Afamelanotide vs Melanotan-1: Melanocortin Peptides Compared
Comparison of afamelanotide (Scenesse) and melanotan-1, the FDA-approved implant versus the research peptide -- both alpha-MSH analogs targeting MC1R for melanin production, but with vastly different regulatory status, delivery, and evidence.
Verdict at a Glance
Afamelanotide and melanotan-1 are the same molecule (Nle4-D-Phe7-alpha-MSH) with different names, regulatory statuses, and delivery systems. Afamelanotide (Scenesse) is the FDA-approved pharmaceutical formulation with proven safety and efficacy from Phase 3 clinical trials, delivered as a controlled-release subcutaneous implant. Melanotan-1 is the unregulated research peptide version available from non-pharmaceutical sources. For EPP patients, afamelanotide is the clearly superior choice as a proven, approved treatment. For individuals seeking tanning or photoprotection outside of EPP, melanotan-1 represents an unregulated alternative with identical pharmacology but unverified product quality and no medical oversight. The core comparison is not between different molecules but between pharmaceutical-grade and research-grade versions of the same peptide.
| Best for | Pick | Why |
|---|---|---|
| Erythropoietic Protoporphyria (EPP) | Afamelanotide | FDA-approved treatment with Phase 3 evidence demonstrating increased pain-free time in sunlight. Controlled-release implant provides consistent 60-day dosing. Only medically validated option for EPP. |
| Pharmaceutical-Grade Quality | Afamelanotide | GMP manufacturing, regulatory oversight, and consistent 16 mg dosing in a controlled-release implant. Research peptide melanotan-1 has variable quality and no regulatory standards. |
| Medical Supervision | Afamelanotide | Administered by healthcare providers with monitoring. Research peptide melanotan-1 is typically self-administered without medical oversight. |
| Cost Accessibility | Melanotan-1 | Research peptide melanotan-1 costs a fraction of pharmaceutical afamelanotide. However, this comes with quality uncertainty and no regulatory protection. |
| Non-EPP Photoprotection | Neither (insufficient evidence for either) | Afamelanotide is only approved for EPP. Melanotan-1 is not approved for any indication. Neither has robust evidence for general photoprotection or cosmetic tanning in healthy individuals. |
| Category | Afamelanotide | Melanotan-1 | Advantage |
|---|---|---|---|
| Molecular Identity | Afamelanotide is the pharmaceutical name for the same molecule originally developed as melanotan-1. It is a synthetic tridecapeptide analog of alpha-MSH with the substitution Nle4-D-Phe7, providing resistance to enzymatic degradation and extended biological activity. FDA-approved as Scenesse in a 16 mg subcutaneous implant formulation. | Melanotan-1 (MT-1) refers to the same base peptide sequence (Nle4-D-Phe7-alpha-MSH) as afamelanotide, but is sold as an unregulated research peptide in lyophilized powder form for subcutaneous injection. The name "melanotan-1" is used in the research peptide market, while "afamelanotide" is the INN (international nonproprietary name). | Comparable |
| Regulatory Status | FDA-approved (2019) as Scenesse for erythropoietic protoporphyria (EPP). EMA-approved (2014) for the same indication. First-in-class MC1R agonist. Administered only by healthcare providers as a subcutaneous implant. Classified as an orphan drug. | Not approved by any regulatory agency for any indication. Sold through research peptide suppliers without quality standardization or regulatory oversight. Quality, purity, and dosing accuracy vary significantly between suppliers. Used off-label by individuals for tanning and photoprotection. | Afamelanotide |
