Carnosine vs Glutathione: Endogenous Antioxidant Peptides Compared
Comparison of carnosine and glutathione, two naturally occurring antioxidant peptides with distinct mechanisms, bioavailability profiles, and therapeutic applications for oxidative stress and aging.
Verdict at a Glance
Glutathione has the stronger clinical evidence base and the more fundamental biological role as the body's primary intracellular antioxidant and redox regulator. Carnosine has a more specialized niche in anti-glycation and muscle pH buffering. For general antioxidant support and detoxification, glutathione (or its precursor NAC) is the more evidence-based choice. For targeted anti-glycation, exercise buffering, or diabetic complications, carnosine (or its precursor beta-alanine) fills a unique role that glutathione does not. Both are endogenous peptides with excellent safety profiles.
| Best for | Pick | Why |
|---|---|---|
| General Antioxidant Support | Glutathione | Glutathione is the body's master antioxidant with the most extensive evidence for broad oxidative stress reduction. IV glutathione or oral NAC supplementation effectively raises intracellular GSH levels. |
| Anti-Glycation and AGE Prevention | Carnosine | Carnosine is a potent anti-glycation agent that directly inhibits AGE formation by competing with sugars for protein binding sites. Glutathione does not share this specific mechanism. |
| Exercise Performance | Carnosine | Beta-alanine supplementation raises muscle carnosine, which buffers intracellular pH during high-intensity exercise. This is one of the most well-validated ergogenic supplement strategies, supported by multiple meta-analyses. |
| Liver Health and Detoxification | Glutathione | Glutathione is central to hepatic detoxification via glutathione S-transferase conjugation reactions. Clinical data supports its use in NAFLD, and N-acetyl cysteine is the standard treatment for acetaminophen overdose specifically because it replenishes liver GSH. |
| Diabetic Complications | Carnosine | The anti-glycation properties of carnosine are particularly relevant for diabetic complications, where AGE accumulation drives retinopathy, nephropathy, and neuropathy. Carnosine directly targets this pathogenic mechanism. |
| Category | Carnosine | Glutathione | Advantage |
|---|---|---|---|
| Mechanism of Action | Dipeptide (beta-alanine + histidine) with primary anti-glycation activity. Inhibits formation of advanced glycation end products (AGEs) by competing with sugars to bind proteins. Also provides pH buffering in muscle, metal chelation, and moderate direct antioxidant activity. Concentrated in skeletal muscle and brain tissue. | Tripeptide (glutamate + cysteine + glycine) serving as the body's master intracellular antioxidant. Directly neutralizes reactive oxygen species via its thiol group. Functions as a cofactor for glutathione peroxidase enzymes. Maintains redox homeostasis, supports detoxification, and regenerates other antioxidants (vitamins C and E). | Comparable |
| Research Evidence | Moderate preclinical evidence for anti-glycation and neuroprotection. Very limited human trial data. Primarily studied in vitro for AGE inhibition and in animal models for diabetes, neurodegeneration, and exercise performance (via beta-alanine supplementation). | Extensive research spanning decades. Human clinical data in chemotherapy-induced neuropathy, HIV/AIDS immune support, liver disease (NAFLD), and respiratory conditions. Well-established biochemistry. Supplementation evidence is limited by poor oral bioavailability, though IV glutathione and NAC precursor studies are more robust. | Glutathione |
| Bioavailability | Oral carnosine is rapidly hydrolyzed by carnosinase in plasma, limiting systemic bioavailability. Beta-alanine supplementation (the rate-limiting precursor) effectively increases muscle and brain carnosine levels. Oral carnosine itself has limited tissue delivery outside the GI tract. | Oral glutathione has poor bioavailability due to peptidase degradation in the GI tract and lack of a specific cell membrane transporter. Liposomal glutathione and IV glutathione provide better delivery. NAC (N-acetyl cysteine) is the most effective oral strategy for raising intracellular GSH levels. | Comparable |
| Practical Supplementation | Most commonly supplemented as beta-alanine (1.6-6.4 g daily), which reliably increases muscle carnosine. Direct carnosine supplements (500-2000 mg) are available but less well-validated for tissue levels. Beta-alanine causes harmless paresthesia (tingling) at higher doses. Widely available and inexpensive. | Multiple delivery routes available. IV glutathione (600-2400 mg) provides direct systemic delivery. Liposomal oral glutathione improves bioavailability over standard oral. NAC (600-1800 mg daily) is the most practical oral precursor strategy. Widely available in multiple formulations. | Comparable |

Introduction#
Carnosine and glutathione are both naturally occurring peptides that serve protective roles in the body, but they operate through fundamentally different mechanisms and occupy distinct biological niches. Glutathione (GSH) is often called the "master antioxidant" -- a tripeptide that serves as the primary intracellular defense against oxidative stress in virtually every cell. Carnosine is a dipeptide concentrated in muscle and brain tissue that excels at preventing glycation damage and buffering intracellular pH.
