triptorelin has an extensive clinical evidence base across multiple indications:
- Prostate cancer: Multiple Phase 3 trials demonstrating sustained testosterone suppression to castrate levels; non-inferior to surgical castration for advanced prostate cancer; available as 1-month (Trelstar), 3-month, and 6-month depot formulations
- Endometriosis: Controlled trials showing reduction in endometriotic lesion activity and pain scores with 3-6 months of treatment
- Central precocious puberty: Demonstrated efficacy in halting premature sexual development and preserving adult height potential
- Uterine fibroids: Evidence for fibroid volume reduction and symptom improvement
- Fertility preservation: The PROMISE-GIM6 trial demonstrated that triptorelin administered during chemotherapy preserved ovarian function in premenopausal breast cancer patients
- Gender-affirming care: Used as a puberty blocker in adolescent gender-affirming protocols
Triptorelin has the broader regulatory portfolio, with FDA approval for four distinct indications and widespread use in additional off-label contexts.
Side Effects and Safety Comparison#
Gonadorelin Side Effects#
Gonadorelin's short duration of action limits its side effect profile:
- Common: Transient headache, nausea, light-headedness, and flushing following injection
- Local: Injection site reactions with IV or SC administration
- Hormonal: Brief LH/FSH spike producing transient sex steroid elevation; no sustained hormonal disruption
- Allergic: Rare hypersensitivity reactions possible
- Key advantage: Does not cause sustained hormone suppression or the cascade of hypogonadal symptoms seen with long-acting agonists
The short half-life and transient receptor engagement make gonadorelin one of the most well-tolerated reproductive peptides.
Triptorelin Side Effects#
Triptorelin's therapeutic mechanism (sustained hormone suppression) is itself the source of most side effects:
- Initial flare: Temporary worsening of hormone-dependent symptoms during weeks 1-2; in prostate cancer, this can cause bone pain, urinary obstruction, or spinal cord compression (requiring anti-androgen cover)
- Hypogonadal symptoms: Hot flashes, decreased libido, erectile dysfunction (men), vaginal dryness (women)
- Bone health: Decreased bone mineral density with prolonged use; increased fracture risk
- Metabolic: Altered lipid profiles, potential insulin resistance, body composition changes
- Cardiovascular: Increased cardiovascular risk with long-term androgen deprivation in men
- Mood: Depression, fatigue, cognitive changes reported in some patients
- Reversibility: Effects generally reverse after discontinuation, though recovery may take weeks to months
The side effect burden is directly proportional to treatment duration. Short-term use (3-6 months for endometriosis) carries less risk than long-term androgen deprivation for prostate cancer.
Dosing and Administration Comparison#
Gonadorelin Dosing#
| Parameter | Details |
|---|---|
| Route | Intravenous or subcutaneous |
| Diagnostic dose | 100 mcg single IV bolus |
| Pulsatile therapy | 5-20 mcg per pulse via pump every 60-120 min |
| Half-life | ~2-4 minutes |
| Assessment | LH/FSH measured at 15, 30, 45, 60, and 120 min post-injection |
| Storage | Room temperature (powder); refrigerated after reconstitution |
Triptorelin Dosing#
| Parameter | Details |
|---|---|
| Route | Intramuscular injection (depot) |
| 1-month depot | 3.75 mg IM every 4 weeks |
| 3-month depot | 11.25 mg IM every 12 weeks |
| 6-month depot | 22.5 mg IM every 24 weeks |
| Onset of suppression | 2-4 weeks after first injection |
| Storage | Room temperature; ready-to-use kits |
The dosing convenience strongly favors triptorelin: a single depot injection provides months of therapeutic effect, whereas gonadorelin requires either acute single dosing (diagnostic) or continuous pulsatile pump delivery (therapeutic).
Use Case Recommendations#
Choose Gonadorelin When:#
- Diagnostic evaluation of pituitary gonadotroph function is needed
- HPG axis stimulation and support of endogenous LH/FSH is the goal
- Fertility treatment requires pulsatile GnRH replacement for hypothalamic amenorrhea
- Axis preservation is important and sustained suppression must be avoided
- Short-term intervention with minimal hormonal disruption is preferred
Choose Triptorelin When:#
- Hormone suppression is the therapeutic goal (prostate cancer, endometriosis, fibroids)
- Chemical castration is needed as part of oncological treatment
- Central precocious puberty requires pubertal arrest
- Long-acting depot convenience is preferred over daily or pulsatile dosing
- Fertility preservation during gonadotoxic chemotherapy is the context
Can They Be Combined?#
Combining gonadorelin and triptorelin would be pharmacologically contradictory. Gonadorelin stimulates the axis that triptorelin is designed to suppress. In practice, however, a sequential approach has clinical rationale: gonadorelin can be used diagnostically to assess pituitary function before initiating triptorelin for suppression, or after triptorelin discontinuation to evaluate axis recovery.