| Research Evidence | Extensive Phase 2 and Phase 3 clinical trial data in EPP, vitiligo, and other photodermatoses. Multiple randomized, placebo-controlled trials demonstrating increased pain-free time in sunlight for EPP patients. Published in peer-reviewed journals including NEJM and Lancet. | Clinical evidence is effectively the same as afamelanotide (same molecule). Early University of Arizona research used the name "melanotan-1." However, research peptide melanotan-1 products have not undergone independent clinical testing, and product quality cannot be assumed to match pharmaceutical-grade afamelanotide. | Afamelanotide |
| Safety Profile | Well-characterized safety profile from clinical trials. Common side effects include nausea, headache, injection site reactions, and skin darkening. Controlled-release implant provides consistent dosing, minimizing peak-related side effects. No cardiovascular or sexual side effects (unlike melanotan-2). | Safety profile theoretically similar (same molecule) but product quality concerns add risk. Self-injection introduces dosing errors and infection risk. No medical supervision. Potential for contamination or incorrect peptide from unregulated suppliers. Reports of nausea and injection site pain. | Afamelanotide |
| Accessibility and Cost | Available only by prescription for EPP patients. Extremely expensive (approximately $40,000-50,000 per implant in the US). Limited to a single approved indication. Not available for cosmetic tanning. Requires healthcare provider administration. | Widely available from research peptide suppliers at a fraction of pharmaceutical cost (typically $30-100 per vial). No prescription needed. Can be self-administered via subcutaneous injection. However, purchasing for human use is legally gray and product quality is unverified. | Melanotan-1 |

Introduction#
Afamelanotide and melanotan-1 present a unique comparison in the peptide world because they are the same molecule under different names and regulatory contexts. Both are synthetic analogs of alpha-melanocyte-stimulating hormone (alpha-MSH) with the amino acid substitutions Nle4 and D-Phe7, which confer resistance to enzymatic degradation and enhanced MC1R receptor binding.
The critical difference lies not in chemistry but in context: afamelanotide (marketed as Scenesse) is an FDA-approved pharmaceutical delivered as a controlled-release subcutaneous implant for erythropoietic protoporphyria (EPP), while melanotan-1 is the same peptide sold through unregulated research suppliers as a lyophilized powder for self-injection. This comparison examines the implications of these differences for safety, efficacy, and appropriate use.
The Same Molecule, Different Names#
Naming History#
The peptide was originally developed at the University of Arizona in the 1980s-1990s by Victor Hruby and Mac Hadley, who created the alpha-MSH analog [Nle4, D-Phe7]-alpha-MSH and named it "melanotan" (later distinguished as "melanotan-1" or "melanotan I" to differentiate it from the cyclic analog melanotan-2).
Clinuvel Pharmaceuticals licensed the peptide for pharmaceutical development and assigned the international nonproprietary name (INN) "afamelanotide." The peptide was developed as Scenesse, a 16 mg controlled-release subcutaneous implant.
Chemical Identity#
| Property | Afamelanotide | Melanotan-1 |
|---|---|---|
| Chemical name | [Nle4, D-Phe7]-alpha-MSH | [Nle4, D-Phe7]-alpha-MSH |
| Sequence | Ac-Ser-Tyr-Ser-Nle-Glu-His-D-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH2 | Same |
| Amino acids | 13 (tridecapeptide) | Same |
| Molecular weight | ~1,646 Da | Same |
| Target receptor | MC1R (primary) | Same |
| Mechanism | Stimulates eumelanin synthesis | Same |
The molecules are pharmacologically identical. The differences are entirely in formulation, manufacturing quality, delivery system, and regulatory status.