Both decline with age, and both have been investigated as supplements for aging-related conditions. However, their mechanisms are complementary rather than overlapping, and the choice between them depends on the specific biological target. This comparison examines their mechanisms, evidence bases, and practical supplementation strategies.
Mechanism of Action Comparison#
Carnosine#
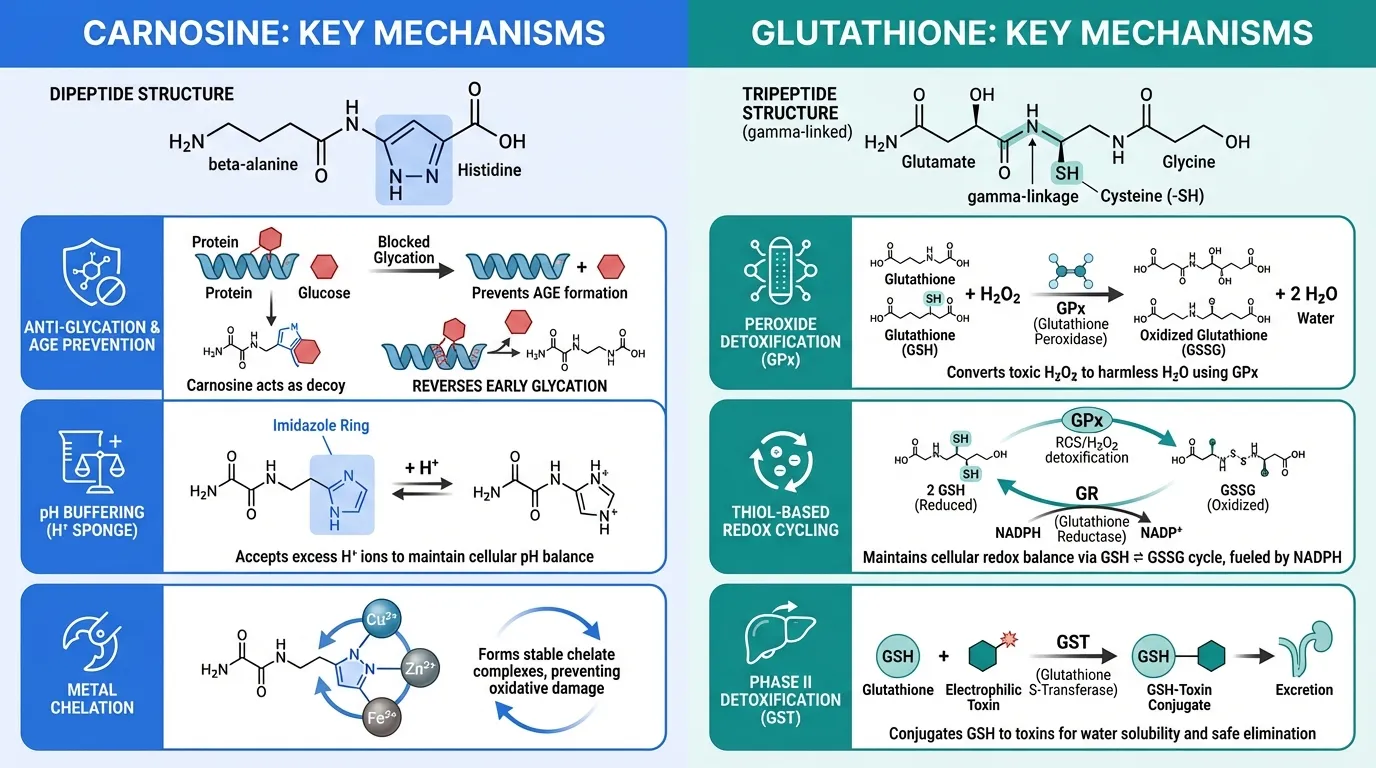
Carnosine (beta-alanyl-L-histidine) is a dipeptide synthesized from beta-alanine and histidine by carnosine synthase. It is found at high concentrations (up to 20 mM) in skeletal muscle and in lower concentrations in the brain, heart, and other tissues. Its key mechanisms include:
- Anti-glycation: Carnosine competes with sugars to bind proteins, preventing the formation of advanced glycation end products (AGEs). It can also "carnosinylate" already-glycated proteins through a trans-glycation reaction, potentially reversing early glycation damage
- pH buffering: The imidazole ring of histidine in carnosine has a pKa near physiological pH, making carnosine an effective intracellular buffer during high-intensity exercise when lactic acid accumulates
- Metal chelation: Chelates transition metals (copper, zinc, iron) that would otherwise catalyze oxidative reactions
- Direct antioxidant activity: Scavenges reactive oxygen species and reactive carbonyl species, though this activity is relatively modest compared to glutathione
- Aldehyde quenching: Reacts with and neutralizes toxic aldehydes produced during lipid peroxidation
Glutathione#
Glutathione (gamma-L-glutamyl-L-cysteinyl-glycine) is a tripeptide with a unique gamma peptide linkage that makes it resistant to most cellular peptidases. It exists in reduced (GSH) and oxidized (GSSG) forms, with GSH comprising over 98% of total intracellular glutathione at concentrations of 0.5-10 mM. Its mechanisms include:
- Peroxide detoxification: Serves as the electron donor for glutathione peroxidase enzymes (GPx), which convert hydrogen peroxide and lipid hydroperoxides to water and alcohols
- Thiol-based redox cycling: The cysteine thiol group (–SH) directly reduces oxidizing species. Oxidized GSSG is recycled back to GSH by glutathione reductase using NADPH
- Phase II detoxification: Glutathione S-transferase (GST) enzymes conjugate GSH to electrophilic toxins, drugs, and carcinogens for excretion
- Antioxidant recycling: Regenerates oxidized vitamin C (dehydroascorbate back to ascorbate) and vitamin E
- Protein thiol maintenance: Maintains cysteine residues in proteins in their reduced, functional state (protein S-glutathionylation)
- Immune function: Critical for T-cell proliferation and function; GSH depletion impairs immune responses
Mechanistic Comparison#
| Feature | Carnosine | Glutathione |
|---|---|---|
| Structure | Dipeptide (beta-alanine + histidine) | Tripeptide (glutamate + cysteine + glycine) |