In fertility protocols, the sequential use of GnRH agonist suppression (using triptorelin or similar agents) followed by pulsatile GnRH stimulation is an established reproductive endocrinology strategy, though typically the suppression and stimulation phases use different GnRH analogs.
For related reproductive peptides, see our profiles on HCG, kisspeptin, and HMG, which offer complementary approaches to HPG axis modulation.
Verdict#
Gonadorelin and triptorelin are not alternatives to each other but rather tools for opposite clinical objectives. Gonadorelin supports the HPG axis by providing the physiological signal that drives LH and FSH release, making it indispensable for diagnostic testing and fertility applications. Triptorelin exploits the paradox of continuous agonism to suppress the same axis, providing chemical castration for hormone-dependent cancers, endometriosis, and other conditions requiring hormone deprivation.
Triptorelin has the broader clinical footprint with four FDA-approved indications and the practical advantage of depot formulations lasting up to 6 months. Gonadorelin has the narrower but irreplaceable role of stimulating and assessing pituitary function. The "better" peptide is entirely determined by whether the clinical goal is to turn the HPG axis on or off.
For a broader perspective on reproductive peptides, explore our profiles on HCG and kisspeptin, or use the half-life comparison tool to visualize the pharmacokinetic differences between short-acting and depot formulations.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Pituitary function diagnostic testing
Gonadorelin
FDA-approved for evaluating pituitary gonadotroph function; acute LH/FSH stimulation test with rapid assessment
Advanced prostate cancer treatment
Triptorelin
FDA-approved for androgen deprivation therapy with depot formulations providing months of sustained castrate testosterone levels
Fertility support and HPG axis stimulation
Gonadorelin
Stimulates endogenous LH/FSH release to support gonadal function; used in pulsatile protocols for hypothalamic amenorrhea
Endometriosis or uterine fibroid management
Triptorelin
Suppresses estrogen to menopausal levels, reducing endometriotic lesion activity and fibroid volume
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Gonadorelin vs Triptorelin: Native GnRH vs Long-Acting Agonist
Which is better, Gonadorelin or Triptorelin?
Gonadorelin and triptorelin produce opposite clinical outcomes despite targeting the same receptor. Gonadorelin stimulates LH/FSH release and supports the HPG axis, making it essential for diagnostic testing and fertility applications. Triptorelin suppresses the axis through sustained receptor desensitization, providing chemical castration for hormone- dependent conditions. The choice is entirely determined by the clinical goal: stimulation and axis support (gonadorelin) versus suppression an... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Gonadorelin and Triptorelin?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to Triptorelin; Side Effect Profile: advantage goes to Gonadorelin. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Gonadorelin over Triptorelin?
For the scenario of "Pituitary function diagnostic testing," research data suggests Gonadorelin may be more relevant. FDA-approved for evaluating pituitary gonadotroph function; acute LH/FSH stimulation test with rapid assessment. This is based on currently available evidence and individual circumstances may differ.
How do Gonadorelin and Triptorelin differ in their mechanisms of action?
Gonadorelin: Synthetic decapeptide identical to native GnRH; stimulates pulsatile LH and FSH release from anterior pituitary gonadotrophs via Gq/11-PLC-Ca2+ signaling; short half-life maintains physiological si.... Triptorelin: GnRH agonist with D-Trp6 substitution conferring metabolic stability; initial stimulatory flare followed by pituitary desensitization and gonadotropin suppression; produces chemical castration with....
Which has fewer side effects, Gonadorelin or Triptorelin?
In terms of side effects and tolerability, the advantage goes to Gonadorelin. Gonadorelin: Generally well-tolerated; transient headache, nausea, and flushing; minimal systemic effects due to short half-life; does not cause sustained hormo.... Triptorelin: Initial testosterone/estrogen flare (1-2 weeks); sustained castrate hormone levels with hot flashes, bone density loss, sexual dysfunction, and met....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.