Formulation and Delivery Comparison#
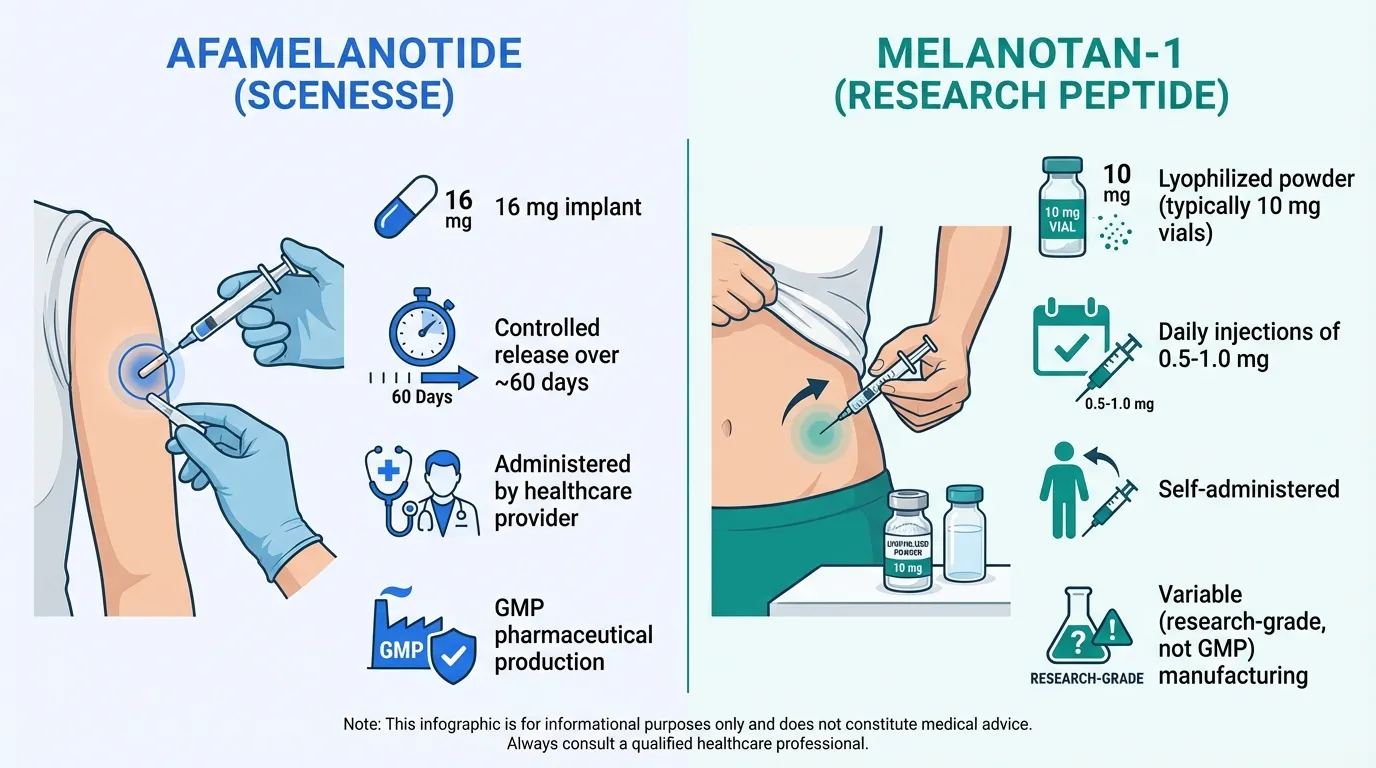
Afamelanotide (Scenesse)#
The pharmaceutical formulation uses a controlled-release bioresorbable implant:
| Feature | Details |
|---|---|
| Formulation | 16 mg subcutaneous implant |
| Delivery | Controlled release over ~60 days |
| Administration | By healthcare provider using implant applicator |
| Manufacturing | GMP pharmaceutical production (Clinuvel) |
| Quality assurance | FDA/EMA regulatory oversight |
| Storage | Controlled pharmaceutical storage |
| Frequency | Every 60 days (approximately) |
Melanotan-1 (Research Peptide)#
The research peptide version is sold as lyophilized powder:
| Feature | Details |
|---|---|
| Formulation | Lyophilized powder (typically 10 mg vials) |
| Delivery | Self-administered subcutaneous injection |
| Administration | Daily injections of 0.5-1.0 mg |
| Manufacturing | Variable (research-grade, not GMP) |
| Quality assurance | None (no regulatory oversight) |
| Storage | Refrigerated after reconstitution |
