Cerebrolysin vs Davunetide: Neuroprotective Peptides Compared
Evidence-based comparison of cerebrolysin and davunetide (NAP/AL-108), two neuroprotective peptide therapies -- a porcine brain-derived peptide mixture approved for stroke versus a synthetic ADNP-derived octapeptide tested in tauopathies.
Verdict at a Glance
Cerebrolysin has the stronger overall evidence base and broader clinical validation, with approval in over 30 countries for stroke and TBI, multiple randomized controlled trials, and extensive clinical experience spanning decades. Davunetide has an elegant mechanism targeting microtubule stability and tau-mediated neurodegeneration, with an exceptionally benign safety profile, but its clinical development was hampered by the failure to meet the primary endpoint in the PSP Phase 2/3 trial. For acute neurological injury (stroke, TBI), cerebrolysin has far more evidence. For tauopathies specifically, davunetide showed promise in subgroups but failed overall. Both peptides are well-tolerated, but cerebrolysin's broader evidence base and international regulatory acceptance give it the advantage for most neuroprotective applications.
| Best for | Pick | Why |
|---|---|---|
| Acute Stroke Recovery | Cerebrolysin | The CARS trial demonstrated significant improvement in arm function at day 90 with 30 mL/day IV for 21 days. A 2025 study showed significant NIHSS improvement in acute ischemic stroke. Approved in many countries for this indication. |
| Traumatic Brain Injury | Cerebrolysin | Multiple clinical trials and regulatory approvals for TBI across international markets. Standard of care in some countries for acute TBI neurorecovery. Davunetide has not been studied in TBI. |
| Tauopathies (PSP, FTD) | Neither (insufficient efficacy data) | Davunetide's PSP Phase 2/3 trial failed its primary endpoint despite showing benefit in women subgroup. Cerebrolysin has not been specifically studied in PSP or FTD. Neither has proven efficacy for tauopathies. |
| Non-Invasive Administration | Davunetide | Intranasal delivery provides brain penetration without IV access. Cerebrolysin requires IV infusion or IM injection in clinical settings. |
| Safety-First Approach | Davunetide | Side effects virtually indistinguishable from placebo in the PSP trial. Cerebrolysin is also well-tolerated but carries risk of porcine protein allergy and requires invasive administration. |
| Alzheimer's Disease | Cerebrolysin | Multiple small clinical trials show modest cognitive improvements in Alzheimer's patients. Davunetide was studied in MCI and schizophrenia cognition but not specifically in Alzheimer's disease. |
| Category | Cerebrolysin | Davunetide | Advantage |
|---|---|---|---|
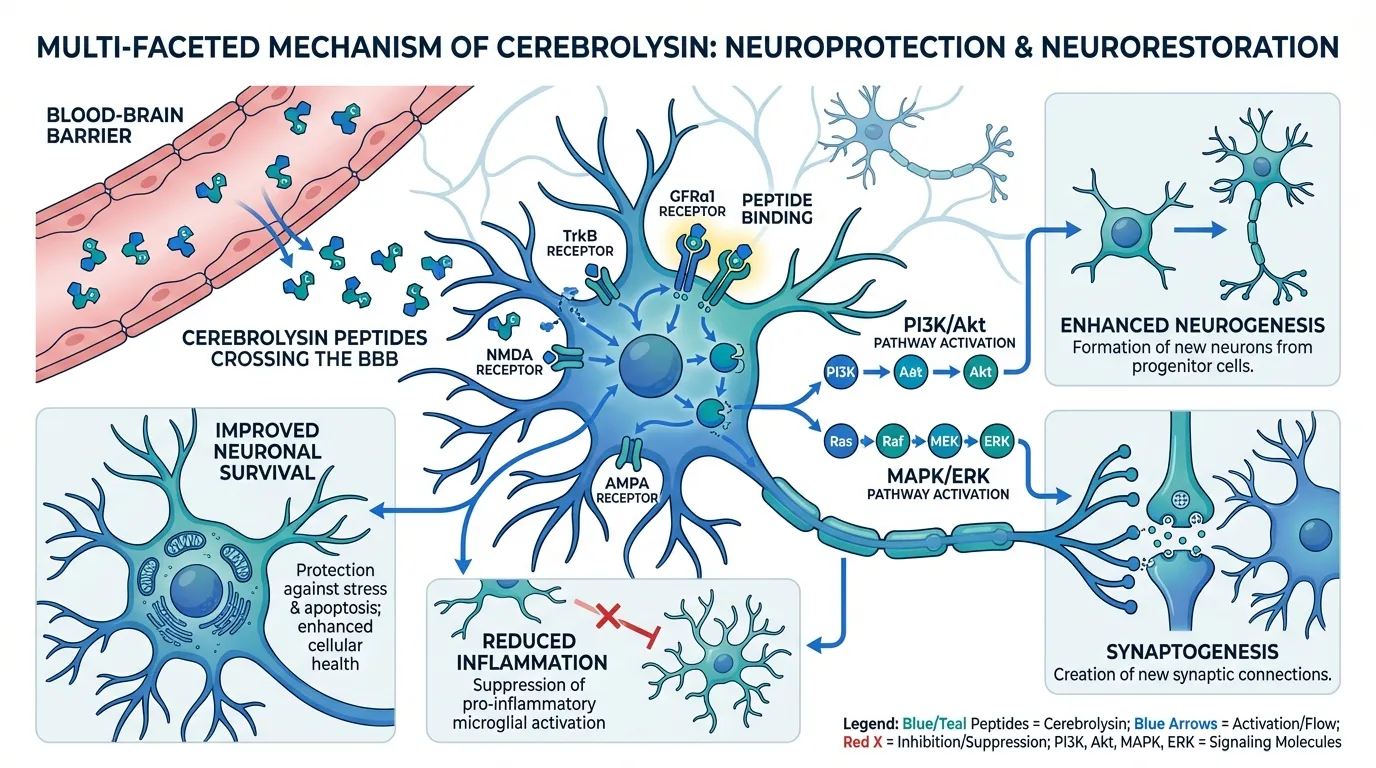
| Mechanism of Action | Cerebrolysin is a mixture of low molecular weight neuropeptides and free amino acids derived from porcine brain tissue. It mimics the effects of neurotrophic factors (NGF, BDNF, CNTF) by activating PI3K/Akt and MAPK/ERK signaling pathways. It promotes neurogenesis, synaptogenesis, and neuronal survival while reducing neuroinflammation and apoptosis. Crosses the blood-brain barrier. | Davunetide (NAP, NAPVSIPQ) is a synthetic octapeptide derived from activity-dependent neuroprotective protein (ADNP). It stabilizes microtubules by interacting with tubulin, protecting neurons from tau-mediated toxicity. It also has antioxidant and anti-inflammatory properties and promotes microtubule dynamics essential for axonal transport and synaptic function. | Comparable |
