HGH 191AA vs HGH Fragment 176-191: Growth Hormone Compared
HGH 191AA vs HGH Fragment 176-191 compared: full growth hormone vs fat-loss fragment — mechanisms, body composition, and side effects.
Verdict at a Glance
HGH 191AA is the clear choice when comprehensive growth hormone effects are needed, offering FDA-approved efficacy across growth, metabolism, and body composition. HGH Fragment 176-191 fills a narrower niche for researchers interested in isolated fat-loss mechanisms without the broader hormonal effects and side-effect burden of full-length GH. The fragment's limited clinical validation means it remains primarily a research tool, while HGH 191AA has a well-established therapeutic role.
| Best for | Pick | Why |
|---|---|---|
| Growth hormone deficiency treatment | HGH 191AA | FDA-approved for GH deficiency with proven efficacy for growth, body composition, and metabolic outcomes |
| Targeted fat loss research without anabolic effects | HGH Fragment 176-191 | Selective lipolytic action without IGF-1 elevation, insulin resistance, or growth-promoting effects |
| Anti-aging and body composition optimization | HGH 191AA | Comprehensive effects on lean mass, bone density, skin quality, and fat reduction supported by clinical evidence |
| Metabolic research with minimal hormonal disruption | HGH Fragment 176-191 | Does not activate the GH receptor or alter glucose homeostasis, allowing isolated study of lipolytic pathways |
| Category | HGH 191AA | HGH Fragment 176-191 | Advantage |
|---|---|---|---|
| Mechanism of Action | Full 191-amino acid somatotropin that binds the GH receptor and activates JAK2-STAT5, ERK, and PI3K/AKT pathways; drives IGF-1 production, growth, lipolysis, and anabolic signaling across multiple tissues | 16-amino acid C-terminal fragment of GH that does not bind the GH receptor; selectively promotes lipolysis and inhibits lipogenesis via beta-3 adrenergic and HSL/ACC pathways without growth or IGF-1 effects | HGH 191AA |
| Research Evidence | FDA-approved for multiple indications with decades of Phase 3 RCTs; extensive safety and efficacy data across pediatric and adult populations | Phase 2 clinical data as AOD-9604; preclinical evidence for selective lipolysis; limited human efficacy data and no regulatory approvals for injectable form | HGH 191AA |
| Side Effect Profile | Well-characterized but significant side effects including edema, joint pain, carpal tunnel syndrome, insulin resistance, and potential tumor growth risk with long-term use | Minimal reported side effects; does not cause hyperglycemia or insulin resistance; no IGF-1 elevation; limited long-term safety data | HGH Fragment 176-191 |