| Primary mechanism | Anti-glycation, pH buffering | Redox cycling, peroxide detoxification |
| Tissue distribution | Muscle, brain (high concentrations) | All cells (ubiquitous) |
| Intracellular concentration | Up to 20 mM (muscle) | 0.5-10 mM |
| Direct antioxidant | Moderate | Strong (thiol-based) |
| Enzymatic systems | None | GPx, GST, GR (glutathione reductase) |
| Metal chelation | Yes (Cu, Zn, Fe) | Limited |
| Detoxification role | Aldehyde quenching | Phase II conjugation |
Dosing Comparison#
Carnosine Dosing#
Carnosine supplementation can be approached directly or through its precursor:
- Beta-alanine (precursor): 1.6-6.4 g daily, typically divided into multiple doses. This is the most effective strategy for raising muscle carnosine levels (increases of 40-80% documented over 4-12 weeks)
- Direct carnosine: 500-2000 mg daily oral supplementation. Rapidly hydrolyzed by serum carnosinase (CN1), limiting systemic bioavailability
- Sustained-release beta-alanine: Reduces paresthesia side effect while maintaining efficacy
- L-carnosine eye drops: N-acetylcarnosine eye drops studied for cataracts (topical application avoids carnosinase issue)
Glutathione Dosing#
Multiple delivery strategies exist to address bioavailability challenges:
- IV glutathione: 600-2400 mg infusion, typically 1-3 times weekly. Provides direct systemic delivery
- Liposomal oral glutathione: 250-1000 mg daily. Liposomal encapsulation improves absorption
- Standard oral glutathione: 250-1000 mg daily, but most evidence suggests poor absorption due to GI peptidase degradation
- NAC (precursor): 600-1800 mg daily oral. Provides cysteine (the rate-limiting amino acid for GSH synthesis) and is the most cost-effective oral strategy
- Nebulized glutathione: Used in some respiratory conditions (600 mg in nebulizer solution)
Side Effects Comparison#
Carnosine Side Effects#
Carnosine and beta-alanine are well tolerated:
- Paresthesia (beta-alanine): Harmless tingling sensation in face, hands, and chest at doses above ~800 mg. Dose-dependent, resolves within 60-90 minutes. Avoided with sustained-release formulations or divided dosing
- GI effects: Mild nausea at high doses of direct carnosine supplementation
- No serious adverse effects: Extensive supplement use history with no significant safety signals
- Drug interactions: None well documented
Glutathione Side Effects#
Glutathione is also well tolerated across delivery routes:
- IV glutathione: Mild cramping, bloating, or allergic reactions (rare). Transient flushing
- Oral glutathione/NAC: GI discomfort (nausea, diarrhea) at higher doses. NAC has a sulfur taste/smell
- Nebulized glutathione: May cause bronchospasm in some individuals with reactive airway disease
- Skin lightening: Long-term glutathione use has been associated with skin depigmentation (melanin synthesis inhibition), which is intentional in some markets but an unwanted effect in others