| Research Evidence | Cerebrolysin has extensive clinical trial data across stroke, TBI, Alzheimer's disease, and vascular dementia. The CARS trial showed significant improvement in arm function after stroke. Multiple RCTs with hundreds of patients. Approved in >30 countries (not FDA-approved). A 2025 study showed NIHSS improvement in acute ischemic stroke. | Davunetide showed promise in Phase 2 for progressive supranuclear palsy (PSP), with significant disease slowing in women. However, the Phase 2/3 trial in PSP (n=313) did not meet its primary endpoint overall. Intranasal formulation showed good brain penetration and safety. No approved indications. Development has been largely discontinued for PSP but continues for other applications. | Cerebrolysin |
| Side Effect Profile | Generally well-tolerated in clinical trials. Common side effects include injection site reactions, dizziness, headache, and mild agitation. IV infusion is well-tolerated at standard doses (30 mL/day). No significant safety concerns in meta-analyses. Risk of allergic reaction to porcine proteins exists. | Exceptionally well-tolerated. In the PSP Phase 2/3 trial, side effects were virtually indistinguishable from placebo. Intranasal administration is non-invasive and well-accepted. No serious treatment-related adverse events reported. One of the safest neuroprotective agents tested. | Davunetide |
| Administration | Intravenous infusion or intramuscular injection. Standard dose is 30 mL IV daily for 10-21 days in acute stroke/TBI. Lower doses (5-10 mL IM) for cognitive conditions. Requires clinical setting for IV administration. Not available orally or intranasally. | Intranasal administration (primary route in clinical trials). Non-invasive spray delivery provides good brain penetration. Oral formulation was being explored. No IV required. More practical for chronic use in neurodegenerative disease. | Davunetide |
| Indications and Scope | Broad neuroprotective applications including acute ischemic stroke, traumatic brain injury, Alzheimer's disease, vascular dementia, Parkinson's disease, and ALS. Approved in >30 countries for stroke and TBI. Most extensive clinical data in acute stroke and neurorecovery. | Primarily investigated for tauopathies (progressive supranuclear palsy, frontotemporal dementia) and cognitive impairment. Microtubule-stabilizing mechanism is particularly relevant to tau-mediated neurodegeneration. Also studied for schizophrenia-related cognitive deficits and mild cognitive impairment. | Cerebrolysin |

Introduction#
Cerebrolysin and davunetide represent two distinct approaches to neuroprotection: cerebrolysin is a complex mixture of porcine brain-derived peptides that broadly mimics neurotrophic factor signaling, while davunetide is a precisely defined synthetic octapeptide that stabilizes microtubules to protect against tau-mediated neurodegeneration. Both have been tested in clinical trials for neurological conditions, but with very different levels of success and regulatory acceptance.