| Dosing Complexity | Daily subcutaneous injection with dose titration based on IGF-1 levels; requires medical monitoring for glucose, IGF-1, and growth markers | Subcutaneous injection typically administered 1-2 times daily; simpler monitoring with fewer metabolic parameters to track | HGH Fragment 176-191 |
| Body Composition Effects | Comprehensive body composition changes including fat loss, lean mass gain, bone density improvement, and enhanced protein synthesis; affects virtually every tissue | Targeted fat loss without anabolic effects on muscle or bone; does not increase lean mass or affect growth parameters; isolated lipolytic action | HGH 191AA |

Introduction#
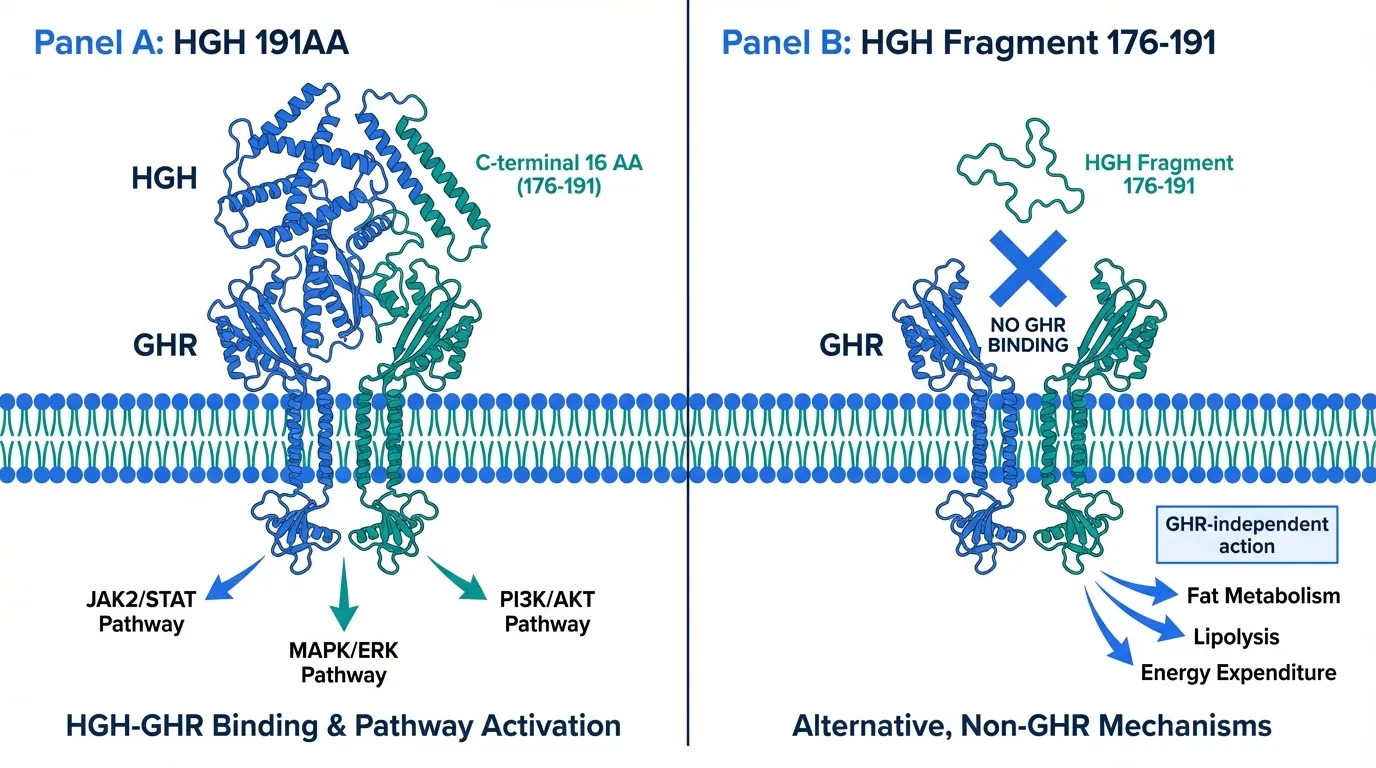
HGH 191AA and HGH Fragment 176-191 share a direct structural relationship: the fragment is literally the last 16 amino acids of the full 191-amino acid growth hormone protein. Yet they represent fundamentally different pharmacological approaches. Full-length HGH 191AA binds the growth hormone receptor and activates the full spectrum of GH signaling, producing effects on growth, metabolism, body composition, and organ function. The fragment, by contrast, retains only the lipolytic activity encoded in the C-terminal region while lacking the ability to activate GH receptor signaling.
This comparison examines when the comprehensive effects of full-length growth hormone are warranted versus when the targeted, narrower action of the fat-loss fragment may be more appropriate for research or clinical contexts.
Quick Comparison#
| Feature | HGH 191AA | HGH Fragment 176-191 |
|---|---|---|
| Structure | 191 amino acids, 22.1 kDa | 16 amino acids, 1.8 kDa |
| Receptor | GH receptor (GHR) | Does not bind GHR |
| Primary Action | Full GH signaling cascade | Selective lipolysis |
| IGF-1 Effects | Increases systemic IGF-1 | No effect on IGF-1 |
| Regulatory Status | FDA-approved | Phase 2 (as AOD-9604) |
| Research Status | Approved | Phase 2 |
| Insulin Sensitivity | May decrease (higher doses) | Does not impair |
| Growth Effects | Promotes linear growth, organ growth | None |
| Half-Life | ~3-4 hours | ~30 minutes |
Mechanism of Action Comparison#
HGH 191AA#
HGH 191AA is identical to endogenous pituitary-derived somatotropin. It binds the growth hormone receptor (GHR), a class I cytokine receptor present as a preformed homodimer on target cells throughout the body. A single GH molecule engages two receptor subunits asymmetrically through site 1 and site 2 binding, producing a rotational realignment that activates intracellular signaling.