- NAC caution: Very high doses of NAC can theoretically act as a pro-oxidant; standard doses are safe
Research Evidence Comparison#
Carnosine Research#
- Anti-glycation (in vitro): Potent inhibition of AGE formation confirmed in multiple in vitro systems. Carnosine is one of the most effective biological anti-glycation agents identified
- Exercise performance (beta-alanine): Strong evidence from multiple meta-analyses that beta-alanine supplementation improves high-intensity exercise performance lasting 1-4 minutes
- Diabetes (preclinical): Animal studies show reduced diabetic complications (nephropathy, retinopathy) with carnosine supplementation
- Neuroprotection (preclinical): Protective effects in animal models of ischemic stroke and neurodegenerative disease
- Human supplementation trials: Limited. One RCT in diabetic patients showed improvements in some inflammatory markers. One trial in autism showed no effect on AGE markers
Evidence level: Low to moderate -- strong in vitro and preclinical data, but limited human clinical trials for direct carnosine effects. Beta-alanine for exercise performance has moderate-to-strong evidence.
Glutathione Research#
- Chemotherapy neuropathy: Randomized study showed IV glutathione (1500 mg/m2) before oxaliplatin significantly reduced neurotoxicity (58% vs 10% in placebo)
- HIV/AIDS: Liposomal glutathione supplementation improved Th1 cytokine profiles and immune function in HIV patients
- NAFLD/liver disease: Clinical data supports glutathione supplementation for non-alcoholic fatty liver disease
- Respiratory conditions: Nebulized and intratracheal glutathione reduced lung disease risk in preterm infants
- Acetaminophen toxicity: NAC (glutathione precursor) is the standard of care for acetaminophen overdose, directly demonstrating the clinical importance of hepatic GSH
- Skin lightening: Multiple clinical trials confirm glutathione (oral and IV) reduces melanin production, though with variable results
Evidence level: Moderate -- multiple human clinical trials across indications, though many are small. NAC has strong evidence as a precursor strategy.
Key Differences Summary#
- Primary role: Carnosine is an anti-glycation agent and muscle buffer. Glutathione is the master intracellular antioxidant and detoxifier.
- Tissue distribution: Carnosine is concentrated in muscle and brain. Glutathione is ubiquitous in all cells.
- Enzymatic systems: Glutathione feeds into GPx, GST, and GR enzyme families. Carnosine has no dedicated enzymatic pathway.
- Clinical evidence: Glutathione has more human interventional data (chemotherapy protection, immune support, liver disease). Carnosine's strongest human evidence is indirect, through beta-alanine for exercise.
- Supplementation strategy: Both suffer from oral bioavailability challenges. Beta-alanine is the practical solution for carnosine; NAC is the practical solution for glutathione.