Cerebrolysin is approved in over 30 countries for stroke and traumatic brain injury, making it one of the most widely used neuropeptide therapies globally (though notably not FDA-approved in the United States). Davunetide showed initial promise in tauopathies but its development was hindered by a pivotal trial that failed to meet its primary endpoint. This comparison examines their mechanisms, evidence, and clinical utility.
Mechanism of Action Comparison#
Cerebrolysin#
Cerebrolysin is a standardized mixture of low molecular weight neuropeptides (<10 kDa) and free amino acids derived from enzymatic proteolysis of porcine brain proteins. Its composition is complex but reproducible, containing peptide fragments that mimic the actions of multiple neurotrophic factors:
- Neurotrophic factor mimicry: Activates signaling pathways normally triggered by NGF, BDNF, GDNF, and CNTF
- PI3K/Akt pathway: Promotes neuronal survival by activating anti-apoptotic signaling
- MAPK/ERK signaling: Stimulates neuronal differentiation and synaptic plasticity
- Neurogenesis: Promotes generation of new neurons in the hippocampus and subventricular zone
- Synaptogenesis: Enhances formation of new synaptic connections
- Anti-inflammatory: Reduces neuroinflammatory cytokines and microglial activation
- Blood-brain barrier penetration: The low molecular weight of cerebrolysin peptides allows significant BBB crossing
Davunetide#
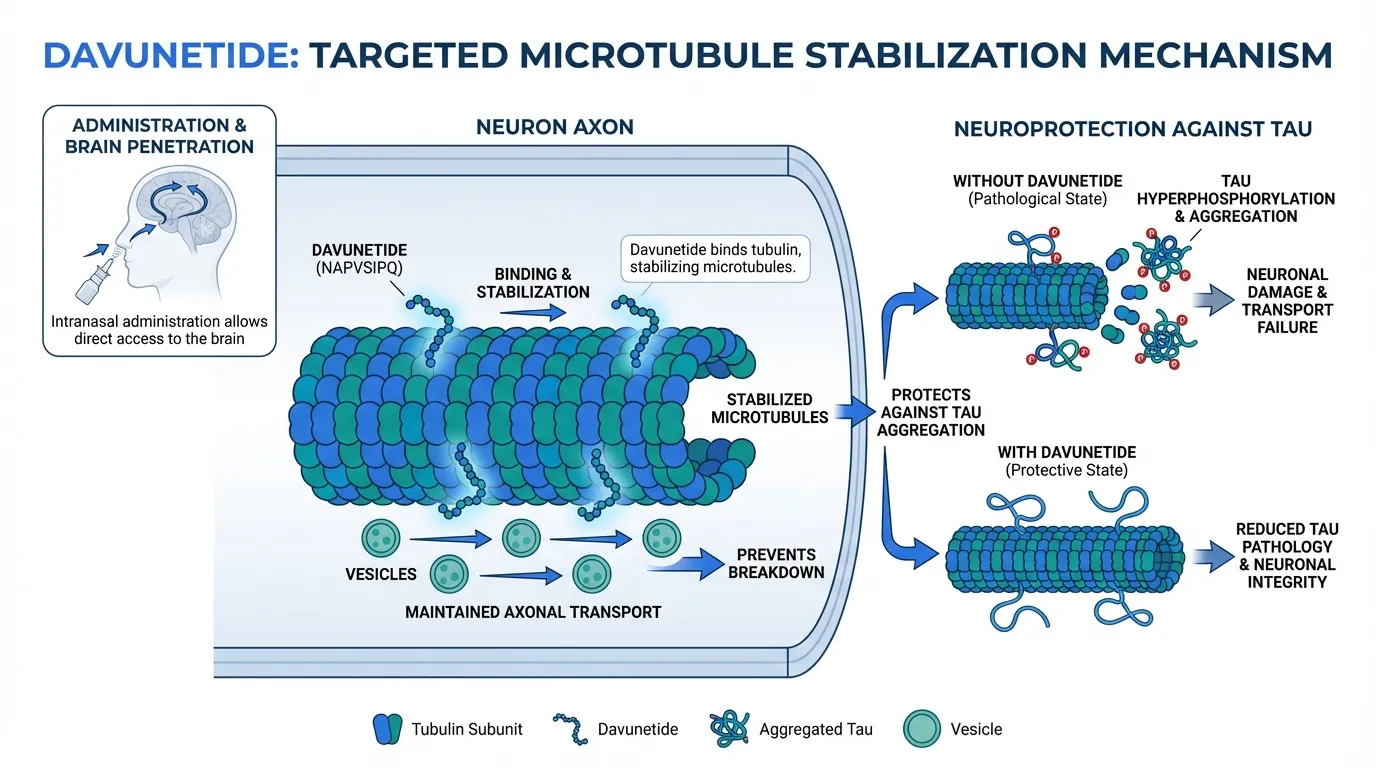
Davunetide (NAP, AL-108) is a synthetic octapeptide (NAPVSIPQ) derived from the most active fragment of activity-dependent neuroprotective protein (ADNP). ADNP is essential for brain development, and mutations in the ADNP gene cause the ADNP syndrome. Davunetide's mechanism is more targeted:
- Microtubule stabilization: Directly interacts with tubulin to stabilize microtubule dynamics, which are disrupted in tauopathies
- Tau interaction: Protects against tau hyperphosphorylation and aggregation, preserving cytoskeletal integrity