| Frequency | Daily during loading, then periodic maintenance |
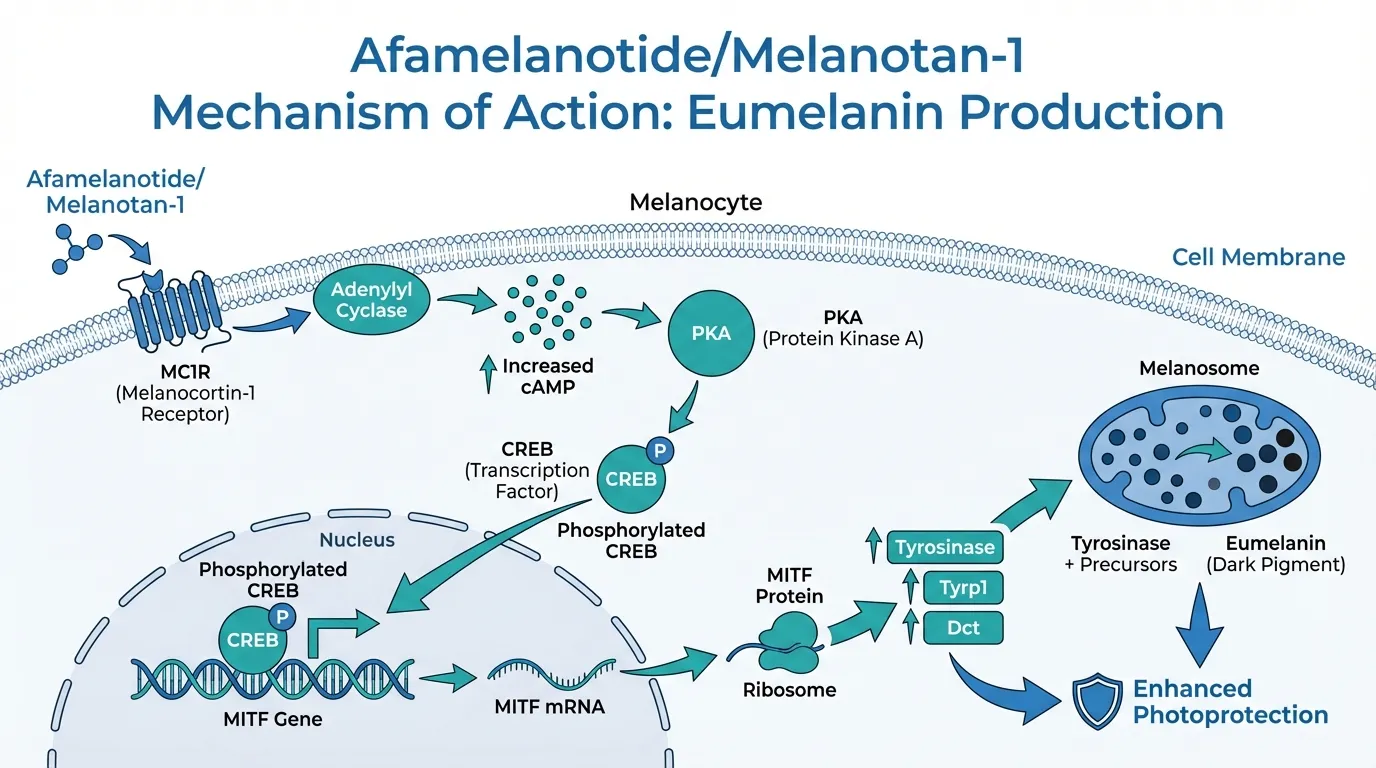
Mechanism of Action#
Both afamelanotide and melanotan-1 share the same mechanism:
- MC1R binding: The peptide binds to melanocortin-1 receptors (MC1R) on melanocytes with high affinity and longer duration than native alpha-MSH
- Adenylyl cyclase activation: MC1R activation stimulates adenylyl cyclase, increasing intracellular cAMP
- PKA/CREB pathway: cAMP activates protein kinase A, which phosphorylates CREB transcription factor
- MITF induction: CREB activates the MITF gene, the master regulator of melanocyte function
- Eumelanin synthesis: MITF upregulates tyrosinase and other enzymes in the eumelanin biosynthetic pathway
- Photoprotection: Increased eumelanin provides UV absorption and free radical scavenging
The key distinction from alpha-MSH is the substitutions at positions 4 (norleucine replaces methionine) and 7 (D-phenylalanine replaces L-phenylalanine), which increase metabolic stability from minutes to hours.