- Unique capabilities: Carnosine's anti-glycation and pH buffering are not shared by glutathione. Glutathione's peroxide detoxification and phase II conjugation are not shared by carnosine.
- Safety: Both have excellent safety profiles as endogenous peptides with long supplement use histories.
Conclusion#
Carnosine and glutathione are genuinely complementary antioxidant peptides that address different aspects of cellular damage. Glutathione is the more fundamental molecule -- the body's primary defense against oxidative stress, with clinical evidence spanning chemotherapy protection, immune support, and liver health. For broad antioxidant support, glutathione (or its precursor NAC) has the stronger evidence base and the more critical biological role.
Carnosine fills a specialized niche that glutathione cannot: anti-glycation. The formation of AGEs is a distinct pathological process from oxidative stress, and carnosine is one of the few endogenous molecules that directly inhibits it. For conditions driven by glycation (diabetic complications, some aspects of aging), carnosine is the more targeted choice. Additionally, beta-alanine supplementation for exercise performance is one of the better-validated ergogenic strategies available.
For comprehensive cellular protection, both peptides address different vulnerabilities -- oxidative damage (glutathione) and glycation damage (carnosine) -- and supplementing both through practical precursor strategies (NAC + beta-alanine) is a well-tolerated, evidence-informed approach.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
General Antioxidant Support
Glutathione
Glutathione is the body's master antioxidant with the most extensive evidence for broad oxidative stress reduction. IV glutathione or oral NAC supplementation effectively raises intracellular GSH levels.
Anti-Glycation and AGE Prevention
Carnosine
Carnosine is a potent anti-glycation agent that directly inhibits AGE formation by competing with sugars for protein binding sites. Glutathione does not share this specific mechanism.
Exercise Performance
Carnosine
Beta-alanine supplementation raises muscle carnosine, which buffers intracellular pH during high-intensity exercise. This is one of the most well-validated ergogenic supplement strategies, supported by multiple meta-analyses.
Liver Health and Detoxification
Glutathione
Glutathione is central to hepatic detoxification via glutathione S-transferase conjugation reactions. Clinical data supports its use in NAFLD, and N-acetyl cysteine is the standard treatment for acetaminophen overdose specifically because it replenishes liver GSH.
Diabetic Complications
Carnosine
The anti-glycation properties of carnosine are particularly relevant for diabetic complications, where AGE accumulation drives retinopathy, nephropathy, and neuropathy. Carnosine directly targets this pathogenic mechanism.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Carnosine vs Glutathione: Endogenous Antioxidant Peptides Compared
Which is better, Carnosine or Glutathione?
Glutathione has the stronger clinical evidence base and the more fundamental biological role as the body's primary intracellular antioxidant and redox regulator. Carnosine has a more specialized niche in anti-glycation and muscle pH buffering. For general antioxidant support and detoxification, glutathione (or its precursor NAC) is the more evidence-based choice. For targeted anti-glycation, exercise buffering, or diabetic complications, carnosine (or its precursor beta-alanine) fills a uniqu... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Carnosine and Glutathione?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to Glutathione; Bioavailability: advantage goes to neither (tie). 1 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Glutathione over Carnosine?
For the scenario of "General Antioxidant Support," research data suggests Glutathione may be more relevant. Glutathione is the body's master antioxidant with the most extensive evidence for broad oxidative stress reduction. IV glutathione or oral NAC supplementation effectively raises intracellular GSH l.... This is based on currently available evidence and individual circumstances may differ.
How do Carnosine and Glutathione differ in their mechanisms of action?
Carnosine: Dipeptide (beta-alanine + histidine) with primary anti-glycation activity. Inhibits formation of advanced glycation end products (AGEs) by competing with sugars to bind proteins. Also provides pH b.... Glutathione: Tripeptide (glutamate + cysteine + glycine) serving as the body's master intracellular antioxidant. Directly neutralizes reactive oxygen species via its thiol group. Functions as a cofactor for glu....
In what scenario might Carnosine be preferred?
For "Anti-Glycation and AGE Prevention," Carnosine may be more appropriate. Carnosine is a potent anti-glycation agent that directly inhibits AGE formation by competing with sugars for protein binding sites. Glutathione does not share this specific mechanism.. Individual factors and clinical context should guide any decisions.
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.