- Axonal transport: By maintaining microtubule stability, preserves the axonal transport systems critical for synaptic function
- Antioxidant effects: Reduces oxidative stress in neuronal cells
- Anti-inflammatory: Modulates inflammatory pathways in the CNS
- Intranasal brain penetration: Designed for intranasal delivery with direct CNS access via the olfactory pathway
Mechanistic Comparison#
| Feature | Cerebrolysin | Davunetide |
|---|---|---|
| Composition | Mixture of porcine peptides + amino acids | Single defined octapeptide |
| Molecular weight | <10 kDa (mixture) | ~824 Da |
| Primary mechanism | Neurotrophic factor mimicry | Microtubule stabilization |
| Target specificity | Broad (multiple pathways) | Focused (tubulin/microtubules) |
| Neurogenesis | Yes | Not primary effect |
| Synaptogenesis | Yes | Indirect (via microtubule health) |
| Anti-inflammatory | Yes | Yes |
| Tau-specific protection | Not primary | Primary mechanism |
| BBB penetration | Yes (low MW peptides) | Yes (intranasal route) |
Clinical Evidence Comparison#
Cerebrolysin Research#
Cerebrolysin has extensive clinical trial data:
CARS Trial (Stroke): Randomized, placebo-controlled trial of cerebrolysin 30 mL/day IV for 21 days in acute stroke. Demonstrated large superiority over placebo on the Action Research Arm Test at day 90 (Mann-Whitney estimator 0.71, 95% CI 0.63-0.79, p<0.0001).
2025 Acute Ischemic Stroke Study: Adjuvant therapy with cerebrolysin 30 mL IV daily for 14 days showed significantly greater NIHSS reductions (9.90 to 3.40) compared to standard care alone (10.10 to 4.80, p<0.001).
CLINCH Trial (2025): Frontiers in Neurology published results from a pilot trial evaluating cerebrolysin safety and feasibility in primary intracerebral hemorrhage.
Alzheimer's Disease: Multiple small trials showing modest improvements in cognitive function scores with 30 mL IV for 20 days.
ALS: A 2024 Phase 2 trial showed that add-on cerebrolysin improved clinical symptoms in ALS patients.
Evidence level: Moderate -- multiple RCTs, international approval, but not FDA-approved. Some meta-analyses show modest effects.