Selectivity vs Melanotan-2#
Unlike melanotan-2 (MT-2), both afamelanotide and melanotan-1 are highly selective for MC1R:
| Property | Afamelanotide/MT-1 | Melanotan-2 |
|---|---|---|
| MC1R activity | Strong agonist | Strong agonist |
| MC3R activity | Minimal | Moderate |
| MC4R activity | Minimal | Strong |
| MC5R activity | Minimal | Moderate |
| Sexual side effects | Not reported | Common (MC4R) |
| Appetite effects | Not reported | Possible (MC4R) |
This MC1R selectivity means afamelanotide/MT-1 produces tanning and photoprotection without the sexual arousal, appetite suppression, or cardiovascular effects associated with melanotan-2.
Clinical Evidence#
Afamelanotide Clinical Trials#
Multiple Phase 2 and Phase 3 trials have evaluated afamelanotide:
EPP Phase 3 (CUV039): Randomized, double-blind, placebo-controlled trial in 93 EPP patients. Afamelanotide significantly increased the median duration of pain-free direct sunlight exposure from 10 minutes (placebo) to 70 minutes (treatment) over 6 months.
EPP Phase 3 (CUV017): Confirmatory trial in 74 patients demonstrating significant increases in light exposure time and quality of life measures.
Vitiligo Phase 2: Studies showed acceleration of repigmentation when afamelanotide was combined with narrowband UVB phototherapy. Repigmentation rates were faster and more extensive compared to NB-UVB alone.
Melanotan-1 Research#
Because melanotan-1 is the same molecule, the University of Arizona's original human studies technically constitute evidence for both:
Dorr et al. (early studies): Demonstrated increased melanin density and tanning in human subjects after subcutaneous injections of [Nle4, D-Phe7]-alpha-MSH.
However, no clinical trials have been conducted using commercially available research-grade melanotan-1 products. The pharmaceutical-grade evidence applies to the molecule but not to the variable-quality products sold through research suppliers.
Side Effects Comparison#
Afamelanotide Side Effects (from clinical trials)#
| Side Effect | Frequency | Notes |
|---|---|---|
| Implant site reactions | Common | Bruising, pain, redness at insertion site |
| Nausea | Common | Usually transient |
| Headache | Common | Mild |
| Skin darkening | Expected | Pharmacological effect (eumelanin increase) |
| Mole darkening | Occasional | Existing nevi may darken |
| Fatigue | Occasional | Mild |
| Oropharyngeal pain | Occasional | Mild |
Melanotan-1 Side Effects (reported from unregulated use)#
| Side Effect | Frequency | Notes |
|---|---|---|
| Nausea | Common | May be more pronounced with rapid injection |
| Injection site pain | Common | Self-injection related |
| Headache | Common | Similar to afamelanotide |
| Skin darkening | Expected | Same pharmacological effect |
| Flushing | Occasional | After injection |
| Fatigue | Occasional | Similar to afamelanotide |
| Infection risk | Variable | Self-injection without sterile technique |
| Unknown contaminants | Possible | No quality assurance on research products |
Regulatory and Legal Status#
| Jurisdiction | Afamelanotide | Melanotan-1 |
|---|---|---|
| United States | FDA-approved (Scenesse) for EPP | Not approved; sold as "research chemical" |
| European Union | EMA-approved for EPP | Not approved; sale for human use is illegal |
| Australia | TGA-approved for EPP | Not approved; classified as Schedule 4 |
| International | Approved in multiple countries for EPP | Not approved anywhere; legal status varies |
Key Differences Summary#
- Same molecule: Afamelanotide and melanotan-1 are pharmacologically identical -- [Nle4, D-Phe7]-alpha-MSH.
- Different quality: Afamelanotide is GMP pharmaceutical grade; melanotan-1 is research grade with variable quality.
- Different delivery: Afamelanotide uses a controlled-release 60-day implant; melanotan-1 requires daily subcutaneous injections.