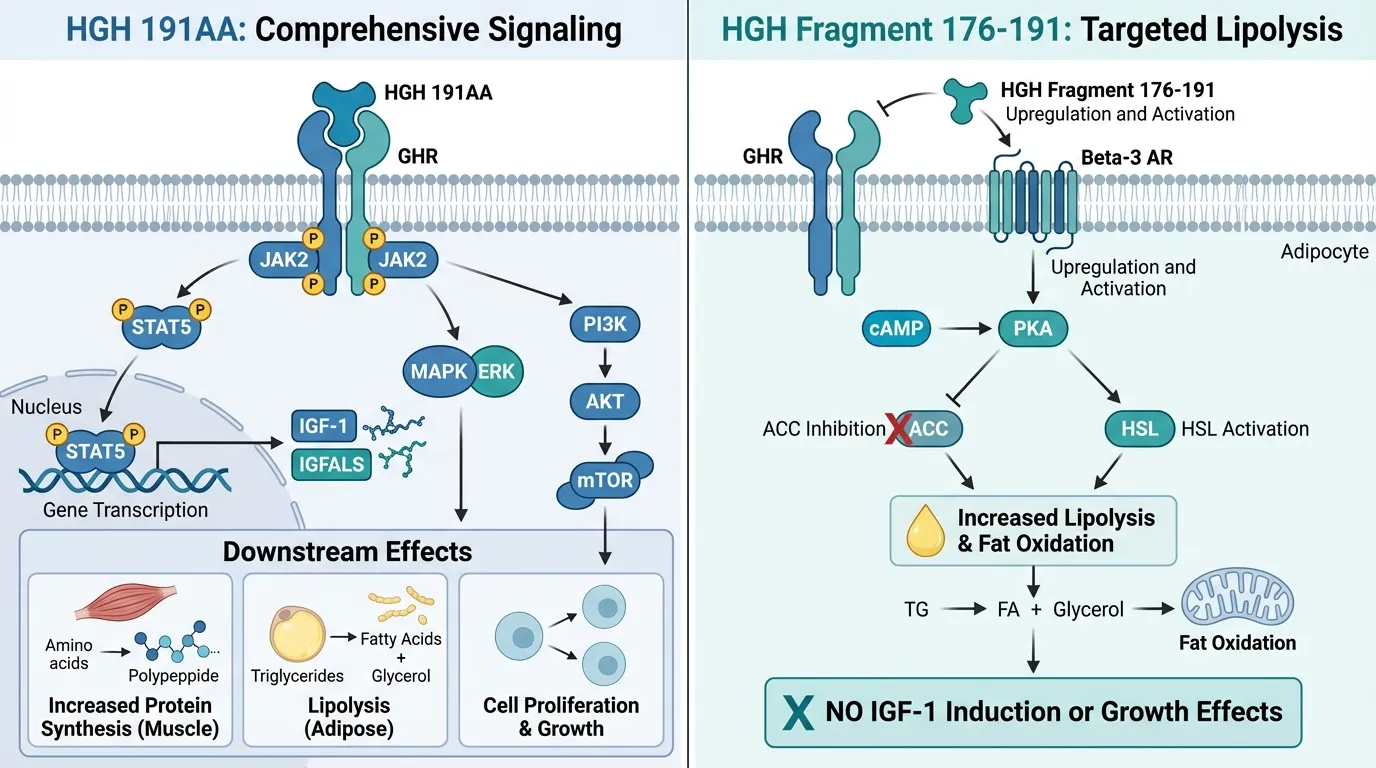
The primary downstream pathway involves JAK2 trans-phosphorylation and subsequent activation of STAT5a/b, which drives transcription of key targets including hepatic IGF-1, IGFALS, and feedback regulators CISH and SOCS2. GH also activates the MAPK/ERK pathway through Shc recruitment, the PI3K/AKT/mTOR pathway through IRS adaptors, and Src family kinases through a JAK2-independent branch.
These signaling cascades produce tissue-specific effects: hepatic IGF-1 production for endocrine growth signaling, muscle protein synthesis and glucose uptake, adipose tissue lipolysis, bone formation, and immune cell modulation. The breadth of GH action is a defining characteristic, distinguishing it from targeted peptide fragments.
HGH Fragment 176-191#
HGH Fragment 176-191 corresponds to amino acids 176-191 of the growth hormone protein. Critically, this fragment does not bind or activate the canonical GH receptor. Radioligand competition studies show no displacement of labeled GH by the fragment, and GHR-dependent proliferation assays confirm absence of receptor-mediated signaling.
Instead, the fragment appears to promote fat metabolism through GHR-independent pathways. The proposed mechanisms include upregulation of beta-3 adrenergic receptors in adipose tissue, activation of the cAMP-PKA lipolytic cascade through enhanced catecholamine sensitivity, direct or indirect inhibition of acetyl-CoA carboxylase (ACC) reducing de novo lipogenesis by approximately 43-57% in vitro, and activation of hormone-sensitive lipase (HSL) with increased glycerol release.
The absence of GHR activation means no JAK-STAT signaling, no IGF-1 induction, no insulin resistance, and no growth-promoting effects. This selectivity defines the fragment's pharmacological niche.