Davunetide Research#
Davunetide's clinical development has been mixed:
PSP Phase 2/3 (n=313): The largest trial of davunetide was a randomized, double-blind, placebo-controlled study in progressive supranuclear palsy. The trial did not meet its primary endpoint (change in PSP Rating Scale). However, a subgroup analysis showed significant disease slowing in women.
Intranasal bioavailability: Studies demonstrated that intranasal davunetide achieves significant brain concentrations and is well-tolerated.
Schizophrenia cognition: Showed some improvement in cognitive measures in schizophrenia patients.
MCI/Alzheimer's: Early-phase studies showed signals of cognitive benefit but were not advanced to larger trials.
2025 circadian rhythm study: A recent ScienceDirect publication examined intranasal davunetide's effects on neuroprotection and circadian rhythmicity, suggesting ongoing research interest.
Evidence level: Low to moderate -- one large Phase 2/3 trial that failed, limited positive signals in subgroups.
Evidence Comparison Table#
| Feature | Cerebrolysin | Davunetide |
|---|---|---|
| Largest trial | CARS (stroke, significant) | PSP Phase 2/3 (n=313, failed primary) |
| Total clinical subjects | Thousands across trials | ~500 across trials |
| Positive Phase 3 data | Yes (CARS, stroke) | No (PSP trial failed overall) |
| Regulatory approval | 30+ countries (not USA) | None |
| Indications studied | Stroke, TBI, AD, VD, PD, ALS | PSP, schizophrenia, MCI |
| Meta-analyses | Available (mixed quality) | Limited |
Dosing Comparison#
Cerebrolysin Dosing#
| Parameter | Acute Stroke/TBI | Cognitive/Dementia |
|---|---|---|
| Dose | 30 mL IV daily | 5-10 mL IM or 10-30 mL IV |
| Route | Intravenous infusion | IM or IV |
| Duration | 10-21 days | 20-30 day cycles |
| Frequency | Once daily | Once daily |
| Setting | Hospital/clinical | Hospital or outpatient |
| Repeat cycles | As needed per clinical course | Every 3-6 months |
Davunetide Dosing#
| Parameter | Details |
|---|---|
| Dose | 15-30 mg intranasal twice daily |
| Route | Intranasal spray |
| Duration | Chronic (months in PSP trial) |
| Frequency | Twice daily |
| Setting | Home-based (self-administered) |
| Repeat cycles | Continuous treatment |
Side Effects Comparison#
Cerebrolysin Side Effects#
| Side Effect | Frequency | Notes |
|---|---|---|
| Injection site reactions | Common | IV infusion-related |
| Dizziness | Occasional | Mild, transient |
| Headache | Occasional | Mild |
| Agitation | Occasional | More common in TBI patients |
| Nausea | Rare | Mild |
| Allergic reaction | Rare | Porcine protein allergy risk |
| Fever | Rare | Mild |
Davunetide Side Effects#
| Side Effect | Frequency | Notes |
|---|---|---|
| Nasal irritation | Occasional | Related to intranasal delivery |
| Headache | Rare | Mild |
| Fatigue | Rare | Mild |
| Serious AEs | None reported | Side effects indistinguishable from placebo |
Davunetide has one of the best safety profiles of any neuroprotective agent tested in clinical trials, with adverse event rates virtually identical to placebo.
Key Differences Summary#
- Composition: Cerebrolysin is a complex peptide mixture; davunetide is a single defined peptide.
- Mechanism: Cerebrolysin broadly mimics neurotrophic factors; davunetide specifically stabilizes microtubules.
- Clinical success: Cerebrolysin has positive RCTs in stroke and international approval; davunetide failed its pivotal PSP trial.
- Administration: Cerebrolysin requires IV infusion; davunetide uses non-invasive intranasal delivery.
- Safety: Both are well-tolerated, but davunetide's safety profile is exceptional (placebo-like).
- Availability: Cerebrolysin is commercially available in many countries; davunetide is primarily a research compound.
- FDA status: Neither is FDA-approved. Cerebrolysin is approved in 30+ other countries; davunetide is not approved anywhere.
- Disease specificity: Cerebrolysin is broadly neuroprotective; davunetide specifically targets tau/microtubule pathology.