- Different oversight: Afamelanotide is prescribed and administered by healthcare providers; melanotan-1 is self-administered without medical supervision.
- Different cost: Afamelanotide costs approximately $40,000-50,000 per implant; melanotan-1 costs $30-100 per vial.
- Different indication: Afamelanotide is approved for EPP; melanotan-1 is used off-label for tanning.
- Same selectivity: Both are MC1R-selective without the MC4R-mediated sexual and appetite effects of melanotan-2.
Conclusion#
The afamelanotide vs melanotan-1 comparison is not a comparison of different molecules but of the same molecule in two very different contexts. For patients with erythropoietic protoporphyria, afamelanotide (Scenesse) is a proven, FDA-approved treatment that should be obtained through proper medical channels. For individuals using melanotan-1 from research suppliers for cosmetic tanning, they are using a pharmaceutical-grade molecule from non-pharmaceutical sources, accepting the risks of variable product quality, self-injection, and absence of medical oversight.
The comparison highlights an important broader principle: the safety and efficacy of a peptide depend not only on its molecular identity but also on its manufacturing quality, formulation, delivery system, and medical supervision. The same molecule can be a validated treatment (afamelanotide) or an unregulated product of uncertain quality (research melanotan-1) depending on its source and context of use.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Erythropoietic Protoporphyria (EPP)
Afamelanotide
FDA-approved treatment with Phase 3 evidence demonstrating increased pain-free time in sunlight. Controlled-release implant provides consistent 60-day dosing. Only medically validated option for EPP.
Pharmaceutical-Grade Quality
Afamelanotide
GMP manufacturing, regulatory oversight, and consistent 16 mg dosing in a controlled-release implant. Research peptide melanotan-1 has variable quality and no regulatory standards.
Medical Supervision
Afamelanotide
Administered by healthcare providers with monitoring. Research peptide melanotan-1 is typically self-administered without medical oversight.
Cost Accessibility
Melanotan-1
Research peptide melanotan-1 costs a fraction of pharmaceutical afamelanotide. However, this comes with quality uncertainty and no regulatory protection.
Non-EPP Photoprotection
Neither (insufficient evidence for either)
Afamelanotide is only approved for EPP. Melanotan-1 is not approved for any indication. Neither has robust evidence for general photoprotection or cosmetic tanning in healthy individuals.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Afamelanotide vs Melanotan-1: Melanocortin Peptides Compared
Which is better, Afamelanotide or Melanotan-1?
Afamelanotide and melanotan-1 are the same molecule (Nle4-D-Phe7-alpha-MSH) with different names, regulatory statuses, and delivery systems. Afamelanotide (Scenesse) is the FDA-approved pharmaceutical formulation with proven safety and efficacy from Phase 3 clinical trials, delivered as a controlled-release subcutaneous implant. Melanotan-1 is the unregulated research peptide version available from non-pharmaceutical sources. For EPP patients, afamelanotide is the clearly superior choice as a... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Afamelanotide and Melanotan-1?
The main differences across comparison categories are: Molecular Identity: advantage goes to neither (tie); Regulatory Status: advantage goes to Afamelanotide; Research Evidence: advantage goes to Afamelanotide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Afamelanotide over Melanotan-1?
For the scenario of "Erythropoietic Protoporphyria (EPP)," research data suggests Afamelanotide may be more relevant. FDA-approved treatment with Phase 3 evidence demonstrating increased pain-free time in sunlight. Controlled-release implant provides consistent 60-day dosing. Only medically validated option for EPP.. This is based on currently available evidence and individual circumstances may differ.
Which has fewer side effects, Afamelanotide or Melanotan-1?
In terms of side effects and tolerability, the advantage goes to Afamelanotide. Afamelanotide: Well-characterized safety profile from clinical trials. Common side effects include nausea, headache, injection site reactions, and skin darkening..... Melanotan-1: Safety profile theoretically similar (same molecule) but product quality concerns add risk. Self-injection introduces dosing errors and infection r....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.