Evidence and Research Comparison#
HGH 191AA Research#
HGH 191AA has one of the most extensive clinical evidence bases of any peptide. Key milestones include:
- Growth hormone deficiency: Multiple Phase 3 RCTs demonstrating efficacy for linear growth in GH-deficient children, with catch-up growth velocities of 10-12 cm/year in the first treatment year
- Adult GH deficiency: Controlled trials showing improved body composition (reduced visceral fat, increased lean mass), bone mineral density, and quality of life
- Turner syndrome: FDA-approved indication with documented growth velocity improvement
- AIDS wasting: Approved for HIV-associated wasting syndrome, demonstrating lean mass preservation
- Chronic renal insufficiency: Approved for growth failure in pediatric CKD patients
The safety database spans decades of post-marketing surveillance across millions of patient-years, providing detailed understanding of both short-term and long-term risks.
HGH Fragment 176-191 Research#
The fragment has been studied primarily as AOD-9604 (an analog with improved stability):
- Preclinical models: Demonstrated selective fat loss in obese rodent models with 2-3 fold increases in fat oxidation, reduction in adiposity, and glycemic neutrality
- Phase 2 clinical trial: AOD-9604 was tested in obese adults but did not demonstrate statistically significant weight loss compared to placebo in the primary endpoint analysis
- Mechanism studies: In vitro data confirm ACC inhibition, HSL activation, and absence of GHR binding
- Oral formulation: Some studies have explored oral delivery of AOD-9604, representing a departure from the injectable route typical of peptide therapeutics
The clinical evidence base is significantly thinner than that of full-length GH, and no regulatory approvals have been granted for the injectable peptide fragment in any major market.
Side Effects and Safety Comparison#
HGH 191AA Side Effects#
Full-length growth hormone carries a well-characterized side effect profile reflecting its broad biological activity:
- Common: Fluid retention and edema, arthralgia and myalgia, carpal tunnel syndrome, headache
- Metabolic: Insulin resistance and impaired glucose tolerance at higher doses, potential progression to diabetes in predisposed individuals
- Growth-related: Theoretical concern for accelerating pre-existing malignancies via IGF-1 elevation (though observational data remain debated)
- Endocrine: Suppression of endogenous GH secretion, potential hypothyroidism, altered cortisol metabolism
- Long-term: Acromegalic features with chronic supraphysiological dosing, including frontal bossing, jaw enlargement, and visceral organ growth
Monitoring requirements include IGF-1 levels, fasting glucose, HbA1c, and periodic cancer screening.
HGH Fragment 176-191 Side Effects#
The fragment's selectivity results in a more favorable side effect profile:
- Metabolic: Does not impair insulin sensitivity or glucose tolerance in studied models
- Hormonal: No IGF-1 elevation, no suppression of endogenous GH axis
- Growth: No growth-promoting effects, eliminating concerns about tumor promotion
- Reported: Mild injection site reactions and occasional headache in clinical studies
- Limitation: Long-term safety data are limited due to smaller study populations and shorter follow-up periods
The absence of GHR activation eliminates the majority of GH-related side effects, though the limited clinical experience means rare adverse effects cannot be ruled out.
Dosing and Administration Comparison#
HGH 191AA Dosing#
| Parameter | Details |
|---|---|
| Route | Subcutaneous injection |
| GH deficiency (pediatric) | 0.025-0.05 mg/kg/day |
| GH deficiency (adult) | 0.2-0.5 mg/day, titrated to IGF-1 |
| Administration | Daily, typically at bedtime |
| Monitoring | IGF-1, glucose, thyroid function |
| Storage | Refrigerated (2-8 C) |
HGH Fragment 176-191 Dosing#
| Parameter | Details |
|---|---|
| Route | Subcutaneous injection |
| Research doses | 250-500 mcg per administration |
| Frequency | 1-2 times daily in research protocols |
| Timing | Often studied on an empty stomach |
| Monitoring | Fewer parameters required |
| Storage | Refrigerated after reconstitution |
The fragment requires less complex monitoring since it does not affect IGF-1 levels, glucose homeostasis, or growth parameters.