Conclusion#
Cerebrolysin and davunetide represent different generations and philosophies of neuroprotective therapy. Cerebrolysin is the more established agent, with decades of clinical use, approval in over 30 countries, and positive randomized controlled trials in acute stroke. Its broad neurotrophic mechanism makes it applicable across multiple neurological conditions, though its complex composition and IV administration are practical limitations.
Davunetide has an elegant and targeted mechanism -- stabilizing the microtubule network that underlies neuronal structure and function. Its intranasal delivery, exceptional safety profile, and tau-specific mechanism made it a compelling candidate for tauopathies. However, the failure of the pivotal PSP Phase 2/3 trial significantly limited its clinical development, despite intriguing signals in the female subgroup.
For acute neurological injury (stroke, TBI), cerebrolysin has far more evidence and is the clearly established option. For chronic neurodegenerative conditions, particularly tauopathies, neither agent has definitively proven efficacy. The field continues to need better neuroprotective agents, and both compounds have contributed valuable insights into different approaches to protecting and restoring neural function.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Acute Stroke Recovery
Cerebrolysin
The CARS trial demonstrated significant improvement in arm function at day 90 with 30 mL/day IV for 21 days. A 2025 study showed significant NIHSS improvement in acute ischemic stroke. Approved in many countries for this indication.
Traumatic Brain Injury
Cerebrolysin
Multiple clinical trials and regulatory approvals for TBI across international markets. Standard of care in some countries for acute TBI neurorecovery. Davunetide has not been studied in TBI.
Tauopathies (PSP, FTD)
Neither (insufficient efficacy data)
Davunetide's PSP Phase 2/3 trial failed its primary endpoint despite showing benefit in women subgroup. Cerebrolysin has not been specifically studied in PSP or FTD. Neither has proven efficacy for tauopathies.
Non-Invasive Administration
Davunetide
Intranasal delivery provides brain penetration without IV access. Cerebrolysin requires IV infusion or IM injection in clinical settings.
Safety-First Approach
Davunetide
Side effects virtually indistinguishable from placebo in the PSP trial. Cerebrolysin is also well-tolerated but carries risk of porcine protein allergy and requires invasive administration.
Alzheimer's Disease
Cerebrolysin
Multiple small clinical trials show modest cognitive improvements in Alzheimer's patients. Davunetide was studied in MCI and schizophrenia cognition but not specifically in Alzheimer's disease.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Cerebrolysin vs Davunetide: Neuroprotective Peptides Compared
Which is better, Cerebrolysin or Davunetide?
Cerebrolysin has the stronger overall evidence base and broader clinical validation, with approval in over 30 countries for stroke and TBI, multiple randomized controlled trials, and extensive clinical experience spanning decades. Davunetide has an elegant mechanism targeting microtubule stability and tau-mediated neurodegeneration, with an exceptionally benign safety profile, but its clinical development was hampered by the failure to meet the primary endpoint in the PSP Phase 2/3 trial. For... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Cerebrolysin and Davunetide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to Cerebrolysin; Side Effect Profile: advantage goes to Davunetide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Cerebrolysin over Davunetide?
For the scenario of "Acute Stroke Recovery," research data suggests Cerebrolysin may be more relevant. The CARS trial demonstrated significant improvement in arm function at day 90 with 30 mL/day IV for 21 days. A 2025 study showed significant NIHSS improvement in acute ischemic stroke. Approved in .... This is based on currently available evidence and individual circumstances may differ.
How do Cerebrolysin and Davunetide differ in their mechanisms of action?
Cerebrolysin: Cerebrolysin is a mixture of low molecular weight neuropeptides and free amino acids derived from porcine brain tissue. It mimics the effects of neurotrophic factors (NGF, BDNF, CNTF) by activating.... Davunetide: Davunetide (NAP, NAPVSIPQ) is a synthetic octapeptide derived from activity-dependent neuroprotective protein (ADNP). It stabilizes microtubules by interacting with tubulin, protecting neurons from....
Which has fewer side effects, Cerebrolysin or Davunetide?
In terms of side effects and tolerability, the advantage goes to Davunetide. Cerebrolysin: Generally well-tolerated in clinical trials. Common side effects include injection site reactions, dizziness, headache, and mild agitation. IV infu.... Davunetide: Exceptionally well-tolerated. In the PSP Phase 2/3 trial, side effects were virtually indistinguishable from placebo. Intranasal administration is ....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.