Use Case Recommendations#
Choose HGH 191AA When:#
- Diagnosed GH deficiency requiring comprehensive hormone replacement
- Growth failure in pediatric patients with documented GH deficiency
- Body composition goals requiring both fat loss and lean mass gain
- Bone health is a treatment priority alongside metabolic optimization
- Clinical setting with proper medical oversight and monitoring capability
Choose HGH Fragment 176-191 When:#
- Isolated fat-loss research is the objective without desire for anabolic effects
- Insulin sensitivity must be preserved and cannot tolerate GH-induced resistance
- IGF-1 elevation is contraindicated or undesirable
- Research context studying GHR-independent lipolytic mechanisms
- Simpler monitoring is preferred without the need for IGF-1 tracking
Can They Be Combined?#
Combining full-length GH with its own fragment would be pharmacologically redundant. HGH 191AA already contains the amino acid sequence of the fragment and activates both GHR-dependent and the fragment's GHR-independent pathways. The fragment would not add meaningful lipolytic activity beyond what full-length GH already provides.
For researchers seeking enhanced fat loss alongside GH therapy, the more common approach is to combine GH with GH-releasing peptides such as ipamorelin or GHRH analogs like sermorelin or tesamorelin, which amplify endogenous GH pulsatility rather than providing a redundant fragment.
Verdict#
HGH 191AA and HGH Fragment 176-191 are not truly competing options for the same indication. Full-length HGH 191AA is an FDA-approved hormone with comprehensive effects on growth, metabolism, and body composition, backed by one of the largest clinical evidence bases in endocrinology. HGH Fragment 176-191 is a research-stage peptide that isolates one specific activity of GH (lipolysis) while eliminating the rest.
The choice depends entirely on the objective: when the full spectrum of growth hormone effects is needed, HGH 191AA is the established standard. When isolated fat metabolism research is the goal without hormonal complexity, the fragment offers a more targeted tool. However, the fragment's limited clinical validation means it remains primarily in the research domain rather than as a validated therapeutic option.
For those exploring GH-axis peptides, our dosing calculator can help estimate weight-based dosing parameters, and our guides to related peptides including sermorelin and tesamorelin provide context on alternative approaches to GH augmentation.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Growth hormone deficiency treatment
HGH 191AA
FDA-approved for GH deficiency with proven efficacy for growth, body composition, and metabolic outcomes
Targeted fat loss research without anabolic effects
HGH Fragment 176-191
Selective lipolytic action without IGF-1 elevation, insulin resistance, or growth-promoting effects
Anti-aging and body composition optimization
HGH 191AA
Comprehensive effects on lean mass, bone density, skin quality, and fat reduction supported by clinical evidence
Metabolic research with minimal hormonal disruption
HGH Fragment 176-191
Does not activate the GH receptor or alter glucose homeostasis, allowing isolated study of lipolytic pathways
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About HGH 191AA vs HGH Fragment 176-191: Growth Hormone Compared
Which is better, HGH 191AA or HGH Fragment 176-191?
HGH 191AA is the clear choice when comprehensive growth hormone effects are needed, offering FDA-approved efficacy across growth, metabolism, and body composition. HGH Fragment 176-191 fills a narrower niche for researchers interested in isolated fat-loss mechanisms without the broader hormonal effects and side-effect burden of full-length GH. The fragment's limited clinical validation means it remains primarily a research tool, while HGH 191AA has a well-established therapeutic role. Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between HGH 191AA and HGH Fragment 176-191?
The main differences across comparison categories are: Mechanism of Action: advantage goes to HGH 191AA; Research Evidence: advantage goes to HGH 191AA; Side Effect Profile: advantage goes to HGH Fragment 176-191. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider HGH 191AA over HGH Fragment 176-191?
For the scenario of "Growth hormone deficiency treatment," research data suggests HGH 191AA may be more relevant. FDA-approved for GH deficiency with proven efficacy for growth, body composition, and metabolic outcomes. This is based on currently available evidence and individual circumstances may differ.
How do HGH 191AA and HGH Fragment 176-191 differ in their mechanisms of action?
HGH 191AA: Full 191-amino acid somatotropin that binds the GH receptor and activates JAK2-STAT5, ERK, and PI3K/AKT pathways; drives IGF-1 production, growth, lipolysis, and anabolic signaling across multiple .... HGH Fragment 176-191: 16-amino acid C-terminal fragment of GH that does not bind the GH receptor; selectively promotes lipolysis and inhibits lipogenesis via beta-3 adrenergic and HSL/ACC pathways without growth or IGF-....
Which has fewer side effects, HGH 191AA or HGH Fragment 176-191?
In terms of side effects and tolerability, the advantage goes to HGH Fragment 176-191. HGH 191AA: Well-characterized but significant side effects including edema, joint pain, carpal tunnel syndrome, insulin resistance, and potential tumor growth.... HGH Fragment 176-191: Minimal reported side effects; does not cause hyperglycemia or insulin resistance; no IGF-1 elevation; limited long-term safety data.
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.